Abstract
The rates of posttraumatic stress syndrome (PTSD) are high among refugee populations. At the same time, evidence is emerging of intergenerational transmission of psychopathology. The objective of this study was to examine the current knowledge on risk and protective factors for adverse mental health outcomes in the non-exposed offspring of trauma-affected refugees. A systematic search was undertaken from 1 January 1981 to 5 February 2021 (PubMed, Embase, PSYCInfo). Studies were included if they reported on families of trauma-exposed refugee parents and mental health outcomes in their non-exposed children. The search yielded 1415 results and twelve articles met inclusion criteria. The majority of studies emphasized the negative effects of parental mental health symptoms. There was substantial evidence of an association between parental PTSD and increased risk of psychological problems in offspring. Parenting style was identified as both a potential risk and protective factor. Risk/protective factors at the individual and family level were identified, but findings were inconclusive due to sample sizes and study designs. There is a need for evidence-based interventions aimed at improving child outcomes, especially by improving parental mental health and reinforcing parenting skills. Future research should aim to incorporate broader aspects of child development.
1. Introduction
According to UNHCR, there are more than 79.5 million displaced people worldwide, of which 26 million are refugees (United Nations High Commissioner for Refugees, 2020). In addition to this, many former refugees have resettled in new countries. The rates of posttraumatic stress disorder (PTSD) and other mental illnesses among refugee populations are high and persistent (Blackmore et al., 2020). A recent meta-analysis found that 1 out of 3 adult refugees resettled in Western countries has diagnosable PTSD and/or depression, while self-reported rates are even higher (Henkelmann et al., 2020). Earlier findings from systematic reviews have ranged from a prevalence of 9% for diagnosed PTSD and 5% for major depression (Fazel et al., 2005) to 30% for PTSD and 31% for depression (Steel et al., 2009). While early research on mental health among refugees primarily focused on the effects of exposure to war-related trauma, in recent years, focus has shifted to including the ongoing stressors associated with resettlement (Miller and Rasmussen, 2017).
At the same time, there is emerging evidence of adverse psychological and biological outcomes in children of trauma-affected parents (Leen-Feldner et al., 2013). The concept of intergenerational trauma transmission developed primarily in Holocaust studies and refers to the way trauma exposure affects the subsequent generations (Dekel and Goldblatt, 2008). Studies of the adult offspring of Holocaust survivors have identified an association between parental PTSD and offspring PTSD (Yehuda et al., 2001). The offspring sequelae related to parental PTSD symptoms are numerous and include depression, behavioral problems, biological alterations, and even elevated posttraumatic stress symptoms when children were not exposed themselves (Leen-Feldner et al., 2013). Maternal PTSD has been identified as a stronger predictor of negative child outcomes than paternal PTSD and furthermore, there seems to be a “dose-response effect” meaning an association between PTSD symptom levels and child outcomes (Leen-Feldner et al., 2013). Among war veterans, the severity of combat exposure and severity of PTSD symptoms, especially the emotional detachment component, was associated with greater child distress (Dekel and Goldblatt, 2008). In addition to negative child outcomes, parental exposure to traumatic events is linked to compromised relational patterns between parents and their children (van Ee et al., 2016a).
Generally, four mechanisms have been proposed to impact the intergenerational transmission of psychopathology: (epi)genetics, prenatal exposure, environmental stressors and parenting (Goodman et al., 2020). While the psychosocial mechanisms of trauma transmission have been established in numerous studies, the biological aspects remain largely unexplored apart from findings indicating offspring altered hypothalamic-pituitary-adrenal axis function (Leen-Feldner et al., 2013; Yehuda and Lehrner, 2018). Meanwhile, there is substantial evidence that parenting functions as a mediator between parental depression and child functioning – in both positive and negative directions (Goodman et al., 2020). Child development takes place in a dynamic and changing social environment which includes socioeconomic status, stressful life events, and social relationships (Gilman and Marden, 2013). The development of psychopathology in children is equally complex, and broader social-ecological factors influence the development of mental health issues (Bronfenbrenner, 1977; Williams, 2010). In order to understand and promote resilience, it is therefore important to identify not only risk factors, but also protective factors present in the family, social, or school environment (Daud et al., 2008).
Two previous reviews have sought to investigate trauma transmission between refugee parents and their non-exposed children, both focusing on the mechanisms of intergenerational transmission. Sangalang et al. (2017) included 20 articles and described a heterogeneous body of literature with many studies relying on the accounts of adult offspring, and concluded that family interactions and parenting play a significant role in the way trauma is processed in refugee families. Flanagan et al. (2020)included 8 studies and found that the parental trauma exposure and sequalae affect the children negatively, possibly via mechanisms of insecure attachment and family dysfunction. They argued that there is a need for a more thorough examination of the effects of contextual factors on trauma transmission which is what this review sets out to do (Flanagan et al., 2020).
In refugee populations, recent research has highlighted why a focus on children of refugees is warranted. Children of trauma-affected refugees are at increased risk of adverse psychological effects, highlighted by solid evidence of higher rates of mental illness among children of parents with PTSD (Back Nielsen et al., 2019). Additionally, a recent cohort study found that refugee parents’ trauma exposure and postmigration stressors are associated with elevated PTSD symptoms, and in turn, more psychological and behavioral problems in children (Bryant et al., 2018).
For these reasons, it is imperative to focus on aspects related to the development of psychopathology in this group of children. Thus, the aim of this review is to identify risk and protective factors for adverse mental health outcomes in children of trauma-affected refugees. The current review seeks to broaden the scope of previous reviews (Flanagan et al., 2020; Sangalang and Vang, 2017) focusing mainly on interpersonal mechanisms of trauma transmission by searching to identify both risk and protective factors, including interpersonal as well as contextual factors for the development of mental health problems.
2. Methods
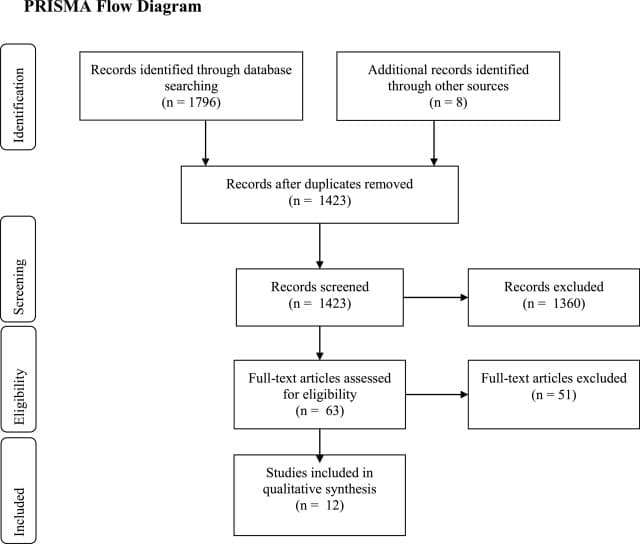
A review of the literature was conducted using the databases of PubMed, Embase and PSYCInfo on February 5th 2021 to identify original research publications from the past 40 years (1981 to present). The search included the following terms: [PTSD, PTSS, posttraumatic stress, intergenerational trauma, trauma transmission, historical trauma], [child, adolescent, teenager, intergenerational, transgenerational, second-generation], [refugee*, displaced person, asylumseeker*, asylum seeker*] and relevant controlled search terms (MesH, Emtree, and APA Thesaurus terms) were added in each database. This yielded a total of 1423 articles after the removal of duplicates. All were screened for by title, and of these articles, 462 abstracts were screened against the inclusion criteria. Additional 8 articles were identified through other sources (reference lists). Finally, 56 articles were selected for full-text screening. Prisma guidelines were adhered to (Liberati et al., 2009) (see Fig. 1).
Prespecified inclusion criteria were families consisting of two generations (parent-child), children aged 0–18 years. Second, at least one parent had to have status as refugee or asylum seeker and to have experienced trauma. Individuals respond differently to trauma and not everyone develops PTSD symptoms after trauma exposure why PTSD was not chosen as an inclusion criterion. Third, a significant part of children in the sample had to be born in host country or arrived at age < 2 in order to assess effects of parental trauma and not the effects of direct trauma exposure. Finally, studies had to report on variables associated with adverse psychological outcomes in children.
Publications which did not include a measure of parental trauma (defined as either trauma events or posttraumatic stress symptoms) or an explicit statement that parents had been exposed to trauma, and measurement of at least one mental health child outcome (including behavioral problems) were excluded. All original research studies were included, except reviews. Studies in English, Scandinavian, German, French, and Spanish were assessed for eligibility based on abstracts, and in the end, no studies were excluded based on language restrictions.
3. Results
A total of 12 articles met all inclusion criteria (See Table 1): Four longitudinal studies (Back Nielsen et al., 2019; Bager et al., 2020; Sangalang et al., 2017; Vaage et al., 2011), three comparative cross-sectional (Daud et al., 2008, 2005; Field et al., 2013), and five cross-sectional (Dalgaard et al., 2020, 2016; East et al., 2018; van Ee et al., 2016b, 2012). Of these, two articles (Daud et al., 2008, 2005) reported on the (partially) same sample. All studies were conducted in Western countries, three in the U.S. and the rest in Northern Europe. Samples ranged from 21 to 327 children in clinical studies, and two register studies of 19,000 and 35,000 children.
Table 1. Overview of included articles.
Authors | Country of study | Study population | Sample (size, age) | Purpose of study | Study design | Statistical analysis | Assessment of parent trauma and child outcome | Category of risk/protective factors investigated | Main findings |
Back Nielsen et al., 2019. | Denmark | Children born to all refugees who obtained permission to reside in Denmark between 1995 and 2012 | n = 51,793. Age: 0–18 years Descendants born in Denmark: n = 35,329 | To determine whether parental PTSD is associated with childhood psychiatric morbidity among children of refugees | Nationwide register cohort study 1995–2015 | Cox proportional regression model, adjusted for sex, age, disposable household income, and geographical origin | Parent trauma: PTSD diagnosis (ICD-10) in population-based register Child outcome: any psychiatric contact | Parental mental health | Parental diagnosis of PTSD significantly increased the risk of psychiatric morbidity in children of refugees born after arrival (descendants): HR 1.41 (CI 95% 1.22–1.78), lowest for affected father and highest for both parents. |
Bager et al., 2020. | Denmark | Clinical sample of refugee parents treated for torture trauma and war trauma compared to population-level data | n = 19,294 (offspring to traumatized refugees) Age: 0–18 61.2% born in Denmark | To estimate the risk of psychiatric diagnoses in children of severely traumatized refugees | Nationwide register study 1986–2016 | Cox proportional hazards regression, adjusted for sex, calendar time, child age at immigration, parental somatic and psychiatric morbidity | Parent trauma: treatment at trauma center Child outcome: any psychiatric diagnosis during hospital contact | Parental torture exposure | Children of traumatized foreign-born parents had a lower risk of psychiatric diagnosis in childhood compared to non-exposed children of native Danes (HR ranging from 0.49 (95% CI 0.42–0.59) to 0.75 (95% CI 0.65–0.87) depending on country of origin). |
Dalgaard et al., 2016. | Denmark | 30 Middle Eastern refugee families (Iraq, Iran, Lebanon, Palestine, Syria and Afghanistan) referred for treatment of PTSD symptoms | n = 30 Age 4–9 years (mean: 6.78) 14 girls and 16 boys Majority of sample born in host Denmark; 7 children arrived age ≤ 3 | To explore potential risk and protective factors by examining the association between intra-family communication style regarding the parents’ traumatic experiences from the past, children's psychosocial adjustment and attachment security | Cross-sectional (Mixed methods) | t-test correlations and point-biserial correlations Fisher's exact test | Parent trauma: Clinical PTSD symptoms, HTQ (PTSD mean score 2.84) Other measures: HSCL-25, qualitative interview (communication) Child outcome: SDQ (parent version) ATST | Parental mental health | Correlations between parental symptoms (PTSD, anxiety and depression) and the child's psychosocial adjustment and attachment security were n.s. but in the expected direction. |
Parenting | Significant association between intra-family communication style and children's attachment security (Fischer's Exact Test for contingency table*). "Unfiltered Speech” significantly related to insecure attachment. | ||||||||
Dalgaard et al., 2020. | Denmark | 21 mother-child dyads affected by family violence Countries of origin: Syria, Iran, Lebanon, Iraq, Eritrea, Yemen, and Afghanistan | n = 21 Mean age: 10.29 Born in Denmark | To explore mother/child dyadic functioning, and symptom levels in mothers and children's psychosocial adjustment | Comparative cross-sectional | Correlation table, adjusted for child age | Parent trauma: Clinical PTSD diagnosis (>1 parent), HTQ (90.5% above clinical cut-off) Other measures: HSCL-25, MIM Child outcome: SDQ (parent report age <8, self-report age ≥8), KIDSCREEN-10S index (self-report) | Parental mental health | Significant association between maternal symptoms and child psychosocial adjustment (SDQ difficulties): Anxiety and depression (HSCL-25): r = 0.62⁎⁎, PTSD (HTQ): =0.57* |
Parenting | Significant association between dyadic functioning and child HRQoL (KIDSCREEN-10): domains Challenge: r = 0.51*, Nurture: r = 0.58*. | ||||||||
Daud et al., 2005. | Sweden | Test group: 15 families where the parents had been tortured in Iraq & Lebanon. Comparison group: 15 families from similar ethnic background | n = 76 Age 6–17 years Test group: n = 45 29 boys, mean age: 12 years, 16 girls: 11.3 years) Comparison group: n = 31 All or most children born in Sweden | To test whether children of traumatized parents display more symptoms of psychopathological disorder than children of non-traumatized parents and to test associations between children's and parents’ symptoms in families where the parents were subjected to torture | Comparative cross-sectional | t-test Pearson Chi-Square | Parent trauma: Clinical interview and H/UTQ (29 out of 30 parents in test group fulfilled DSM-IV criteria for PTSD) Child outcome: DICA-R | Parental mental health | Children's symptoms associated to their parents’ symptoms (data not presented). |
Parental torture exposure | Children of traumatized parents had more symptoms of anxiety, depression, posttraumatic stress, attention deficits and behavioral disorders compared to comparison group of children of non-traumatized parents (⁎⁎⁎). | ||||||||
Daud et al., 2008. | Sweden | Same sample as above | n = 80 Age 7–16 years Test group: n = 40 (mean age: 12.1) Comparison group: n = 40, (mean age: 12.5) All children born in Sweden (partially same sample as above) | To explore resilience among children whose parents had been traumatized and were suffering from Post-Traumatic Stress Disorder (PTSD) | Comparative cross-sectional | Student's t-test Not adjusted One-way ANOVA F-test Not adjusted Pearson correlation coefficients | Parent trauma: same as above Child outcome: DICA-R, PTSS checklist (self-rating), SDQ (teacher rating) Other measures: WISC-III (IQ), ITIA (self-esteem) | Parental torture exposure | Children of traumatized parents had significantly lower IQ scores compared to children of non-traumatized parents. |
Individual child characteristics | Association between self-esteem and PTSD-related symptoms in test group: psychological wellbeing (*), total score (*), and relation to family (p < 0.06). | ||||||||
Social factors | Association between children's PTSD symptoms and peer relations (SDQ peer problems⁎⁎⁎), and family relations (ITIA relation to family: mean score 16.8 (SD = 7.1) for children with symptoms, mean 20 (SD = 7.4) for children without symptoms). | ||||||||
East et al., 2018. | U.S. | 198 Somali mothers and their children | n = 198 Age 7–14 years (mean age: 10.4) 56% male 76% of children born in U.S. | To identify how Somali refugee mothers’ past trauma and current mental health impact their children's psychosocial adjustment | Cross-sectional | Chi square | Parent trauma: HTQ (average 42 traumatic events and 1 torture event) Other measures: HSCL Child outcome: Children's Depression Inventory-2 (CDI-2) (self-rating), Perceived Racism Scale‐Children (PRS‐C) (self-report), Peer Victimization Scale (self-report), HUTQ-C (self-report) | Parental mental health | Mothers’ depressive symptoms significantly associated to child functioning (depressive symptoms: r = 0.40*, perceived racism: r = 0.65⁎⁎, and bullying victimization r = 0.76⁎⁎⁎). |
Parental torture exposure | Association between past trauma events and children's functioning n.s. Maternal PTSD and depressive symptoms mediated the effect of torture exposure on children's functioning (perceived racism and bullying victimization). | ||||||||
Social factors | Maternal lower education related to bullying victimization (r = −0.18*). | ||||||||
Field et al., 2013. | U.S. | Cambodian-American refugees: 15 mental health treatment-seeking mothers and their children. 17 non-treatment-seeking mother–child pairs. | n = 32 Clinical sample: n = 15, mean age: 16.07 Non-clinical sample: n = 17, mean age 16.24 10 boys, 22 girls All children born in U.S. | The impact of parental styles in intergenerational transmission of trauma among mothers who survived the Khmer Rouge regime in Cambodia, in power from 1975 to 1979, and their teenaged children | Comparative cross-sectional | Correlation analysis | Parent trauma: HTQ (clinical group: mean = 11.67 traumatic events, non-clinical group: mean = 10.53 traumatic events), PTSD checklist Other measures: Social support Child outcome: HSCL-25 Other measures: Parental Bonding Instrument (PBI), Relationship with Parents Scale (RPS) | Parental mental health | Significant association between maternal PTSD and the child's anxiety (pr = 0.70⁎⁎⁎) and depression (pr = 0.45⁎⁎). Effect partially mediated by role-reversing parenting. |
Parenting | Associations between parenting styles and child outcomes: Role-reversing parenting and anxiety (pr = 0.55⁎⁎) and depression (pr = 0.47⁎⁎). Rejecting parenting and anxiety (pr = 0.40*). | ||||||||
Sangalang et al., 2017. | U.S. | Southeast Asian (Cambodian and Vietnamese) refugee mothers and their children | n = 327 Mean age: 12 years 51% girls 62% of sample born in U.S. (of foreign-born, 53.6% <5 years at migration) | To: (1) examine the effects of maternal traumatic distress on family functioning and child mental health, and (2) explore differences in these associations by ethnicity and child nativity. | Longitudinal (2 years) | Chi square, adjusted for child age and family structure | Parent trauma: HTQ (mean PTSD symptoms 1.56) Other measures: “Family functioning” measure Child outcome: A measure of Depressive symptoms, Antisocial behavior, Delinquent behavior, and School problems (self-report) | Parental mental health | U.S. born: Association between maternal PTSD symptoms and child outcomes n.s. Weaker family functioning was significantly associated with more depressive symptoms (b = 0.16*), antisocial behavior (b = 0.24⁎⁎), and delinquent behavior (b = 0.27⁎⁎) in children. |
Parenting | |||||||||
Vaage et al., 2011. | Norway | Vietnamese refugee families | n = 127 Age 4–23 years (mean age: 12.8 years, 94 children aged 4–18) 49 girls and 57 boys All children born in Norway | 1. To study the association between the psychological distress of Vietnamese refugee parents and their children after 23 years resettlement. 2. To analyze paternal predictors for their children's mental health. | Longitudinal prospective cohort study (1982–2006) | Simple and multiple linear regression, adjusted for siblings | Parent trauma: Symptom Check List-90-R (SCL-90-R) (28.3% full or “partial” PTSD during study period) Child outcome (age 4–18): SDQ (self report) | Parental mental health | Association between parental psychological distress and child outcome n.s. (only for older children >18). |
Social factors (network) | A significant positive predictor for fewer problems (SDQ) was the father's participation in a Norwegian network (>10 friends): estimate −6.19 (SD = −8.63, −3.76⁎⁎). | ||||||||
van Ee et al., 2012. | Netherlands | Asylum-seeker and refugee mothers and their children from Eastern Europe, Russia, Asia, Middle East, Africa | n = 49 Age 18–46 months (mean: 26.6) 28 boys, 21 girls All children born in the Netherlands | To examine the association between maternal posttraumatic stress symptoms, parent–child interaction and infants’ psychosocial functioning and development | Cross-sectional | Preliminary analyses: Chi-square test, Fisher's Exact test, Kendall's τ, one-way analysis of variance, or Mann–Whitney U test | Parent trauma: HTQ (mean PTSD 2.56) Other measures: HSCL-25, “Current stressors”, Parent-child interaction: Emotional Availability Scales Child outcome: Child Behavior Check List (CBCL) (parent report), Bayley Scales of Infant Development | Parental mental health | Significant association between maternal posttraumatic stress symptoms and infant psychosocial functioning (CBLC): internalizing behavior, r = 0.40⁎⁎, total problems, r = 0.40⁎⁎. Maternal posttraumatic stress symptoms associated with lower scores of parent-child interactions: parent sensitivity, r = −.49⁎⁎, structuring, r = −.43⁎⁎, and nonhostility, r = 0.35*, infant responsiveness: r = −.45⁎⁎; and infant involvement: r = −.37*. |
Parenting (observed emotional availability in parent-child interaction) | Significant association between nonhostility and internalizing behavior, r = −.30*, and total problems, r = −.30*. | ||||||||
Van Ee et al., 2016b. | Netherlands | 68 asylum seekers and refugee parents in the Netherlands with traumatic experiences and their children from Eastern Europe, Asia, Middle East, Africa, and South America | n = 50 Age: 18–42 months (mean: 29.7 months) 31 boys and 19 girls All children born in the Netherlands | To examine the relation between parental PTSD and child attachment, and the unique contribution of disconnected and extremely insensitive parenting behavior to these associations | Cross-sectional | Multilevel structural equation modeling | Parent trauma: HTQ (59.4% had clinical level of PTSD symptoms, mean 2.71) Other measures: Parenting behavior: Disconnected and extremely Insensitive measure Parenting (DIP) Child outcome: SSP (The Strange Situation Procedure) | Parental mental health | Parental symptoms of PTSD associated with child attachment (attachment security: β=1.92, SE=0.89*), attachment organization: β=1.49, SE=0.91*). |
Parenting (observed adverse behavior) | Adverse parenting behavior partially linked to attachment (disconnected parenting and disorganized attachment: β=0.57, SE.26*). | ||||||||
Social factors |
Since the articles as a whole were heterogeneous in terms of study design, samples/populations and outcomes, a meta-analysis was not performed (Harris et al., 2014) and instead, the results are presented in a qualitative analysis. The categorization of findings is inspired by Bronfenbrenner's bioecological model of child development which places the child in the center of environmental influences ranging from micro (parents) to macro (society) level (Bronfenbrenner and Morris, 2006). This model also takes into account the personal characteristics and resources of a person. Inspired by this theoretical framework, this review sought to identify categories of risk and protective factors on different levels of child development (Bronfenbrenner and Morris, 2006). Based on findings from the included studies, five different categories of risk/protective factors were identified: factors related to parental mental health symptoms, parenting, parental torture exposure, individual child characteristics, and social factors. In the following, the findings are presented with respect to each identified factor. Each article is briefly presented with respect to study aim, sample characteristics and main relevant findings the first time it is mentioned.
3.1. Parental mental health symptoms
The majority of included studies investigated the associations between parental mental health and child mental health, nine articles in terms of parental symptoms of PTSD, depression, or anxiety and one study regarding the effect of parental PTSD diagnosis (See Table 1). Seven out of 10 articles identified associations between parental mental health and child mental health outcomes (Back Nielsen et al., 2019; Dalgaard et al., 2020; Daud et al., 2005; East et al., 2018; Field et al., 2013; van Ee et al., 2016b, 2012) as described in the following.
Based on register data of more than 35,000 children born in Denmark to refugees over a 20 year-period, Back-Nielsen et al. (Back Nielsen et al., 2019) compared the psychiatric morbidity of children of refugee parents with PTSD to the psychiatric morbidity of children of refugees without PTSD and found that a parental diagnosis of PTSD significantly increased risk of psychiatric morbidity in children.
Likewise, two comparative cross-sectional studies identified associations between parental symptoms of PTSD and child mental health outcomes. In a test group of children of tortured refugee parents, Daud et al. (2005) reported that the children's symptoms were associated to their parents’ symptoms, however, these results were not presented in the article. In a sample of Cambodian-American refugee mothers and their teenage children, Field et al. (2013) found a significant association between maternal PTSD symptoms and the child's anxiety and depression, while there was no significant difference in parental trauma exposure between a clinical, treatment-seeking group and a non-clinical group; both groups had lived through the Khmer rouge regime and had high trauma exposure.
In a small sample of mother-child dyads affected by family violence, Dalgaard et al. (2020) found that maternal symptoms of anxiety, depression and PTSD were related to psychosocial problems in children. The sample was a convenience sample recruited when referred for family treatment on the basis of past or ongoing trauma-related family violence (physical child abuse or intimate partner violence) at a refugee rehabilitation center. One child (“target child”) from each family was chosen by a clinician for assessment. In a larger sample of Somali women and their children, East et al. (2018) found that mothers’ depressive symptoms were significantly associated to the children's depressive symptoms, perceived racism, and bullying.
The effect of parental symptoms on younger children was investigated in two studies: in a diverse sample of asylum-seeker and refugee mothers and their toddlers, Van Ee et al. (2012) found a significant association between maternal PTSD symptoms and child psychosocial problems (parent-reported). In a different study, Van Ee et al. found a negative association between parental PTSD and child attachment security as observed in a clinical experiment (the Strange Situation Procedure) (van Ee et al., 2016b).
Finally, three articles did not identify significant associations: In a small sample of families referred for PTSD treatment, correlations between parental symptoms of PTSD, anxiety and depression and the child's psychosocial adjustment and attachment security were non-significant (Dalgaard et al., 2016). In a two-year longitudinal study of Cambodian and Vietnamese refugee mothers and their children by Sangalang et al. (2017), maternal PTSD symptoms were not associated with child mental health outcomes two years later. In a longitudinal study by Vaage et al. (2011), there was no association between paternal PTSD at arrival in Norway and mental health in children <18 at follow-up 23 years later.
3.2. Parenting
The category of “parenting” includes all concepts of parenting styles, communication styles, and intra-family interactions. These concepts were investigated in six studies employing different measures.
Three of these studies assessed aspects of parenting by parent or child reports. The findings of Sangalang et al. (2017) indicated that weaker family functioning, as reported by the mother, was associated with more mental health problems in children. Dalgaard et al. (2016) found that intra-family communication styles regarding past traumas, assessed by parental interviews, was associated with child attachment security. Specifically, “unfiltered” communication where the parent reported not disclosing past trauma, but openly described traumas in the presence of the child, was associated with insecure attachment. Using teenage children's retrospective assessment of their relationship with their mothers, Field et al. (2013) found that role-reversing and rejecting parenting, but not overprotecting parenting, were associated to current child symptoms of anxiety and depression. Here, role-reversal was defined by parents’ helplessness, imposing guilt, demands for attention, and seeking direction from the child.
Three studies evaluated family dyadic interactions based on observations. Dalgaard et al. (2020) measured dyadic functioning based on observations of mother and child behavior in a play-based test setting and found that some domains of positive dyadic functioning (challenging and nurturing the child) were significantly associated with greater health related quality of life in the child. Additionally, the authors observed that patterns of role-reversal in some cases were affected by the fact that children spoke the host country language fluently and thus ended up reading instructions and structuring the session (Dalgaard et al., 2020). Van Ee et al. (2012) studied emotional availability in play-based interactions between mothers and young children. Mothers’ non-hostility was correlated to less child psychosocial problems and less child internalizing behavior. Child behavior was assessed by parent report, causing a possible bias (see Discussion). In another study, Van Ee et al. (2016b) studied parenting behavior during an unstructured play session and found that ‘disconnected’ parenting was linked to decreased attachment organization in young children. Disconnected parenting was characterized by e.g., unpredictable changes in the parent's otherwise normal behavior, or the parent's disorganized or frightening behavior, and was hypothesized to stem from disconnectedness from the environment (traumatic dissociation).
3.3. Parental torture exposure
Three studies investigated the effect of parental torture exposure as a risk factor. Bager et al. (2020) found a lower risk of psychiatric disorder in children of foreign-born parents who had been referred to treatment for torture or war trauma at specialized centers compared to children of non-traumatized native Danes (See Discussion).
Daud et al. (2005) found that children of tortured refugee parents, recruited from trauma treatment centers, had more symptoms of anxiety, depression, posttraumatic stress, attention deficits, and behavioral disorders compared to a control group of similar ethnicities. They also investigated personality features, hypothesizing that torture would lead to a post traumatic personality, and found that the parents exposed to torture differed from parents in the comparison group with respect to detachment, muscular tension, and guilt. East et al. (2018) investigated the effects of past trauma and torture events separately. The direct associations between torture events and child outcomes were not significant, but maternal depressive symptoms mediated the effect of torture events on child functioning (perceived racism and bullying).
3.4. Individual child characteristics
In one study, the effects of children's individual characteristics were investigated. Daud et al. (2008) compared psychological symptoms, IQ and self-esteem in children whose parents had been tortured. The results did not support their hypothesis that IQ was a factor involved in understanding resilience (protective factor): there was no significant difference in IQ between the children with symptoms PTSD-related symptoms and children without symptoms. The children without symptoms had higher self-esteem (as measured by a self-report questionnaire designed specifically for assessing self-esteem) than the children with symptoms, suggesting self-esteem as a protective factor.
3.5. Social factors
Four studies included analyses on variables we have chosen to call “social” factors, representing factors related to the social environment surrounding the children, sociodemographic, and family level factors. These factors are not identical but are presented here together, as they were not the main focus of any of the included studies.
Daud et al. (2008) highlighted the variables peer relations and family relations as possible environmental protective factors. Children without PTSD-related symptoms tended to have better relation to family and fewer peer problems. According to the authors, the results indicate that adequate family relations are a plausible protective factor, even if the parents are not well themselves, and indicate that good peer relations are a possible environmental protective factor. The findings of Vaage et al. (2011) hinted to the importance of parents’ social networks: fathers’ number of native friends predicted better child mental health.
East et al. (2018) found that mother's lower education was related to more bullying victimization and perceived racism reported by the child. Van Ee et al. (2016b) tested whether the following predictors at the family level could explain differences in child attachment: family composition (single parents versus traditional family composition), child sex, residence permit (asylum seekers versus refugees), and number of parents with a clinical level of PTSD symptoms within the family. Neither of these predictors were significant.
4. Discussion
This review aimed to identify risk and protective factors related to adverse mental health outcomes in children of trauma-affected refugees including both interpersonal and contextual factors. The main identified categories of risk/protective factors were parental mental health symptoms and parenting, the implications of which will be discussed in detail below. Other identified categories of risk/protective factors were parental torture exposure, individual characteristics, and social factors e.g., peer relations, social network, and education. Findings regarding these categories were inconclusive and methodologically differing and will only be discussed in a general manner concerning the generalizability of findings. Generally, studies focused on identifying risk factors, while only four studies explicitly sought to identify protective factors (Dalgaard et al., 2020, 2016; Daud et al., 2008; van Ee et al., 2012). In studies which explored the negative effects of parental mental health symptoms, protective factors were indirectly explored in the sense that fewer parental symptoms were identified as a protective factor.
Compared to a previous review by Flanagan et al. (2020) which aimed to identify potential mechanisms of intergenerational trauma transmission in refugee families, the current study set out to identify a broader scope of risk and protective factors and included two more recent years. Seven of the 12 studies included in this review were included in the former study which comprised a total of eight studies. Notably, the present review included more recent populations of refugees and their children, and two large samples of 35,000 (Back Nielsen et al., 2019) and 19,000 children (Bager et al., 2020).
Results from the included studies emphasized the effect on children of symptoms of PTSD, anxiety, and/or depression among trauma-affected parents. The prevalence of PTSD in the included samples was generally high, and children's symptom levels were largely associated with parents’ symptom levels. This is in line with research in the general population which has linked parental PTSD to an array of adverse child outcomes (Leen-Feldner et al., 2013). Offspring sequelae in general populations include psychological outcomes (internalizing problems, behavioral problems) and biological outcomes (altered HPA axis functioning) (Leen-Feldner et al., 2013). While this review focused on child mental health outcomes, parental trauma in refugee populations affect other areas of child functioning. A recent Swedish register study found that children's school performance was negatively affected by parental PTSD in refugee families (Berg et al., 2019) and a recent US study suggested increased risk of criminal behavior. Trauma, PTSD, and depression are also linked to increased risk of family violence (Timshel et al., 2017).
Results of the included studies concerning torture exposure were inconclusive, partially due to sample sizes and recruitment. One register study by Bager et al. (2020) found a negative association between parental torture exposure and child psychopathology, in contrast to the existing body of research. Notably, there was a lower risk of psychiatric disorder diagnoses among all children of foreign born-parents, regardless of whether the parents had been exposed to trauma or not, compared to children of native parents; a pattern indicating general underutilization of mental health services by minority populations (Bager et al., 2020). An overall lower use of mental health services in spite of higher susceptibility to mental health problems is a well-known phenomenon among immigrants compared to natives (Sarria-Santamera et al., 2016).
Furthermore, the findings of this review indicate that parenting and family functioning constitute important risk/protective factors for child mental health. Identified risk factors linked to parenting behavior included parent-child role reversal (Dalgaard et al., 2020; Field et al., 2013), disconnected (van Ee et al., 2016b) and hostile (van Ee et al., 2012) parenting, and unfiltered trauma communication (Dalgaard et al., 2016). Protective factors were positive dyadic functioning (Dalgaard et al., 2020) and emotional availability (van Ee et al., 2012). In line with these findings, a recent cohort study on prolonged grief among refugees found that harsh parenting was associated with children's emotional problems, hyperactivity, and behavioral problems, and on the other hand, warm parenting was associated with less hyperactivity (Bryant et al., 2020).
In one included study, patterns of role-reversal were linked to intergenerational language barriers, because the child, fluent in host country language, was the one to translate messages and initiate assignments in a test setting; a pattern likely to occur often in day-to-day life (Dalgaard et al., 2020). An inherent part of family relations, language can influence trauma transmission in different ways, and language as well as cultural barriers between parents and children are a potential challenge to family functioning. Among Southeast Asian refugees, the rapid acquisition of language in children, in combination with intergenerational differences in culture, has been found to turn traditional family hierarchies upside down and create family conflict (Ying and Han, 2007). It is likely that such alterations in family dynamics can exacerbate trauma symptoms. Generally, the refugee parenting experience is characterized by disruptions which can affect established roles (gender, parent-child roles), family structure and hierarchies (Fazel and Betancourt, 2018; Williams, 2010).
As pointed out by Daud et al. (2008), parenting is not the sole aspect to consider, and evaluations of parenting in trauma-affected samples should not be reduced to judgements of whether the parent is a “good enough” parent. Being a parent who has been through life-threatening events is in itself threatening to the notion of family as a secure base (Daud et al., 2008), and dealing with one's own traumatic experiences and handling parenting responsibilities at the same time should be recognized as an extraordinary task (Fazel and Betancourt, 2018). In addition to past trauma, worries over family members in insecure conditions are a continuous stressor among Somali refugees (Betancourt et al., 2015). Focusing research solely on aspects of parenting comes with the potential risk of not identifying other relevant arenas, e.g., socioeconomical factors.
As highlighted by attachment theory (Ainsworth, 1978), parenting qualities are essential to healthy child development and negative – or inconsistent – parenting a potential stressor. Another weighty reason why a clinical focus on parenting makes good sense, as argued by Goodman et al. (Goodman et al., 2020), is that parenting is not a static, rather, research on maternal depression and parenting suggests it is a modifiable variable. Parenting abilities in refugee populations are influenced by a multitude of extraneous factors such as socioeconomic and legal status which should be taken into account in a clinical setting. This highlights the importance of studying both parenting and external factors impeding or promoting good parenting despite trauma.
A recent review aimed at interventions for refugee children and unaccompanied minors (Frounfelker et al., 2020) highlighted that while there is ample research concerning the prevalence of mental disorders among refugees, knowledge on evidence-based interventions for refugee youth is scarce. Interventions can generally be divided into the unimodal and multimodal kind (Fazel, 2018). While unimodal interventions, aimed at treating a specific psychological disorder, have been researched to some extent, there have been very few multimodal psychosocial interventions aimed at family, school, or the wider community (Fazel, 2018). School-based interventions can consist of broad mental health promotion offered to all students and to those identified as high-risk students. Two recent studies have explored relevant family interventions. A smaller parenting intervention for Burmese refugees in the U.S. was thoroughly adapted to fit the culture and current parenting practices of the sample (Ballard et al., 2018). Their recommendations for future parenting interventions among trauma-exposed communities included the integration of traumatic stress psychoeducation/awareness and emotional regulation (Ballard et al., 2018). A community-based, home-visiting intervention for Somali refugee families aimed at improving communication, navigating the US school system, and learning positive parenting practices (Betancourt et al., 2020). They adapted an evidence-based intervention to fit refugee communities and findings suggested that it improved child functioning and improved family relationships (Betancourt et al., 2020).
Many of the studies included are cross-sectional and some of the factors identified are therefore probably not causally related as this would require studies with a longitudinal design. Since a risk factor can be defined as a correlate which precedes the outcome/symptoms (Kraemer et al., 2001), the identified correlates in cross-sectional studies are not necessarily true risk factors. Within several of the studies, there is the additional possibility of reciprocal causality between variables. Depressive symptoms in mothers may affect children's depressive symptoms, but in turn, children's symptoms may also affect the mothers or increase existing symptoms (East et al., 2018). Additionally, three included studies used parent-reported child psychological outcomes (Dalgaard et al., 2020, 2016; van Ee et al., 2012). Self-report or report by a third party (e.g., teacher) is methodologically sounder because parents with PTSD symptoms tend to have more negative perceptions of their children (Leen-Feldner et al., 2013; van Ee et al., 2016a). In one study (Dalgaard et al., 2020), one “target” child from each family was chosen by a clinician for assessment based on which child appeared most affected by family problems. This is another possible cause of bias since the selection was not random, and the “target” children possibly had more negative symptoms than their siblings. Most studies used clinical interviews to assess parental PTSD symptoms which is the “gold standard” (Leen-Feldner et al., 2013). The results regarding individual and social factors were inadequate for generalizations, signifying the need for broader assessments of risk/protective factors.
4.1. Limitations to this study
Refugees are not a homogenous population; on the contrary, depending on cultural and historical contexts, risk and protective factors may vary greatly among different groups of refugees. Findings from one population of trauma-affected refugees cannot automatically be generalized to all groups as their trauma experiences have specific social and political contexts (Sangalang et al., 2017). Likewise, intra-family communication, parenting, and language vary across cultures, all affecting the effects of parental trauma on children. In addition to the heterogeneity of refugee populations, as a group they are difficult to reach for research purposes and samples often small and non-random (Henkelmann et al., 2020). Due to the heterogeneity of the studies, a meta-analysis could not be performed. Though the possibility of publication bias favoring significant results and larger samples is always present, many of the included articles reported non-significant results.
The included studies all stem from Western host countries. Though internally displaced and refugees situated in refugee camps make up the majority of displaced personsworldwide (United Nations High Commissioner for Refugees, 2020), research unproportionally focuses on refugees resettled in Western countries. The challenges faced by refugee children vary greatly depending on whether they live in a high-income or low-income country (Fazel et al., 2012; Reed et al., 2012), and the same is probably the case for children of refugees born in these countries.
The strength of this review is that it provides a thorough overview of the most recent research on a specific group of children; children born in host countries to trauma-affected refugees, and thus encompasses the specific risk and protective factors related to this experience. It includes several studies of rigorous design, large samples/cohorts, child outcomes assessed by third parties. Limitations include studies with smaller samples, parent-reported child outcomes, non-clinically assessed PTSD, and a lack of research exploring epigenetic/biological alterations.
4.2. Summary and recommendations for interventions
As highlighted in this review, recent research has provided convincing evidence of the increased risk of psychological disorders in children of parents with PTSD and other mental health symptoms in refugee populations. It is thus not a question of whether children of trauma-affected parents should be considered at-risk, but rather how to promote resilience and improve outcomes through culturally relevant interventions. Generally, studies focus mainly on risk factors for negative outcomes, while there is a dearth of knowledge on protective factors as seen in this review. Protective factors and the promotion of resilience should be further explored.
Longitudinal research is needed to establish causal pathways in trauma transmission and clarify risk and protective factors. The mental health of children cannot be isolated to one or several individual factors, but are linked to basic conditions of e.g., political status, economic status, access to education which constitute general determinants of health (Fazel and Betancourt, 2018).
The findings of this review suggest that relevant interventions could be aimed at 1) improving parental mental health, i.e., individual and family therapy, and 2) reinforcing positive parenting practices and family functioning. A focus on parents is especially warranted as improvement of their mental health and stressors in the family could potentially improve outcomes for the children (Fazel and Betancourt, 2018). However, more knowledge on effective interventions is warranted. Future research should also explore the significance of social networks, local communities, and other potential psychosocial protective factors.