Abstract
Can purely psychological trauma lead to a complete blockage of autobiographical memories? This long-standing question about the existence of repressed memories has been at the heart of one of the most heated debates in modern psychology. These so-called memory wars originated in the 1990s, and many scholars have assumed that they are over. We demonstrate that this assumption is incorrect and that the controversial issue of repressed memories is alive and well and may even be on the rise. We review converging research and data from legal cases indicating that the topic of repressed memories remains active in clinical, legal, and academic settings. We show that the belief in repressed memories occurs on a nontrivial scale (58%) and appears to have increased among clinical psychologists since the 1990s. We also demonstrate that the scientifically controversial concept of dissociative amnesia, which we argue is a substitute term for memory repression, has gained in popularity. Finally, we review work on the adverse side effects of certain psychotherapeutic techniques, some of which may be linked to the recovery of repressed memories. The memory wars have not vanished. They have continued to endure and contribute to potentially damaging consequences in clinical, legal, and academic contexts.
The past is never dead. It’s not even past.
Faulkner (1950/2011, p. 73)
More than 20 years ago, Crews (1995) coined the term “memory wars” to refer to a contentious debate regarding the existence of repressed memories, which refers to memories that become inaccessible for conscious inspection because of an active process known as repression. This debate raged throughout the 1990s and was widely assumed to have subsided in the new millennium. A number of prominent authors who were skeptical of repressed memories (e.g., Barden, 2016; McHugh, 2003; Paris, 2012) declared the memory wars to be effectively over, essentially arguing that most researchers and clinicians now understand that believing in such memories without reservation is at best questionable scientifically. The argument among these authors is essentially that the recovered-memory skeptics won. Others argue that the memory wars have been resolved in the opposite direction, stating that there is now better evidence for a trauma-dissociation model and less room for a skeptical stance toward repressed (dissociated; see below) memories (Dalenberg et al., 2012). Some proponents of the idea of dissociative amnesia (i.e., the inability to remember autobiographic experiences usually as a result of trauma) have even likened skeptics to climate-science deniers (Brand et al., 2018, in response to Merckelbach & Patihis, 2018). Their argument appears to be that they have won the memory wars, and further proof of this is the continued inclusion of dissociative amnesia in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–5; American Psychiatric Association, 2013; see also Spiegel et al., 2011).
In this article, we present evidence that the debate concerning repressed memories is by no means dead. To the contrary, we contend that it rages on today and that the term dissociative amnesia is being used as a substitute term for repressed memory. To buttress this point, we present converging lines of evidence from several sources suggesting that the concept of repressed memories has not vanished and that it has merely reappeared in numerous guises (e.g., in the context of dissociative amnesia). Admittedly, some researchers have argued that the memory wars have persisted (e.g., Patihis, Ho, Tingen, Lilienfeld, & Loftus, 2014), but no review has systematically and critically evaluated this proposition. In this article, we amass evidence from multiple sources showing that beliefs associated with repressed memories and related topics such as dissociative amnesia, far from being extinguished, as claimed by some scholars, remain very much alive today. Furthermore, we demonstrate that these beliefs carry significant risks in clinical and legal settings.
Repressed Memories and the Memory Wars
As Ellenberger (1970) explained in his classic monograph, the concept of repressed memories traces its roots to the psychoanalytic theory and practice of Sigmund Freud, who in turn was influenced by physician-hypnotists, such as Jean-Martin Charcot, in the final decades of the 19th century. At the heart of this concept is the idea that traumatic experiences are often so overwhelming that people use defense mechanisms to cope with them. One of these mechanisms involves the automatic and unconscious repression of the traumatic memory with the consequence that people no longer recollect or retain awareness of the experience that triggered it (e.g., Loftus, 1993; McNally, 2005; Piper, Lillevik, & Kritzer, 2008). Nevertheless, according to this view, the repressed trauma ostensibly exacts a serious mental and physical toll (Hornstein, 1992), manifesting itself psychologically and somatically in a wide array of symptoms (e.g., fainting, amnesia, mutism). This influential body-keeps-the-score hypothesis implies that trauma can be “entirely organized on an implicit or perceptual level, without an accompanying narrative about what happened” (van der Kolk & Fisler, 1995, p. 512). The goal of therapy is thus to make the implicit—the repressed—explicit (Yapko, 1994a), following Freud’s famous tenet that psychoanalysis aims to make the unconscious conscious. Thus, the notion of repressed memories encompasses three ideas: People repress traumatic experiences, the repressed content has psychopathological potential, and recovering traumatic content is necessary for engendering symptom relief.
In the 1990s, as we demonstrate in a review of data of surveyed clinicians, the belief in repressed memories was endemic in therapeutic circles. Even when patients did not recollect the trauma, such as sexual abuse, some therapists suggested that their unconscious may harbor repressed memories. When clients presented with symptoms of, for example, anxiety, mood, personality, or eating disorders, many clinicians seemed to take these symptoms as signs of long-repressed memories of abuse. Furthermore, in the 1990s, dream interpretation, hypnosis, guided imagery, repeated cuing of memories, and diary methods, among other recovered-memory techniques, were used by many practitioners to ostensibly uncover repressed memories and bring them to the surface of consciousness. As a result of these treatments, patients started to recover purported memories of abuse, typically sexual abuse, and some filed criminal or civil suits against their alleged perpetrator (Loftus, 1994; Loftus & Ketcham, 1994).
During these therapeutic interventions, suggestive techniques were commonly used to recover the alleged repressed memory. At that time, laboratory research began to show the deleterious effects of suggestion on autobiographical recollections of childhood episodes. In one of the first such studies, Loftus and Pickrell (1995) asked students to report on four events that happened in their childhood. One event was fabricated and involved being lost in a shopping mall at about 5 years old. Students were told that their parents provided these narratives to the experimenters, while in fact, parents had confirmed that the event did not happen. After three suggestive interviews, 25% (n = 6) of the participants claimed that the false event in fact had occurred. This and other studies during the 1990s indicated that false autobiographical memories1 can be implanted with suggestive interviewing techniques (e.g., Hyman, Husband, & Billings, 1995; for earlier relevant work, see Laurence & Perry, 1983; for a review of false memories before 1980, see Patihis & Younes Burton, 2015).
Many memory scholars have argued on the basis of this research that repressed memories recovered in therapy may not be based on true events but could be false memories (Lindsay & Read, 1995; Loftus & Davis, 2006). An additional scenario offered by researchers is that some people may reinterpret childhood events as a result of therapy and come to experience this reinterpretation as a recovered memory of abuse (McNally, 2012). For example, Schooler (2001) argued that individuals may initially not experience their abuse as traumatic but later come to reevaluate it in this fashion. This change in meta-awareness may be experienced as a recovery of a memory when it instead comprises a new interpretation of a memory that was accessible all along. Schooler offered several case descriptions suggestive of this intriguing process, but strictly speaking it does not involve the reemergence of repressed memories into consciousness. Nevertheless, the reinterpretation account may be a plausible explanation of certain recovered memories of events that were genuinely experienced.
Still, not all cases that were described by Schooler (2001) can be interpreted in terms of reevaluation. Wagenaar and Crombag (2005), for example, noted the inherent problems that such descriptions have to demonstrate the existence of recovered memories. They criticized Schooler’s case descriptions on the grounds that many assumptions needed to be met to confirm the existence of recovered memories in these cases. For example, Wagenaar and Crombag observed that alleged victims sometimes received therapy that may have influenced their memories. In addition, Wagenaar and Crombag noted that claiming to have forgotten sexual abuse is not the same as having forgotten the abuse.
Apart from suggestive techniques that might lead to the creation of memory aberrations, some memory researchers noted that the concept of repressed memories is difficult to reconcile with studies on the effects of trauma on memory. Specifically, a large body of data suggests that the central aspects of trauma tend to be relatively well remembered (McNally, 2005). Several authors concluded that complete memory loss for traumatic events is rare among trauma victims, such as Holocaust survivors (Wagenaar & Groeneweg, 1990), survivors of Japanese/Indonesian concentration camps (Merckelbach, Dekkers, Wessel, & Roefs, 2003), and victims of sexual abuse (Goodman et al., 2003). Furthermore, the idea of repressed memories runs counter to well-established principles of human memory. For example, purported repressed memories are often about repeated experiences of abuse, but repeated events are generally well recollected. In addition, people with posttraumatic stress disorder (PTSD) frequently experience flashbacks and intrusive memories of the trauma and hence do not typically report repressed memories, at least of their triggering traumatic event. In addition, the idea of apparent recovered memories suggests that experiences can be forgotten and “recovered” following retrieval cues. This common memory phenomenon does not require the idea of repressed memories (for an overview, see Roediger & Bergman, 1998).
The recovery of mundane childhood memories is a perfectly normal phenomenon, although people may find it difficult to estimate how long they have not thought about a childhood experience (Parks, 1999). The recovery of a purportedly long-forgotten trauma is less plausible in light of everything that we know about traumatic memories (see above), and in such cases the question is whether there is independent evidence to corroborate the memory. Thus, a central issue concerning recovered memories is whether they can be independently corroborated. Studies examining corroborative evidence of recovered memories are often limited because they rely exclusively on victims’ characterizations of corroboration (e.g., Chu, Frey, Ganzel, & Matthews, 1999; Herman & Harvey, 1997). Research in which at least partial independent corroboration has been sought demonstrated that continuous memories of child sexual abuse recalled outside of therapy were more often corroborated than discontinued memories of abuse recovered in therapy (Geraerts et al., 2007; see also McNally, Perlman, Ristuccia, & Clancy, 2006). Another key point concerning recovered memories is that people may not think about the abuse for many years or may forget their previous recollections of their traumatic experience. Such people might then spontaneously recover memories of abuse when reminded about the abuse outside of therapy. However, such a phenomenon, psychologically important as it is, is a far cry from repressing a richly detailed memory in its entirety and later recalling it in therapy or everyday life (McNally & Geraerts, 2009).
One way to examine how clinicians think about the reality of repressed memories is to survey them about their beliefs on the topic and on their technical knowledge of how memory works. In this respect, a summary of practitioner-survey studies since the 1990s is informative.
Memory Beliefs About Repressed Memories: From Then to Now
Beliefs among clinical psychologists
Scientific interest in what therapists and other mental-health professionals know about the functioning of memory originated because incorrect beliefs about memory could catalyze suggestive clinical practices and flawed treatment plans (Gore-Felton et al., 2000). Yapko (1994a, 1994b) conducted one of the first surveys of memory beliefs of psychology professionals. He found that 34% (n = 190) of master’s-level psychotherapists and 23% (n = 48) of PhD psychotherapists agreed that traumatic memories uncovered via hypnosis are authentic. Moreover, 59% (n = 513) of clinicians agreed that “events that we know occurred but can’t remember are repressed memories” (Yapko, 1994a, p. 231). Yapko (1994a) also found that 49% (n = 419) agreed that “memory is a reliable mechanism when the self-defensive need for repression is lifted” (p. 232). Dammeyer, Nightingale, and McCoy (1997) found that 58% (n = 64) of PhD-level clinicians, 71% (n = 74) of PsyD-level clinicians, and 60% (n = 43) of MSW-level clinicians agreed that repressed memories are genuine. Merckelbach and Wessel (1998) detected an even higher percentage: 96% (n = 25) of licensed psychotherapists endorsed the view that repressed memories exist. Poole, Lindsay, Memon, and Bull (1995; Survey 2) found that 71% (n = 37) of clinical psychologists reported that they had encountered at least one case of a recovered memory (see also Polusny & Follette, 1996).
These studies were performed in the 1990s, which is considered to be the zenith of interest in repressed memories. After that period, a wealth of research published in psychological, psychiatric, and more legally oriented journals concluded that the notion of repressed memories is a highly problematic concept, particularly in the courts (Loftus, 2003; McNally, 2005; Piper et al., 2008; Porter, Campbell, Birt, & Woodworth, 2003; Rofé, 2008; Takarangi, Polaschek, Hignett, & Garry, 2008). Despite these critical articles, many psychologists, especially clinical and counseling psychologists, continue to harbor the idea that traumatic memories can be buried for years or decades in the unconscious and later recovered. Magnussen and Melinder (2012) surveyed licensed psychologists and found that 63% (n = 540) believed recovered memories to be “real.” Kemp, Spilling, Hughes, and de Pauw (2013) demonstrated that 89% (n = 333) of surveyed clinical psychologists believed that memories for childhood trauma (such as sexual abuse) can be “blocked out” for many years. Patihis et al. (2014) found that 60.3% (n = 35) of clinical practitioners and 69.1% (n = 56) of psychoanalysts agreed that traumatic memories are often repressed. Kagee and Breet (2015) found that 75.7% (n = 78) of 103 South African psychologists responded probably or definitely true to the statement that “individuals commonly repress the memories of traumatic experiences” (Kagee & Breet, 2015, p. 5).
Ost, Easton, Hope, French, and Wright (2017) showed that 69.6% (n = 87) of clinical psychologists strongly endorsed the belief that “the mind is capable of unconsciously ‘blocking out’ memories of traumatic events” (p. 60). Wessel (2018) recently examined memory beliefs among eye-movement desensitization and reprocessing (EMDR) practitioners. EMDR is thought to be effective in making traumatic memories less vivid and emotionally negative (Lee & Cuijpers, 2013). Wessel asked EMDR practitioners whether access to traumatic memories can be blocked and found that 93% (n = 457) responded affirmatively.
Beliefs among other professionals
Researchers have surveyed other professionals for whom it would be important to possess accurate knowledge concerning memory. Many of these studies did not specifically ask about professionals’ beliefs concerning the existence of repressed memories but instead asked about issues related to eyewitness memory (e.g., confidence-accuracy relationship; see Magnussen, Melinder, Stridbeck, & Raja, 2010). Exceptions to this trend include the study by Benton, Ross, Bradshaw, Thomas, and Bradshaw (2006). In an American sample, they demonstrated that 73% (n = 81) of jurors, 50% (n = 21) of judges, and 65% (n = 34) of law-enforcement personnel believed in long-term repressed memories. Odinot, Boon, and Wolters (2015) asked Dutch police interviewers about whether traumatic memories can be repressed. They found that 75.7% (n = 108) agreed that they could. In a recent study, 84% (n = 133) of Dutch child-protection workers indicated that traumatic memories are often repressed (Erens, Otgaar, Patihis, & De Ruiter, 2019).
Beliefs among laypersons
Laypeople such as undergraduates have also been asked in a number of studies to indicate their levels of belief concerning the existence of repressed memories (Lynn, Evans, Laurence, & Lilienfeld, 2015). Golding, Sanchez, and Sego (1996) reported that (a) 89% of 613 undergraduates were familiar with a circumstance in which someone recovered a repressed memory, (b) 75% of these students noted that the source of this information was television, and (c) belief in repressed memories was positively correlated with the amount of media exposure. Merckelbach and Wessel (1998) found that 94% (n = 47) of students endorsed the idea that repressed memories exist. Magnussen et al. (2006) surveyed 2000 Norwegian people from the general public. They found that 45% (n = 900) of respondents believed that traumatic memories can be repressed. Strikingly, 40% (n = 800) believed that people who committed a murder can repress the memory of that event. Finally, Patihis et al. (2014) found that 81% (n = 316) of undergraduates believed that traumatic memories are often repressed.
On the basis of these survey data, we calculated the overall percentage of people who believe in the existence of repressed memories in the combined samples (see Table 1). Although caution needs to be exercised when collapsing data across such surveys because the samples may vary on many dimensions, aggregated data can be informative given they can generally be expected to cancel out largely random differences in participant characteristics. On average, 58% (n = 4,745) of those who were surveyed indicated some degree of belief in the existence of repressed memories. When we examined the prevalence of these beliefs across subgroups within the combined sample, interesting results emerged. Among clinical psychologists, 70% (n = 2,305) believed in the existence of repressed memories. This percentage was somewhat lower in the 1990s (61%; n = 719) and increased to 76% (n = 1,586) from 2010 onward. Furthermore, 75% (n = 377) of other professionals expressed a strong belief in repressed memories, as did 46% (n = 2,063) of laypersons.
Table 1. Percentages of People Who Believe in the Concept of Repressed Memory Among Various Studies
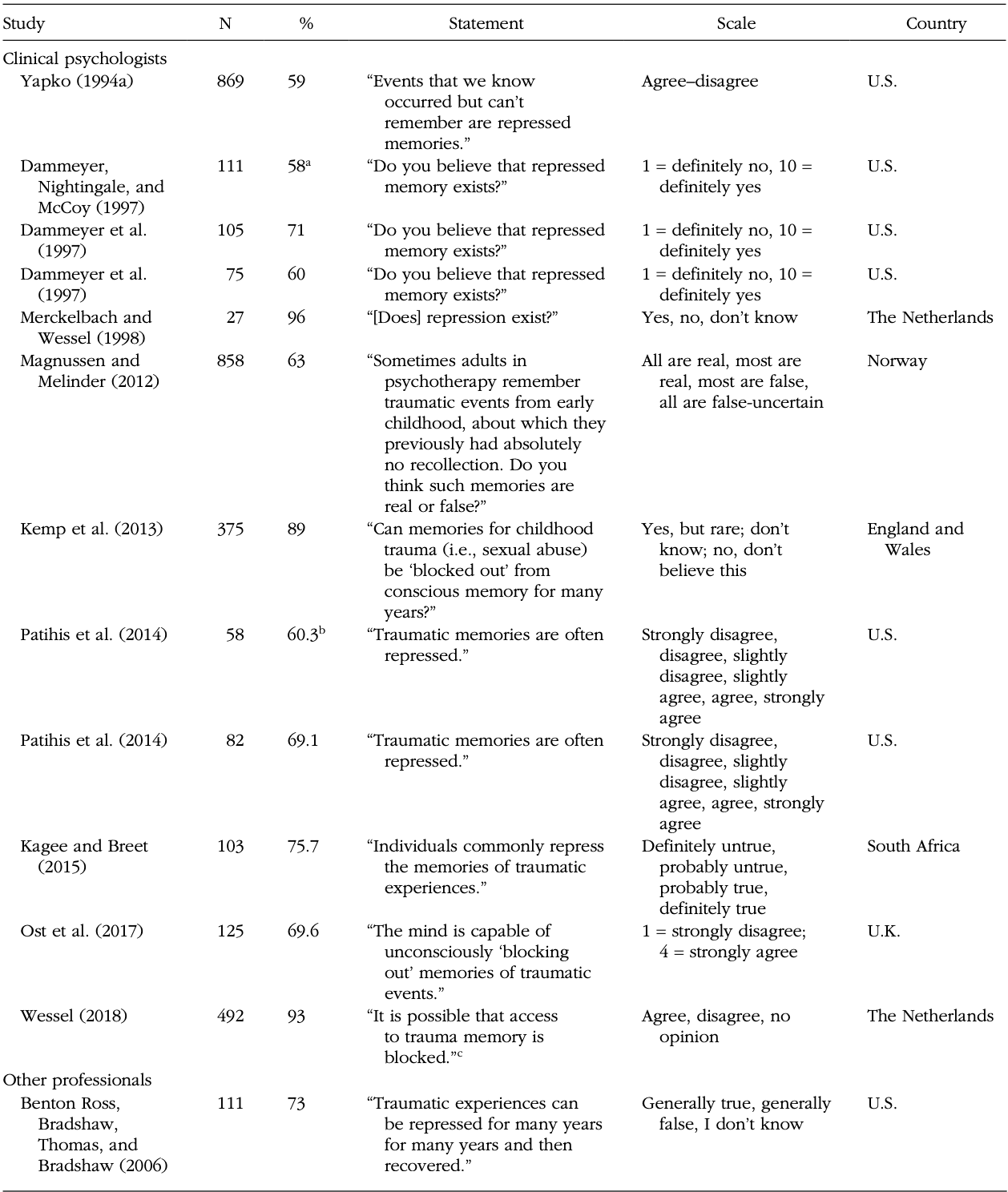
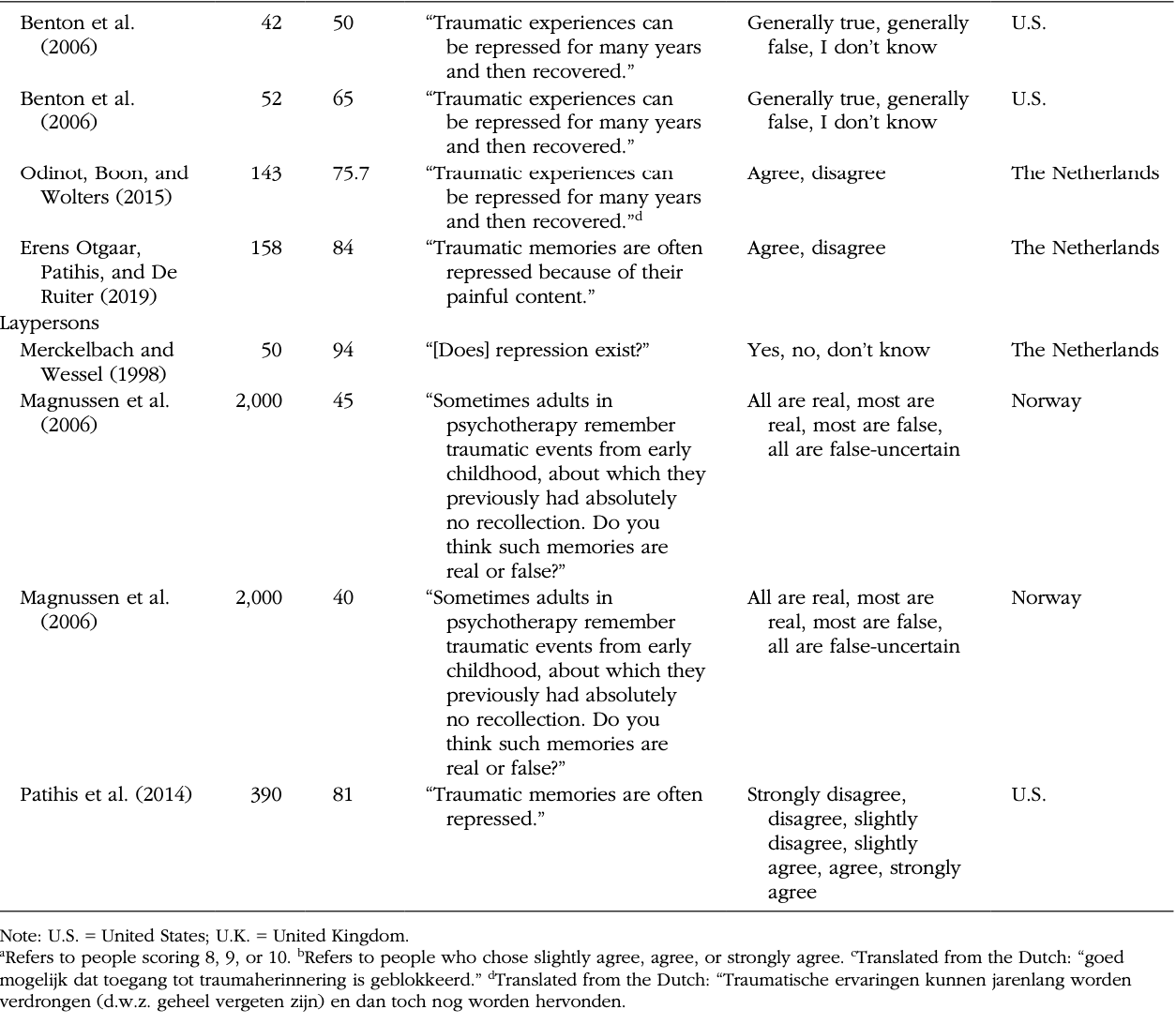
We also performed additional analyses. For example, when we focused only on survey items using the word “repression,” we found a prevalence of 65% (n = 1,265) in the belief of repressed memories. In addition, because the items used differed to some extent among survey studies, we concentrated on statements for which people were asked specifically about the frequency of repressed memories (e.g., “Traumatic memories are often repressed”). When we focused on these statements (Erens et al., 2019; Kagee & Breet, 2015; Patihis et al., 2014), we found that 78% (n = 618) of surveyed people believed that traumatic experiences are often repressed. We also compared the rates of belief in repressed memories in the 1990s with those of all studies performed after the 1990s. A prevalence of 62% (n = 766) was observed for studies in the 1990s; this rate was slightly lower for studies performed after the 1990s (57%; n = 3,979).
Taken together, our data suggest, perhaps surprisingly, that mental-health professionals in our combined samples were not more critical about repressed memories than were laypeople. This finding underscores our argument that a belief in repressed memories is deeply rooted in modern Western societies. Moreover, the data suggest that despite a plethora of scientific work calling the existence of repressed memories into question (e.g., Loftus & Davis, 2006), clinical psychologists’, other mental-health professionals’, and the general public’s views on repressed memories remain strong. Furthermore, it seems that belief in repressed memories even increased within clinical psychologists.
Still, in certain groups of professionals, notably those working in legal psychology, skepticism regarding repressed memories is high. For example, Kassin, Tubb, Hosch, and Memon (2001) found that 22% of experts opined that repressed memories are “reliable enough” to present as evidence in the courtroom. Likewise, some recent research suggests that memory scientists tend to harbor strong reservations concerning the existence of repressed memories (only 12.5% agreed that repressed memories can be retrieved in therapy accurately; 27.2% of experimental psychologists agreed to some extent that traumatic memories are often repressed; Patihis, Ho, Loftus, & Herrera, 2018). It is important to emphasize that many informed scientists are skeptical: It counters the argument that repressed memories must exist because so many people believe in them, a tempting logical error termed the bandwagon fallacy (Briggs, 2014).
Many of these surveys relied on the terms repression or repressed memories. These terms may have all kinds of connotations, leading to artificially raised endorsement patterns suggestive of belief in repressed memories. Brewin, Li, Ntarantana, Unsworth, and McNeilis (2019; Study 3) recently argued that high endorsement rates in the belief in repressed memories (to the statement “Traumatic experiences can be repressed for many years and then recovered”) actually reflect a belief in conscious memory suppression (see section below on retrieval inhibition). They found that when members of the general public were asked about their belief in conscious repression and were questioned regarding repressed memories (“Traumatic experiences can be repressed for many years and then recovered”), similar endorsement rates were found. However, because Brewin and colleagues did not include a survey item on unconscious repression, it is unknown which endorsement rates would be detected for such a controversial statement. To remedy this omission, Otgaar et al. (2019) specifically inquired about people’s belief in unconscious repression. They found high endorsement rates for belief in both conscious and unconscious repression (around 60%), implying that the belief in repressed memories is still widespread. In what follows, we show that, as is true for the belief in repressed memories, dissociative amnesia, a conceptual twin of repression, has been deeply embedded into psychology lore in such a way that it could be the most potent threat to extending the memory wars.
Dissociative Amnesia = Repressed Memories?
Despite the widespread belief in repressed memory, the term “repression” became controversial in the memory wars and is now seldom used in a credible context in scientific publications. After the concept became intensely controversial, many clinicians adopted a new and perhaps more palatable term dissociative amnesia. This term became the preferred and more widely used appellation for the process whereby traumas are rendered inaccessible. For example, dissociative amnesia is mentioned in DSM–5 (American Psychiatric Association, 2013), whereas repressed memory or repression is not.
There might be several reasons for why dissociative amnesia is listed in the DSM–5. One likely reason is that the substantial majority of the Task Force members of the DSM–5 were psychiatrists rather than psychologists, and the Task Force did not include memory experts (see Yan, 2007). This Task Force also did not adequately reflect the full range of scientific opinions regarding the empirical status of dissociative disorders, including dissociative amnesia. Indeed, as Lilienfeld, Watts, and Smith (2012) noted the following:
It is troubling that the DSM–5 Anxiety, Obsessive-Compulsive Spectrum, Posttraumatic, and Dissociative Disorders Work Group contains no members who have expressed doubts in scholarly outlets regarding the etiology of dissociative identity disorder and related dissociative disorders (e.g., dissociative amnesia, dissociative fugue), despite the fact that these disorders are exceedingly controversial in the scientific community. (p. 831)
Case studies of patients claiming dissociative amnesia have also figured prominently in the clinical literature, in turn perhaps contributing to the prima facie validity of the construct of dissociative amnesia (e.g., Staniloiu, Markowitsch, & Kordon, 2018).
We propose that during and after the 1990s, when the term repressed memory was widely criticized, proponents began to favor the term dissociative amnesia instead. Perhaps Holmes (1994) was one of the first to notice this trend:
In the absence of good laboratory or clinical evidence for repression, proponents of the concept have begun to emphasize dissociation instead. But that is simply another name for repression; if one dissociates oneself from an event (is no longer aware of it), one has repressed it. Dissociative amnesia is supposed to occur after certain traumatic experiences. Yet alleged cases of this phenomenon are very rare. (p. 18)
Consistent with this idea, dissociative amnesia was not mentioned in pre-1990s work on repression by Holmes (1972, 1974) and Holmes and Schallow (1969). This subtle but significant name change has muddied the waters and provided a cover for the continued practice of psychotherapy that involves repressed memories, albeit under new terminology.
Dissociative amnesia is defined in the DSM–5 as the “inability to recall autobiographical information” that (a) is “usually of a traumatic or stressful nature,” (b) is “inconsistent with ordinary forgetting,” (c) should be “successfully stored,” (d) involves a period of time when there is an “inability to recall,” (e) is not caused by “a substance” or “neurological . . . condition,” and (f) is “always potentially reversible because the memory has been successfully stored” (American Psychiatric Association, 2013, p. 298). These defining features serve as an umbrella set of criteria for three types of dissociative amnesia listed in the DSM–5. Localized dissociative amnesia applies to memory loss for a “circumscribed period of time” and may be broader than amnesia for a single traumatic event, for example, “months or years associated with child abuse” (p. 298). Because localized dissociative amnesia most resembles what was formerly called repressed memory, it is noteworthy that the DSM–5 calls this type “the most common form of dissociative amnesia.” In selective dissociative amnesia, the individual “can recall some, but not all, of the events during a circumscribed period of time” (p. 298). Generalized dissociative amnesia involves “a complete loss of memory for one’s life history” and “is rare” (p. 298). The DSM–5 indicates “histories of trauma, child abuse, and victimization” as features that support a diagnosis of dissociative amnesia (p. 299).
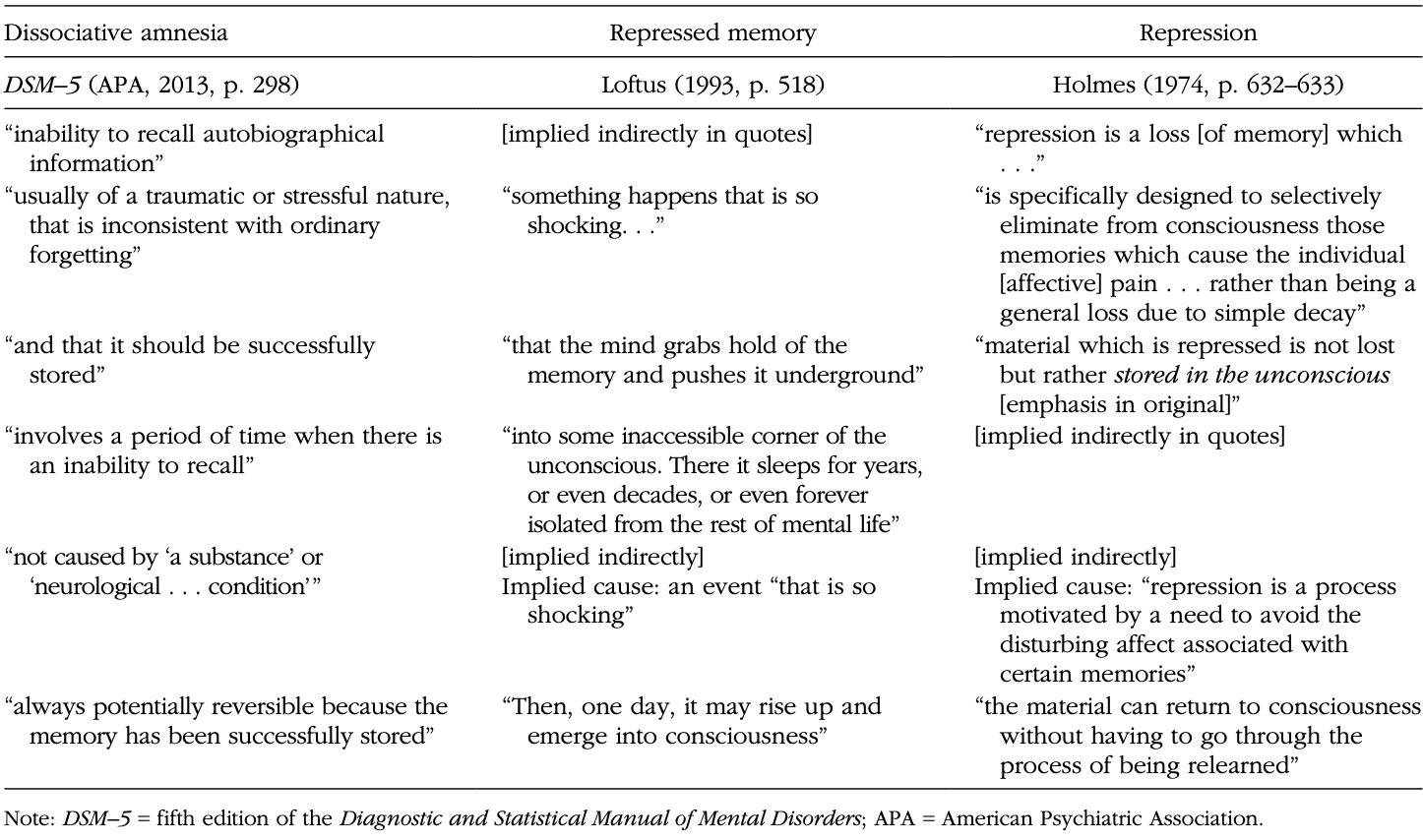
Although dissociative symptoms can manifest themselves in contexts quite different from trauma—for example, after the ingestion or administration of the anesthetic ketamine (Simeon, 2004) or ecstasy, cannabis, and cocaine (van Heugten-van der Kloet et al., 2015)—Table 2 illustrates similarities in the definitions of dissociative amnesia from the DSM–5 and definitions advanced by scientific skeptics of repressed memory (text from Loftus, 1993; and Holmes, 1974). We contend, on the basis of striking parallels in definitions, that skeptical arguments against repressed memories should apply with equal force to dissociative amnesia. More specifically, definitions of both dissociative amnesia and repressed memory share the idea that traumatic or upsetting material is stored, becomes inaccessible because of the trauma, and can later be retrieved in intact form.
Table 2. Side-by-Side Comparisons of the Definitions of Dissociative Amnesia and Repressed Memory
Although repressed memory as a concept is rarely defended in scientific circles these days, the idea of dissociative amnesia has become popular, especially in some psychiatric quarters. For example, between 2010 and 2019, the Journal of Trauma & Dissociation has published 71 articles related to dissociative amnesia; between 1990 and 1999, no such articles were published.2 This ascension appears to be a major reason for the revitalization of the memory wars and for the continuation of therapies that attempt to exhume traumatic memories. In the first two editions of the DSM (American Psychiatric Association, 1952, 1968), neither dissociative amnesia nor psychogenic amnesia was listed or mentioned, although dissociative types of neurosis were. Psychogenic amnesia first appeared in the third edition of the DSM (American Psychiatric Association, 1980; mentioned 19 times). Dissociative amnesia appeared for the first time in the fourth edition of the DSM (American Psychiatric Association, 1994; mentioned 50 times). In DSM–5, dissociative amnesia appeared 75 times (American Psychiatric Association, 2013). Interestingly, in no edition of the DSM have the words repress, repressed memory, or repression been used.
The DSM has codified and widely disseminated the concept of dissociative amnesia. In some quarters of psychology and psychiatry, dissociative amnesia is apparently taken as a valid and totally unproblematic concept (with notable exceptions; see Pope, Poliakoff, Parker, Boynes, & Hudson, 2007). Nevertheless, the definition of dissociative amnesia is scientifically fraught in many respects, just as is repressed memory. There are inherent problems when trying to ascertain whether a trauma has been stored but is nevertheless inaccessible. First, there is the complex problem of the lack of falsifiability: The only way we can determine whether a memory was stored is by memorial report, but a memorial report instantly disproves the claim that the memory is inaccessible. Second, it is difficult to test, or falsify, whether psychological trauma is the reason why an event is not remembered. How this is established depends in part on the theoretical orientation of the psychologist and whether she or he interprets an inability to recall as having been caused by psychogenic trauma or mundane encoding failures or forgetting mechanisms.
Indeed, one key question is whether cases that seem to document dissociative amnesia or repressed memory can be explained in terms of ordinary memory mechanisms. An example is provided by McNally (2003), who commented on two alleged cases of dissociative/psychogenic amnesia in children who had witnessed a lightning strike. McNally concluded that the memory loss could plausibly be explained by the fact that
both amnestic youngsters had themselves been struck by side flashes from the main lightning bolt, knocked unconscious, and nearly killed. Given the serious effects on the brain of being knocked unconscious by lightning, it is little wonder that these two children had no memory of the event. (p. 192)
The presence of a history of (mild) brain injury in case descriptions of patients diagnosed with dissociative amnesia has also been noted by other authors (Staniloiu & Markowitsch, 2014).
Consider another example that is illustrative of many similar clinical reports. Harrison et al. (2017) claimed to have documented 53 cases of, as the authors preferred to call it, “psychogenic amnesia.” These cases are cited by others as evidence for the existence of dissociative amnesia (Brand et al., 2018). Harrison et al. (2017) asked the amnesics several questions concerning their autobiographical memory. Note that none of these cases adequately satisfied the six tenets of dissociative amnesia discussed earlier. For instance, amnesia due to neurological damage, such as “traumatic brain injury” (American Psychiatric Association, 2013, p. 298), substance use, or other physical causes were not ruled out, which would preclude memory loss from being diagnosed in the DSM–5 as dissociative amnesia. The possibility of head injury causing memory impairment is particularly relevant here, especially because Harrison et al. found that a history of head injury was common in the “psychogenic” cases. In addition, Harrison et al. did not establish whether psychological shock or trauma caused the reported memory problems or that any recalled memories really were inaccessible for a period of time (see also Patihis, Otgaar, & Merckelbach, 2019).
Another issue is that Harrison et al. (2017) did not exclude the possibility that the dissociative amnesia was the result of feigning. This omission is remarkable because many of the patients with dissociative amnesia described by these authors were plagued by financial problems, and it would have been relatively easy to administer symptom-validity tests to them. With these tests, one can gauge whether patients endorse atypical or bizarre symptoms in an attempt to exaggerate their problems (Lilienfeld, Thames, & Watts, 2013; Peters, van Oorsouw, Jelicic, & Merckelbach, 2013). Other authors have found that overreporting of bizarre and implausible symptoms (e.g., “When I hear voices I feel as though my teeth are leaving my body”) is prevalent among those who claim dissociative amnesia (Cima, Merckelbach, Hollnack, & Knauer, 2003). Claiming dissociative amnesia is not the same as suffering from it (see also Peters et al., 2013). With this consideration in mind, Staniloiu and Markowitsch (2014) acknowledged in their review article that “the main challenge posed by the differential diagnosis of dissociative amnesia is to distinguish between true and feigned or malingered amnesia” (p. 237).
Key to our argument is that the evidence that scholars put forward for dissociative amnesia is typically subject to more plausible explanations. McNally (2007) listed several alternative and perhaps more plausible interpretations of the evidence for dissociative amnesia. First, memory problems that emerge after trauma might be caused by everyday forgetfulness and should not be confused with amnesia for the trauma. Second, some dissociative-amnesia theorists have confused organic amnesia with dissociative amnesia. Third, people who have experienced trauma and cannot recollect all of it might have failed to encode relevant parts of the traumatic experience. Fourth, victims of abuse commonly fail to disclose the abuse (e.g., because they feel ashamed), a reporting decision that should not be confused with dissociative amnesia. Fifth, when people cannot recollect any events (even traumatic ones) before the age of about 3 years old, it likely reflects the well-established phenomenon of childhood amnesia (Fivush, Haden, & Adam, 1995; Howe, 2013) rather than dissociation. Sixth and finally, victims of abuse understandably often do not want to think about their traumatic experiences but often cannot help it because of flashbacks and intrusive memories. This phenomenon of suppression should not be confused with repression, and it falls well outside the domain of dissociative amnesia.
The Purported Empirical Evidence for Repressed-Memory Mechanisms
Three main areas of research are typically used to support repressed memories or dissociative amnesia: retrieval inhibition, motivated forgetting, and the relation between trauma and dissociation. Nevertheless, none of them fully supports all six parts of the definition of either concept shown in Table 2.
For example, the phenomenon of retrieval inhibition (M. C. Anderson & Green, 2001; Anderson & Hanslmayr, 2014; M. C. Anderson et al., 2004) suggests that some mechanism inhibits some memories whereas others come to consciousness, and that trying not to think about a memory can make it harder to remember. However, this phenomenon does not meet the six tenets of dissociative amnesia, such as the principle that the event is often traumatic in nature (see also Kihlstrom, 2002). Likewise, some research has shown limbic inhibition via the frontal cortex among individuals with a subtype of PTSD that involves emotional suppression (Lanius et al., 2010). Although interesting, cases of PTSD involving inhibited emotions do not establish that a memory is stored, that it is inaccessible because of trauma and then later becomes accessible. One can inhibit one’s emotions regarding a painful memory while retaining a full recollection of this memory.
Other research has shown that alleged cases of dissociative amnesia were accompanied by increased prefrontal cortex activity and decreased activation of the hippocampus when patients were exposed to stimuli (i.e., certain faces) for which they had reported amnesia (Kikuchi et al., 2009). However, it would be premature to interpret this study as evidence for repressed/dissociated memories. Before concluding that dissociative amnesia is involved, it is imperative to rule out other possible plausible explanations, such as feigned amnesia, which was not investigated in this work. This is all the more remarkable because one of the patients who claimed to be amnesic was worried about his impending marriage, whereas the other patient took a leave of absence from work after he had been involved in an accident.
Retrieval inhibition has been suggested to be “a viable model for repression” (M. C. Anderson & Green, 2001, p. 366). The canonical paradigm used to evaluate retrieval inhibition is the think/no-think paradigm (M. C. Anderson & Green, 2001). In the original version, participants see several unrelated word pairs (e.g., ordeal-roach). After seeing these stimuli, participants are presented with cue words (e.g., ordeal) and are instructed to either recall the associated word (think) or not (no-think). When participants are asked to recall all response words during the presentation of cue words, no-think response words are remembered less accurately. A meta-analysis showed that no-think words were associated with lower recall rates than items that were studied but not asked about during the think/no-think phase (8% reduction; M. C. Anderson & Huddleston, 2012). One problem with this meta-analysis is that no unpublished studies from other labs were included, raising the specter of file-drawer effects and therefore inflated effect sizes. In fact, Bulevich, Roediger, Balota, and Butler (2006) conducted three experiments that failed to replicate the think/no-think memory-suppression effect and noted that “while working on this project, we have become aware of other groups of researchers who have failed to replicate the original M. C. Anderson and Green (2001) results, although most have given up and not attempted to publish their results” (p. 1574). Other memory researchers have recently pointed to unpublished studies that failed to replicate the original think/no-think finding (A. J. Barnier, personal communication, November 17, 2018; I. Wessel, personal communication, January 10, 2019).
Our argument is that the following two research lines are needed in the area of the think/no-think memory-suppression effect. First, empirical work is necessary on the relation between trauma and memory suppression. To date, there is only limited work in this specific domain. For example, Hulbert and Anderson (2018) found that students reporting a greater history of trauma showed more memory suppression than did students who reported having little experience with trauma. Although interesting, this research does not causally establish whether trauma led to more memory suppression. Second, a multicenter replication attempt would yield critical information regarding the robustness, reliability, and potential boundary conditions of the think/no-think memory-suppression effect.
Motivated forgetting of trauma-related words in the directed-forgetting paradigm is another technique held up to support dissociative amnesia (as argued by DePrince et al., 2012 as part of betrayal trauma theory). For example, DePrince and Freyd (2001) argued they had adduced evidence for motivated forgetting in dissociated individuals. In this study, participants scoring low and high on the dissociative-experiences scale (DES; E. M. Bernstein & Putnam, 1986) received several words (trauma-related and neutral) and after each word were instructed to remember or forget the word. The authors found that under divided-attention conditions, participants scoring high on dissociation recalled fewer trauma-related and more neutral words than those scoring low on dissociation. Still, several other researchers could not replicate these results (e.g., Devilly et al., 2007; Giesbrecht & Merckelbach, 2009; McNally, Metzger, Lasko, Clancy, & Pitman, 1998). In recent research, Patihis and Place (2018) found only weak evidence supporting the hypothesis that traumatized and dissociated individuals would forget trauma-related words; only one of eight hypotheses predicted support for differential motivated forgetting. Patihis and Place (2018) pointed out the high number of “degrees of freedom” available to researchers to choose comparisons in such directed-forgetting experiments. As they noted:
Within a given data set, researchers can attempt to demonstrate differential forgetting between the To Be Remembered lists and the To Be Forgotten lists. If that fails they can compare trauma to positive or neutral words. If that fails they can look for statistical significance in several interactions—and they can make all these comparisons with a number of categorisations: on dissociation, trauma, diagnosis, acute stress, which all provide additional degrees of freedom. Given the number of possible combinations, a motivated researcher will likely be able to find one comparison that might be interpreted as motivated forgetting. (p. 630)
Even if this paradigm could consistently reveal that trauma words are remembered less well by dissociated individuals, it would not be evidence that a trauma can be stored and become both inaccessible and ultimately retrievable with accuracy. Furthermore, there is work showing that even directed forgetting of autobiographical memories is not significantly related to the emotional valence of these memories, a finding that runs counter to the expectation that trauma should lead to a distinctive repression effect on memory (Barnier et al., 2007). Despite many assertions in the literature to the contrary, directed-forgetting research provides no compelling evidence for repressed memories or dissociative amnesia. On a more general note, researchers have noted that the memory-impairing effects of directed forgetting may be due to a lack of rehearsal, thereby negating the need to invoke repressed memories (Roediger & Crowder, 1972).
In addition, researchers have heralded the statistical correlation between trauma and dissociative symptoms as support for a general theory that trauma can lead to dissociative amnesia (see Dalenberg et al., 2012, 2014; but see Lynn et al., 2014). However, even if this relation is strong—typically it is not (see Patihis & Lynn, 2017)—this does not establish evidence for dissociative amnesia. Dissociation, as measured by the widely used DES, assesses feelings of depersonalization, derealization, and memory problems. These symptoms are not unlikely correlates of being traumatized or stressed for a period of time. Nevertheless, the DES does not assess dissociative amnesia as it is defined in the DSM–5, despite the use of the word “dissociative.” Specifically, the dissociative-amnesia subscale of the DES (e.g., Stockdale, Gridley, Balogh, & Holtgraves, 2002) contains items such as “finding oneself in a place, but unaware how one got there,” “finding oneself dressed up in clothes one can’t remember putting on,” “finding unfamiliar things among one’s belongings,” “not recognizing friends or family members,” and “no memory of some important personal events (e.g., graduation)” (E. M. Bernstein & Putnam, 1986; pp. 733–734). These items do not describe dissociative amnesia and do not assess reactions to trauma and stored yet inaccessible memories. Rather, they might reflect poor attentive control and commonplace cognitive failures. Indeed, studies have found that in undergraduate samples, scores on the amnesia items of the DES correlate positively and significantly with a measure of poor attentive control—that is, cognitive failures (Merckelbach, Muris, & Rassin, 1999: Study 1, r = .49; Study 2, r = .36; see also Merckelbach et al., 2000); for replication in nonclinical groups, see Bruce, Ray, and Carlson (2007: r = .31–.46).
The picture we have so far does not imply that dissociation is unrelated to memory. Our position is that trauma can sometimes lead to feelings of depersonalization and that, probably because of accompanying stress levels, memory problems might arise. However, this position does not favor the existence of dissociative amnesia, which implies that memories of entire autobiographical experiences have been temporarily inaccessible and can later be completely and accurately recovered (see also Patihis et al., 2019). It is true that some earlier studies (e.g., Eich, Macaulay, Loewenstein, & Dihle, 1997) found suggestive evidence for interidentity amnesia in patients with dissociative identity disorder (DID). However, a more recent series of studies by Huntjens and colleagues demonstrated the importance of distinguishing between what people subjectively report about their memory loss and (the absence of) objective manifestations of such loss. Huntjens, Verschuere, and McNally (2012) assessed the transfer of information between personality states in patients with a diagnosis of DID. Both tests of explicit and implicit memory were included, as well as neutral, emotional, and autobiographical information. The data across studies were consistent in that, subjectively, DID patients reported amnesia between their personality states, but objectively, no evidence emerged for interidentity amnesia (e.g., Dorahy & Huntjens, 2007; Huntjens et al., 2012).
Psychotherapeutic Techniques, Memory Distortions, and Other Side Effects
We now consider the role of therapy in the emergence of repressed memories. We discuss research on how often therapists suggest to clients that they might have repressed memories, the effects of therapy on (false) memory, and the link between psychopathology and (false) memory recovery.
Reports of recovered memories in therapy
We have shown that a large percentage of clinical psychologists continue to believe that repressed memories might occur when people are faced with trauma. A pivotal point here is to know whether such beliefs bear any ramifications in therapeutic contexts. Patihis and Pendergrast (2019) surveyed 2,326 U.S. citizens about memory recovery in psychotherapy. Nine percent (n = 217) of the sample reported that their therapists had discussed the possibility that they (the client) had repressed memories of childhood abuse. Furthermore, those participants were 20 times more likely to report recovering memories of abuse in therapy (that they were unaware of before therapy) than participants whose therapists did not discuss the possibility of repressed memories. Five percent (n = 122) of the public sample reported that in the course of therapy, they had memories of being abused, of which they had no previous memory. Therapists who reported recovering memories engaged in a wide range of therapies, from attachment therapy to cognitive-behavioral therapy. In most therapy types, participants indicated a minority of therapists had discussed the possibility of repressed memories. For some therapies that involve working through past trauma, this occurred more frequently (e.g., attachment therapy, EMDR).
The study by Patihis and Pendergrast (2019) concerned recovered memories in the United States; however, Shaw, Leonte, Ball, and Felstead (2017) examined the frequency of repressed and recovered memories in the United Kingdom. They analyzed cases from the British False Memory Society, which is a charity that supports individuals claiming to have been falsely accused of a crime on the basis of a false memory. The society database contains more than 2,500 cases since 1993. The researchers selected a random sample from the database and found that 84.3% (n = 153) of daughters accusing fathers were said to have undergone a form of therapy ranging from standard psychotherapy to hypnosis. Furthermore, Shaw and Vredeveldt (2019) noted that the Dutch equivalent of the British False Memory Society, the Fictitious Memory Group, received 13 new possible false-memory cases from 2011 and 2018. Importantly, in 77% (n = 10) of these cases, alleged victims underwent some form of therapeutic intervention (e.g., EMDR, reincarnation therapy).
In Germany, a similar false-memory group called False Memory Deutschland (2019) maintains an archive containing cases of individuals claiming to have been falsely accused on the basis of recovered memories of sexual abuse. This group states on its website that at the time of the accusations, 83% (n = 81) of alleged victims had been receiving psychotherapy. Even more interesting, the number of accusations has increased since 2002. All in all, reports of repressed memories in therapy occur on a nontrivial scale and can be found in many different countries. Of course, here too, the data should be interpreted with caution because selection biases might play a role. Still, the data provide additional evidence that the issue of repressed memories has not disappeared, and there are even some indications that that it has made a resurgence, at least in some areas (see also below).
Therapy and side effects
One of the most important hypotheses underlying the memory wars was that during psychological treatment, some therapists suggested to clients that they had repressed a memory of trauma, which might have engendered false memories. Although experimental work has confirmed that suggestive questions can elicit false memories (Scoboria et al., 2017), a paucity of systematic research exists on how therapy shapes memory. Goodman, Goldfarb, Quas, and Lyon (2017) investigated whether therapy during a child sexual-abuse prosecution predicted memory consistency (10–16 years later). Interestingly, the authors found that therapy use positively correlated with memory consistency. Specifically, alleged victims who received therapy during or shortly after the prosecution were more likely to correctly remember abuse-related details (e.g., name of the perpetrator, perpetrators’ age) than those who did not. The use of nonsuggestive psychotherapy may aid memory consistency rather than hinder it. However, consistent remembering is not the same as accurate remembering (Smeets, Candel, & Merckelbach, 2004; Talarico & Rubin, 2003).
Nevertheless, Goodman et al. (2017) did not specifically assess whether the type of therapy used was related to memory accuracy, and no causal conclusions concerning the effect of therapy on memory accuracy could be drawn from their study. Establishing a causal relation is important because some therapies, such as EMDR and psychoanalytic therapies, rely on patients retrieving specific autobiographical memories, and hence there might an increased risk of false memories. Furthermore, an important issue is whether certain therapies might increase people’s proneness to acquiesce with suggestions and form false memories. Indeed, Goodman et al. (2017) argued that “a study using an experimental design with random assignment to groups to investigate the effects of therapeutic intervention on true and false memory for traumatic events would be a welcome contribution to this important field of study” (p. 929). Houben, Otgaar, Roelofs, and Merckelbach (2018) addressed this issue by examining the effect of eye movements as provided in EMDR on false-memory formation (i.e., reporting of misinformation). Participants who received eye-movement treatments were more susceptible to creating false memories than participants who did not receive eye-movement treatments. Presumably, eye movements degraded memory, which might make people more susceptible to accept external misleading information—which could result in false memories (but see also van Schie & Leer, 2019). So, although eye movements as in EMDR may improve memory retrieval (e.g., Lyle, 2018), they might also increase people’s willingness to accept external suggestions.
In addition to focusing on the effects of therapy on memory performance, it is imperative to examine unwanted side effects of psychotherapy as reported by the therapists and patients themselves. Although this work is limited, research has shown that psychotherapy can in some cases engender negative side effects (Lilienfeld, 2007; Merckelbach, Houben, Dandachi-Fitzgerald, Otgaar, & Roelofs, 2018; Rozental et al., 2018). Of special interest are studies that examined the relation between therapy and memory. For example, Rozental, Kottorp, Boettcher, Andersson, and Carlbring (2016) surveyed participants who had been in treatment for social anxiety and found that the most frequently endorsed side effect of treatment was “unpleasant memories resurfaced” (n = 251; 38%).
Especially relevant are studies examining what happened after clients recovered memories via therapy. Fetkewicz, Sharma, and Merskey (2000) noted that suicide attempts increased after patients received recovered-memory therapy, although the absence of a comparison group of patients who did not receive such interventions mitigates their conclusions. Loftus (1997) observed a similar pattern with patients who received compensation after recovering memories in therapy. Before memory recovery, 3 patients (10%) reported thinking about committing suicide, whereas after recovery 20 patients (67%) reported being suicidal. Of course, it cannot be concluded that this specific therapy caused these suicide attempts or feelings, but it is concerning that patients can become more symptomatic after such therapeutic interventions. Collectively, research on the negative side effects of therapy, although limited in quantity, suggests that negative effects of therapy may not be negligible and that memory recovery may play a role in deterioration.
Psychopathology and false memory
Another way to examine the role of therapy in the reported unearthing of repressed memories is to determine whether people with some form of psychopathology are at higher risk for false memories than are people without psychopathology. This information is vital because people might seek an explanation for their disorder in therapy (cf. “effort after meaning,” Bartlett, 1932), and therapists might actively search for such explanations in patients’ memories and thereby create a springboard for false memories. Authors have voiced differing opinions with regard to the relation between psychopathology and false-memory generation. For example, Bookbinder and Brainerd (2016) stated that “with respect to PTSD especially, available data do not provide a consistent picture of false memory effects” (p. 1345). In contrast, Scoboria et al. (2017) opined that “people struggling with psychopathology who seek help for their symptoms may be particularly vulnerable to suggestions” (p. 160).
Otgaar, Muris, Howe, and Merckelbach (2017) recently reviewed the body of empirical work related to psychopathology and false-memory creation. Specifically, they focused on false-memory effects in people with PTSD, depression, and a history of trauma and found that in most of these studies, researchers used the Deese/Roediger-McDermott (DRM) false-memory paradigm (Deese, 1959; Roediger & McDermott, 1995). In this paradigm, participants receive word lists containing associatively related words (e.g., night, pillow, moon). During recall and recognition tasks, participants frequently misremember a related but not presented word called the critical lure (in this case, sleep). Otgaar, Muris, et al. (2017) also included experiments that relied on emotionally charged word lists related to some aspects of the participants’ psychopathology. For example, for patients with depression, lists could be used that focused on the word sad. The general finding from the review was that people with PTSD, depression, or a history of trauma were at increased risk of forming false memories when they received word lists linked to their symptoms (see also Howe & Malone, 2011). There is good evidence that certain forms of psychopathology (e.g., schizophrenia) go hand in hand with a tendency to accept and give in to external pressure (Peters, Moritz, Tekin, Jelicic, & Merckelbach, 2012). More importantly, existing work also indicates that psychopathology (i.e., depression, PTSD) is linked to an enhanced propensity to produce spontaneous false memories.
The implications of this review should be drawn with care, however, because spontaneous false memories as induced by the DRM paradigm are typically weakly related or even unrelated to false memories induced by suggestion (e.g., D. M. Bernstein, Scoboria, Desjarlais, & Soucie, 2018; Calado, Otgaar, & Muris, 2019; Nichols & Loftus, 2019; Ost et al., 2013; Otgaar & Candel, 2011; Patihis, Frenda, & Loftus, 2018; Zhu, Chen, Loftus, Lin, & Dong, 2013). So, although psychopathology seems to be related to an increased vulnerability for spontaneous false-memory production, this does not necessarily imply that it is also linked to an increased susceptibility to suggestion-induced false memories.
The Creation of Implanted False Memories
Many battles of the memory wars revolved around the issue of therapists who informed patients that they had repressed memories of childhood. The fact that some therapists suggested to patients that they had been sexually abused raised concerns regarding false memories in psychotherapy (Loftus, 1994) as well as whether suggestive therapeutic interventions could fuel false-memory formation. Focusing on cases in which recovered memories surfaced, researchers began to examine the conditions, such as the types of events suggested, under which false events could be inadvertently implanted in memory. Specifically, a question that was addressed was whether false events could be implanted and whether even emotionally negative false memories could be formed.
False events and implanted false memories
Researchers have used the false-memory-implantation paradigm to demonstrate that entire events, ranging from positive (e.g., a birthday party) to negative (e.g., getting lost in a shopping mall), can be implanted. In the false-memory-implantation paradigm (Loftus & Pickrell, 1995), participants are asked what they can remember about a true experienced event and a false event. Participants are (falsely) told that their parents confirmed that these events were experienced by the participants. During multiple suggestive interviews, about 30% of participants claim to remember the false event (Scoboria et al., 2017). Studies that have successfully implanted negative events bear special relevance to the claim that recovered memories of abuse may be instances of rich false memories.
For example, Hyman et al. (1995) found in their implantation study that at the second suggestive interview 10% (n = 2) of their subjects falsely remembered that they spent a night at the hospital because of a high fever and an ear infection. Loftus and Pickrell (1995) showed that 25% (n = 6) of their sample created false memories of being lost in a shopping mall. Porter, Yuille, and Lehman (1999) implanted several negative events (i.e., getting lost, serious medical procedure, getting seriously hurt by a child, animal attack, indoor accident), and percentages of implantation ranged from 16.7% (n = 3; getting lost) to 36.8% (n = 7; animal attack). Shaw and Porter (2015) found that 70% (n = 21) of participants formed false memories of committing a crime (but see Wade, Garry, & Pezdek, 2018, who used another scoring method and reported that only 26% to 30% of Shaw and Porter’s subjects formed false memories).
Of course, the events that have been implanted in experimental studies on false memories differ in various ways from recollected events in real cases (e.g., sexual abuse), which almost always involve feelings of shame and taboo (Goodman, Quas, & Ogle, 2010). Indeed, when Pezdek, Finger, and Hodge (1997) attempted to implant an experience of a rectal enema in adult participants, none of them fell prey to the suggestion. However, this is not to say that such events cannot be implanted in memory. Otgaar, Candel, Scoboria, and Merckelbach (2010) found that during the second interview, six children (10%) falsely reported having received a rectal enema (see also Hart & Schooler, 2006). Furthermore, in general, research suggests that negative events are more likely to be misremembered than are more mundane events (e.g., Otgaar, Candel, & Merckelbach, 2008; Porter, Taylor, & ten Brinke, 2008). This finding has been explained by the fact that because emotionally negative memories contain a high level of connectivity with other memories, it is relatively easy to activate and then remember events that were not experienced but related to the experienced event (e.g., Bookbinder & Brainerd, 2016; Otgaar, Merckelbach, et al., 2017).
Although one could argue that the type of events implanted in false-memory research do not match events of interest in legal cases, in false-memory-implantation studies, participants are generally interviewed two or three times in a suggestive fashion, whereas legal cases often drive home the point that people with false memories received suggestive interviews by therapists over the course of years (Maran, 2010; van Til, 1997). It seems safe to assume that with enough suggestive pressure, even extreme negative events may be implantable in memory.
Estimating the prevalence of false-memory implantation
Researchers have tried to estimate the percentage of individuals who develop false autobiographical memories in the laboratory. Such experiments have mainly involved healthy undergraduate students who are confronted with suggestive information, after which their memory reports are evaluated for indications of accepting false information. Attempting to come up with an accurate estimate is, however, a daunting task because studies differ in terms of coding and criteria for defining a report of false memory. Brewin and Andrews (2017) reviewed false-memory-implantation studies and concluded that in 15% of the recollective experiences induced by the implantation method, statements were rated as full-blown false memories. They argued that this statistic shows that “susceptibility to false memories of childhood events appears more limited than has been suggested” (p. 2).
Nevertheless, the review by Brewin and Andrews (2017) has been criticized (for a critical analysis, see Otgaar, Merckelbach, et al., 2017). First, as mentioned previously, the coding of false memories varied among false-memory-implantation studies. Therefore, Scoboria et al. (2017) devised a new coding system based on theories concerning remembering (e.g., Brewer, 1996; Conway & Pleydell-Pearce, 2000; Johnson, Hashtroudi, & Lindsay, 1993; Rubin, 2006). Using this system, they recoded transcripts from eight published false-memory-implantation studies. Overall, they found that 30.4% of transcripts were coded as false memories, which is twice the percentage that Brewin and Andrews (2017) reported. In addition, in the analysis by Scoboria et al., an additional 23% of cases were coded as having accepted the false event to some extent.
Second, Otgaar, Merckelbach, et al. (2017) reviewed 15 false-memory laboratory studies that investigated the confidence that participants place in their false memories. The data revealed a mean confidence rating of 74%, with an unweighted 95% confidence interval = [0.66, 0.78].3 Furthermore, in 93% (k = 14) of the studies, false-memory reports had confidence ratings exceeding the midpoint of the rating scale. Clearly, confidence is often high in implanted false memories.
Third, even if we accept the highly conservative 15% as a fair estimate of overall false-memory potential, this percentage still points to a significant problem in legal and therapeutic settings. It means that if a therapist using suggestive prompts consulted with 100 patients, on average, 15 of them might develop illusory autobiographical memories of, for example, sexual abuse, and some might falsely accuse an innocent person because of this memory (Nash, Wade, Garry, Loftus, & Ost, 2017; see also Smeets, Merckelbach, Jelicic, & Otgaar, 2017).
Memory Wars in the Courtroom and Beyond
We have reviewed several lines of evidence showing that the topic of repressed memories continues to be popular although scientifically controversial among psychologists and psychiatrists. We now examine the role of repressed memories and dissociative amnesia in legal cases and the persistence of naive memory beliefs in the courtroom.
Repressed memories and dissociative amnesia in the courtroom
In 2017, a French ministerial report was published proposing to increase the statute of limitations for prosecuting sexual abuse from 20 to 30 years (Flament & Calmettes, 2017). The reason given was that because victims often delay disclosing their abusive experience (e.g., Goodman-Brown, Edelstein, Goodman, Jones, & Gordon, 2003; see also Connolly & Read, 2006), they are still entitled to have their day in court. However, a more controversial reason for increasing the statute of limitations given in the report was that traumatic experiences of abuse could lead to dissociative amnesia (Dodier & Thomas, 2019). Dodier and Thomas rightly noted that the use of such a controversial term in an official governmental report might lead people with a history of trauma to believe that their traumatic memories are atypical and that to uncover additional memories they should rely on methods such as recovered memory therapy that might result in false memories. Admittedly, victims might take many years to disclose their traumatic experiences, but as noted before, there are more plausible explanations than dissociative amnesia for the delay in reporting the abuse, such as feeling ashamed of the trauma and reinterpreting the experience as abusive (e.g., Goodman-Brown et al., 2003; Schooler, 2001). This issue of delayed disclosure is especially relevant to stress, as there is currently much attention regarding historic sexual abuse cases, such as those that emerged in the #MeToo discussion, of which the overwhelming majority has nothing to do with memory repression or recovery (see also Goodman et al., 2017).
There is also evidence of recovered memories entering into some cases in the United Kingdom. The UK Advocate’s Gateway (2015) document on trauma explains to lawyers how to approach traumatized witnesses and victims. It stipulates that dissociative amnesia is possible and argues that “Trauma disrupts the left hemisphere function of the brain. . . . This disruption affects the ability to give a verbal narrative. . . . The right hemisphere of the brain stores implicit or sensory associated memories” (p. 5). This is questionable advice, with some potentially unsupported and pseudoscientific ideas mixed into the document.
An alternative way to examine whether the issue of repressed memories and dissociative amnesia is still prominent in the legal arena is to examine court proceedings and investigate the number of cases in which repressed memories played a role. In the Netherlands, an online database of court rulings (http://www.rechtspraak.nl) exists in which one can search for key terms in a diverse set of cases. The database is not exhaustive in that it only lists the most prominent court rulings. We used the search term verdringing (“repression”) and investigated criminal trials from 1990 to 2018 in which repressed memories were mentioned. Figure 1 demonstrates that cases in which this term was used referring to cases on repressed memories have increased over the past years. When a similar exercise was performed using the search term hervonden herinnering (“recovered memory”), a similar pattern emerged. Moreover, when we used the term dissociatieve amnesia (“dissociative amnesia”), again, we found that this term is on the rise.
Fig. 1. Number of Dutch legal cases mentioning repression, recovered memory, or dissociative memory from 1990 to 2018.
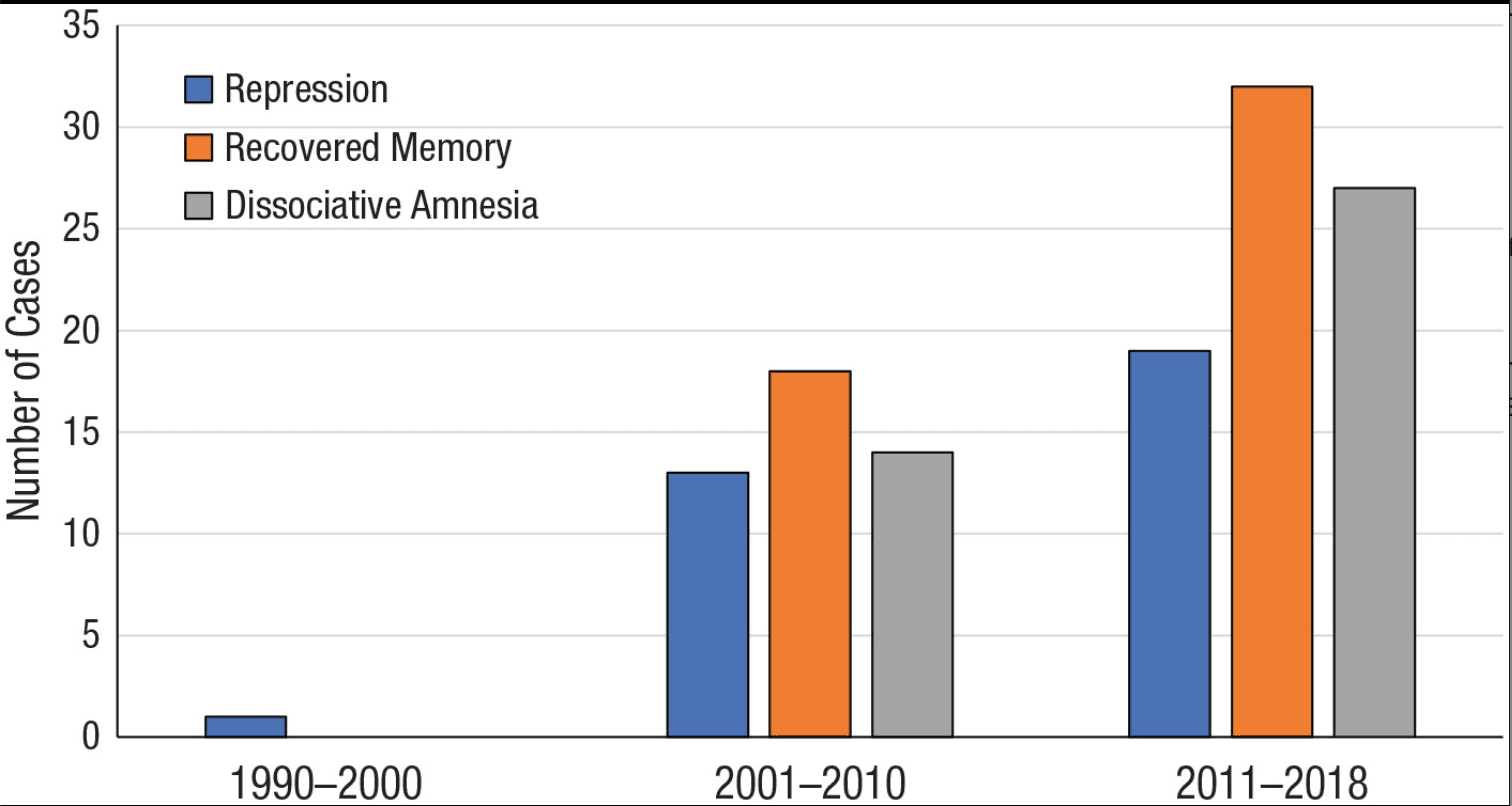
Caution should be exerted when interpreting these data. First, it is remarkable that virtually no legal cases were found on repression and recovered memory from 1990 to 2000. One reason might be that such older cases are not represented in this database. Second, although issues such as repressed and recovered memories were discussed in these criminal trials summarized by pertinent court rulings thereafter, judges did not necessarily accept these notions uncritically. Nonetheless, these data demonstrate that, at least in the Netherlands, legal professionals still use the Freudian and neo-Freudian nomenclature of repression and dissociative amnesia.
Memory beliefs in the courtroom
Although we have discussed naive beliefs about memory across a variety of lay and professional populations, these beliefs can be especially problematic in the courtroom. Because judicial outcomes may be influenced by the naive beliefs about memory that triers of fact harbor, it is critical that when testimony consists mainly of memory evidence (e.g., remembering event details, identifying the perpetrator), actors in the legal domain possess a scientifically informed view of how memory works.
To appreciate how the disconnect between the science of memory and the beliefs held by individuals in the legal arena can lead to unsafe convictions, one can examine the cases listed on the Innocence Project websites in the United States (http://www.innocenceproject.org) and the United Kingdom (http://www.innocencenetwork.org.uk). The most common factor in these false convictions has been faulty memory evidence (i.e., incorrect eyewitness identifications are implicated in more than 70% of cases). Police and prosecutors apparently made decisions about this memory evidence perhaps without exactly understanding the science of how memory works and often because other more objective evidence was lacking (for reviews, see Howe & Knott, 2015; Howe, Knott, & Conway, 2018).
Judges and prosecutors alike differ as to whether they will accept expert memory testimony. For example, in a Dutch revision case in which dissociative memories of abuse were the central issue, one senior prosecutor opined that in contrast to DNA experts, psychological experts do not aid judges in helping them to understand the intricacies of statements by witnesses or defendants (https://uitspraken.rechtspraak.nl/inziendocument?id=ECLI:NL:PHR:2015:2769). He added that the field of legal psychology is known for its lack of consensus and for its high degree of subjectivity, which is hyperbolic when one looks at the generally broad consensus on a range of topics found in surveys among legal psychologists (Kassin, Redlich, Alceste, & Luke, 2018; Kassin et al., 2001). Furthermore, research clearly indicates that judges routinely overestimate jurors’ ability to understand and correctly use memory evidence when in fact it is based solely on their “common sense”—such as that memory works like a video camera (e.g., Houston, Hope, Memon, & Read, 2013; Magnussen et al., 2010); for the Scooter Libby effect, see also Kassam, Gilbert, Swencionis, & Wilson, 2009).
The question of whether jurors’ commonsense views of memory in court are adequate also extends to cases in which adults are recollecting events that happened decades earlier in childhood. As elsewhere, it is not a given that judges will necessarily accept scientific expert testimony about memory in their courtroom to counteract the commonsense views held by jurors and others involved in the judicial system. Progress has been made in some U.S. states in which judges in trials involving eyewitness identification must now present jurors with cautions about the reliability of such evidence before their deliberation (State of New Jersey v. Henderson, 2011). In Pennsylvania, Loftus, Francis, and Turgeon (2012) drafted jury instructions that addressed issues concerning a broad spectrum of expert memory testimony. Likewise, in the United Kingdom, judges are now obligated to give juries so-called Turnbull guidelines in the cases that heavily rely on eyewitness identification (Trevelyan, n.d.). Admittedly, these are but a few recent examples, and much more research needs to be conducted to counteract the impact of erroneous lay beliefs about memory in the courtroom.
Furthermore, it is also imperative that such guidelines are not fixed but are provisional and can be updated any time. Guidelines are ideally based on the current corpus of scientific findings, but new findings might warrant amendments. For example, previous research has suggested that the confidence that eyewitnesses place in their identification is only weakly related to their accuracy. In contrast, recent research has demonstrated that under optimal conditions, confidence is strongly predictive of accuracy (Sauerland & Sporer, 2009; Wixted & Wells, 2017). It is important to be cognizant about such new developments.
Memory wars in the scientific literature
One might posit that although the controversial issue of repressed memories is still relevant in clinical and legal contexts, the debate concerning repressed memories is now muted in the scientific literature. There are two indications that this is not the case. First, in a recent bibliometric analysis, Dodier (2019) examined the number of publications and citations regarding repressed and recovered memories from 2001 to 2018. The author found that proponents and opponents of repressed memories have continued to publish articles about repressed and recovered memories throughout the time period. Notably, these articles were cited just as often as articles published during the presumed heyday of the memory wars in the 1990s. In addition, the year 2018 witnessed an increase in publications on this topic. This increase was characterized by a mix of articles in favor or against the concept of repressed memories. Specifically, of the 16 articles in 2018, 5 (31%) were largely or entirely in favor of the existence of repressed memories, whereas 9 (56%) articles expressed skepticism regarding the existence of repressed memories (two articles adopted a neutral position).
Second, the debate over repressed memories and dissociative amnesia has hardly vanished from the scientific literature. For example, Brand, Schielke, and Brams (2017) and Brand, Schielke, Brams, and DiComo (2017) recently tried to provide legal professionals with evidence-based knowledge on trauma-related dissociation and concomitant effects such as dissociative amnesia. Their articles provoked a disagreement between them and memory researchers who argued that their conclusions were not based on evidence and potentially hazardous (Brand et al., 2018; Merckelbach & Patihis, 2018; Patihis et al., 2019). Debates relating to the issue of dissociative amnesia, repressed memories, or both, are clearly alive and well in the scientific literature (see also Staniloiu & Markowitsch, 2014).
Conclusion
The claims of some authors to the contrary, the controversial topic of repressed memories and dissociative amnesia continues to be very much alive in clinical, legal, and academic contexts. Converging lines of evidence suggest that concerns regarding the widespread belief in repressed memories are far from having been resolved following the memory wars of the 1990s. Across many different professionals (e.g., psychotherapists), the percentage who believe in repressed memories remains high, generally above 50%. Furthermore, the idea of repressed memories has merely become popular under a different name—dissociative amnesia—which shares many characteristics with repressed memory and that carries the added cachet of being associated with the DSM–5 (American Psychiatric Association, 2013). In addition, research points to the possibility that some therapeutic techniques exert adverse effects by potentially increasing the likelihood of false memories. Finally, questions of repressed memories continue to be addressed in the courtroom and in the scientific literature. Taken together, these different threads of evidence imply that falsely recovered memories of abuse continue to pose a substantial risk in therapeutic settings, potentially leading to false accusations and associated miscarriages of justice.
A relevant question is how flawed ideas regarding the functioning of memory could be corrected. That unconscious repressed memory is still accepted with little qualification and remains popular among many mental-health professionals can be explained in part by the now well-replicated finding that it is typically difficult to correct erroneous beliefs. Specifically, when people are confronted with any form of misinformation (e.g., fake news), correcting such errors is challenging, a phenomenon referred to as the continued-influence effect (Lewandowsky, Ecker, Seifert, Schwarz, & Cook, 2012; see also Lilienfeld, Marshall, Todd, & Shane, 2014) or belief perseverance (C. A. Anderson, Lepper, & Ross, 1980). However, recent studies suggest that informing people that their firmly held beliefs are incorrect (“prebunking”), and even providing them with the correct alternative information (debunking), can often be effective in correcting these beliefs (e.g., Blank & Launay, 2014; Crozier & Strange, 2019). In addition to applying these provisional but promising methods, it is crucially important to educate individuals, especially legal professionals and clinicians, about the science of memory. This effort is all the more essential given that these professionals are often in close contact with victims, patients, witnesses, and suspects. Such interactions are a prime opportunity for inadvertent memory contamination. Increasing their awareness of potentially harmful beliefs about repressed memories should therefore be a priority in clinical and legal work as well as for psychological scientists at large.