Abstract
Purpose: A heated debate exists on whether traumatic memories can be dissociated or repressed. One way in which researchers have attempted to prove the existence of dissociative amnesia or repressed memory is to examine whether claims of amnesia for traumatic events are associated with specific neural markers.
Methods: Here, we will argue that such neuroscientific examinations do not tell us whether traumatic memories can be unconsciously repressed or dissociated from consciousness, respectively.
Results: We discuss neuroscientific studies on dissociative amnesia and repressed memory and show that there are no reliable biological markers for dissociative amnesia and that the alleged involved brain areas are heterogenous among studies. Furthermore, we will demonstrate that it is unclear whether these studies truly involved patients with dissociative amnesia and that alternative explanations of dissociative amnesia were often not ruled out (e.g. malingering, organic amnesia). Moreover, we will make the case that the discussed patients in the studies do not meet the DSM-5 criteria for dissociative amnesia.
Conclusions: Taken together, neuroscientific research into dissociative amnesia does not present a convincing case for a biological basis of the purported memory loss.
INTRODUCTION
There is widespread interest in how traumatic experiences are remembered. Knowledge on this topic is relevant for the clinical field as an aid in the diagnosis and treatment of those who have developed psychological complaints as a result of experiencing traumatic events (Phelps & Hofmann, 2019). In legal systems, victims, witnesses and defendants oftentimes provide testimony about traumatic events that they allegedly experienced (Otgaar et al., 2022). In therapy, knowing whether traumatic memories are accurate and refer to experienced events is not actually treated as a priority or considered necessary—but accuracy is crucially important in legal contexts. That is, truth seeking is the cornerstone of the legal arena and hence, it is pivotal to know how (accurate) traumatic experiences are recollected.
For many years, there has been a debate about whether traumatic memories can be repressed or dissociated from consciousness and accurately recovered many years later (Loftus, 1994; Otgaar et al., 2019). Some clinicians assert that traumatic memories can be unconsciously repressed or dissociated from consciousness1 and lie dormant for many years, to be exhumed in therapy in their original unaltered form (e.g. van der Kolk & Fisler, 1995). However, other clinicians and memory scientists have argued that therapeutic interventions used to ostensibly unlock memories can be suggestive and may lead to the creation of false autobiographical memories (Loftus & Ketcham, 1991; Piper et al., 2008). Also, empirical memory research has shown that plausible alternative explanations exist for claims of repressed memory loss (e.g. ordinary forgetting including childhood amnesia) and that memories recovered spontaneously are likely to be the result of ordinary memory mechanisms (e.g. ordinary forgetting). This contentious debate regarding whether or not traumatic memories can be repressed or dissociated or not has also been termed the memory wars (Crews, 1995; Loftus, 1994; Lynn et al., 2023).
In past years, some authors have claimed that there is neuroscientific evidence in favour of the idea that traumatic experiences can be unconsciously repressed or dissociated from consciousness. Specifically, some researchers have investigated the neural correlates of claims of dissociative amnesia which is a disorder analogous to repressed memory, but is also used as a diagnostic criterion of posttraumatic stress disorder (PTSD) or dissociative identity disorder (DID; for example Staniloiu & Markowitsch, 2012a). As we will explain, the diagnostic criteria of the disorder dissociative amnesia are strikingly similar to the tenets of the concept of repressed memory in which the core idea is that traumatic memories can be completely abolished from consciousness and retrieved in original form (Otgaar et al., 2021; Pope Jr et al., 2022).
In the current article, we will provide a critical discussion of what such neuroscientific studies can and cannot tell us about whether traumatic memories can be unconsciously repressed or dissociated. Specifically, we provide a critical discussion of neuroscientific studies on dissociative amnesia. We will first provide a general overview of these neuroscientific studies and critically review the observed key findings. That is, we will present a literature search on these neuroscientific studies and first examine which brain regions are allegedly associated with the claimed traumatic memory loss. Second, we will provide several critical comments on whether neuroscientific research on dissociative amnesia and repressed memory actually included participants with dissociative amnesia. Third, we will discuss methodological and conceptual problems and argue that the key claims of neuroscientific research on dissociative amnesia and repressed memory are seemingly in contrast with the tenets of dissociative amnesia. Finally, we will provide recommendations for this relatively young field with a strong focus on advocating open science practices.
THE NEUROSCIENCE OF REPRESSED MEMORY AND DISSOCIATIVE AMNESIA
The kernel of the concepts of repressed memory and dissociative amnesia is that when people experience severe traumatic events such as childhood sexual abuse, defence mechanisms need to be applied to deal with the overwhelming nature of the psychological trauma. Purported underlying mechanisms are, for example: (1) repression whereby automatically and unconsciously traumatic memories are processed or (2) dissociation which is regarded as an ‘unconscious, automatic, defensive coping response to highly aversive events’ (Lynn et al., 2022, p. 22.3; but see also Ross, 2022 for a discussion on the conceptualization of repression and dissociation). For example, instead of the term repressed memory, the term dissociative amnesia is often used to designate traumatic memory loss (Mangiulli et al., 2022; McNally, 2023). When examining the criteria of dissociative amnesia in the DSM-5 (American Psychiatric Association, 2013), they are strikingly similar to the tenets of repressed memory (see McNally, 2023; Otgaar et al., 2019). Both conceptualizations include the idea that memory loss is due to a coping response needed to deal with the trauma, that the memory becomes inaccessible to retrieval and that it can be accurately recalled in its original form at a later point in time.
For several years, studies have examined the neural markers of dissociative amnesia that might provide clues regarding the mechanisms underlying the memory loss for trauma. For example, Kikuchi et al. (2009) had two patients with purported dissociative amnesia and control participants undergo fMRI and concluded that ‘memory repression in dissociative amnesia is associated with an altered pattern of neural activity’ (p. 620). Such a statement strongly implies that dissociative amnesia can be readily identified using brain imaging tools.
WHICH MEMORY SYSTEMS AND BRAIN AREAS ARE INVOLVED?
We conducted a literature search to identify relevant papers examining the different brain areas that scholars have claimed to be involved in cases of dissociative amnesia and repressed memory. The search was conducted on September 22 and October 12 and 26, 2022. We attempted to find all relevant papers published prior to 2022. We inspected the Web of Science database using several search terms (see https://osf.io/zkwhj). Our search identified 207 hits. After removing duplicates, screening (i.e. looking at the title and abstract) and assessing papers for eligibility, 29 papers remained. Four extra papers were identified from Mangiulli et al.'s (2022) critical review on case studies of dissociative amnesia leading to a final set of 33 papers (see Figure 1; see also https://osf.io/wkph9/). Specifically, we only included papers in which researchers used brain imaging tools to examine the neural correlates of repressed memory and dissociative amnesia and review papers in which researchers proposed brain regions involved in dissociative amnesia and repressed memory.
FIGURE 1
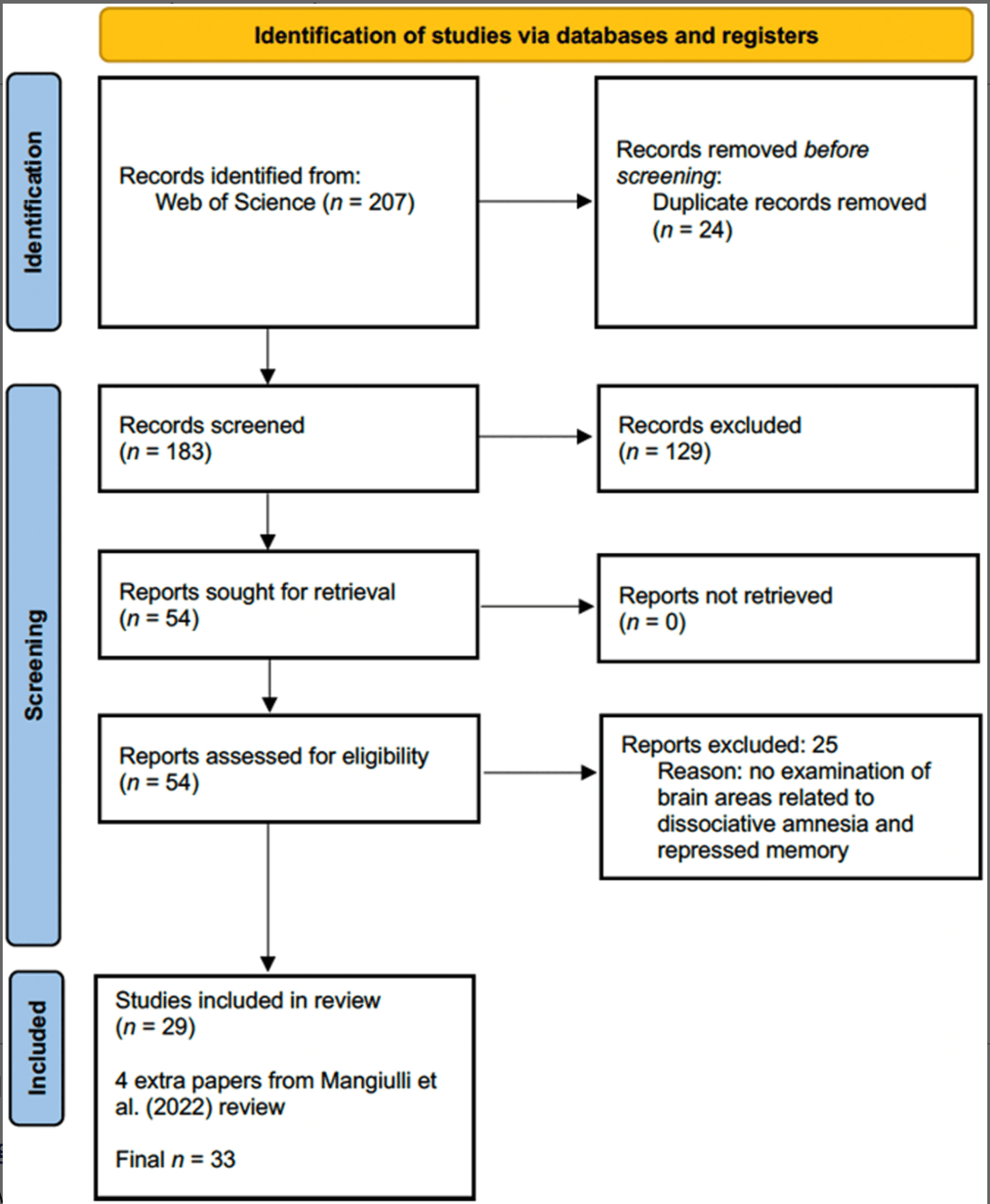
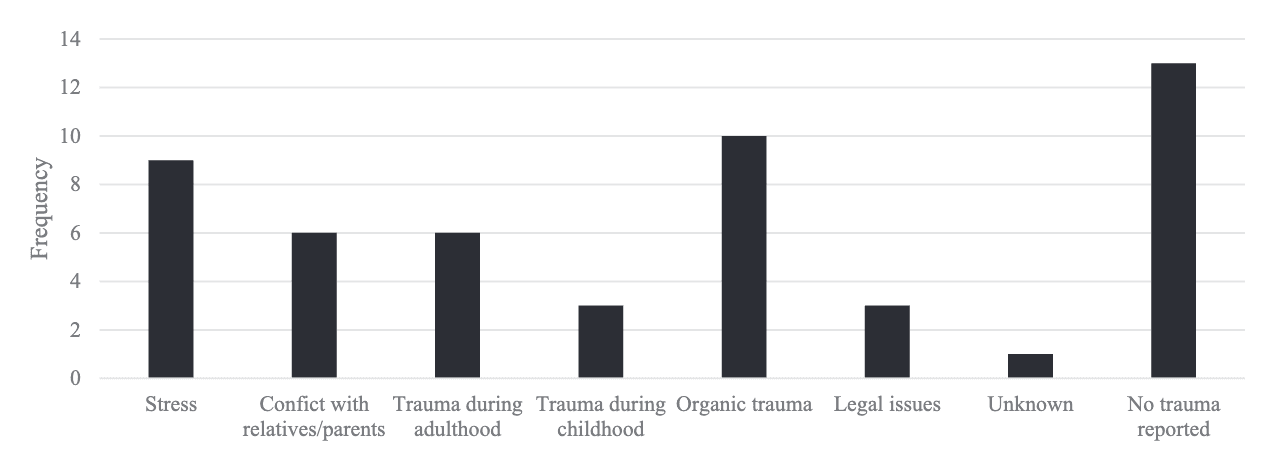
TABLE 1. Overview of papers on the neuroscience of dissociative amnesia and repressed memory.
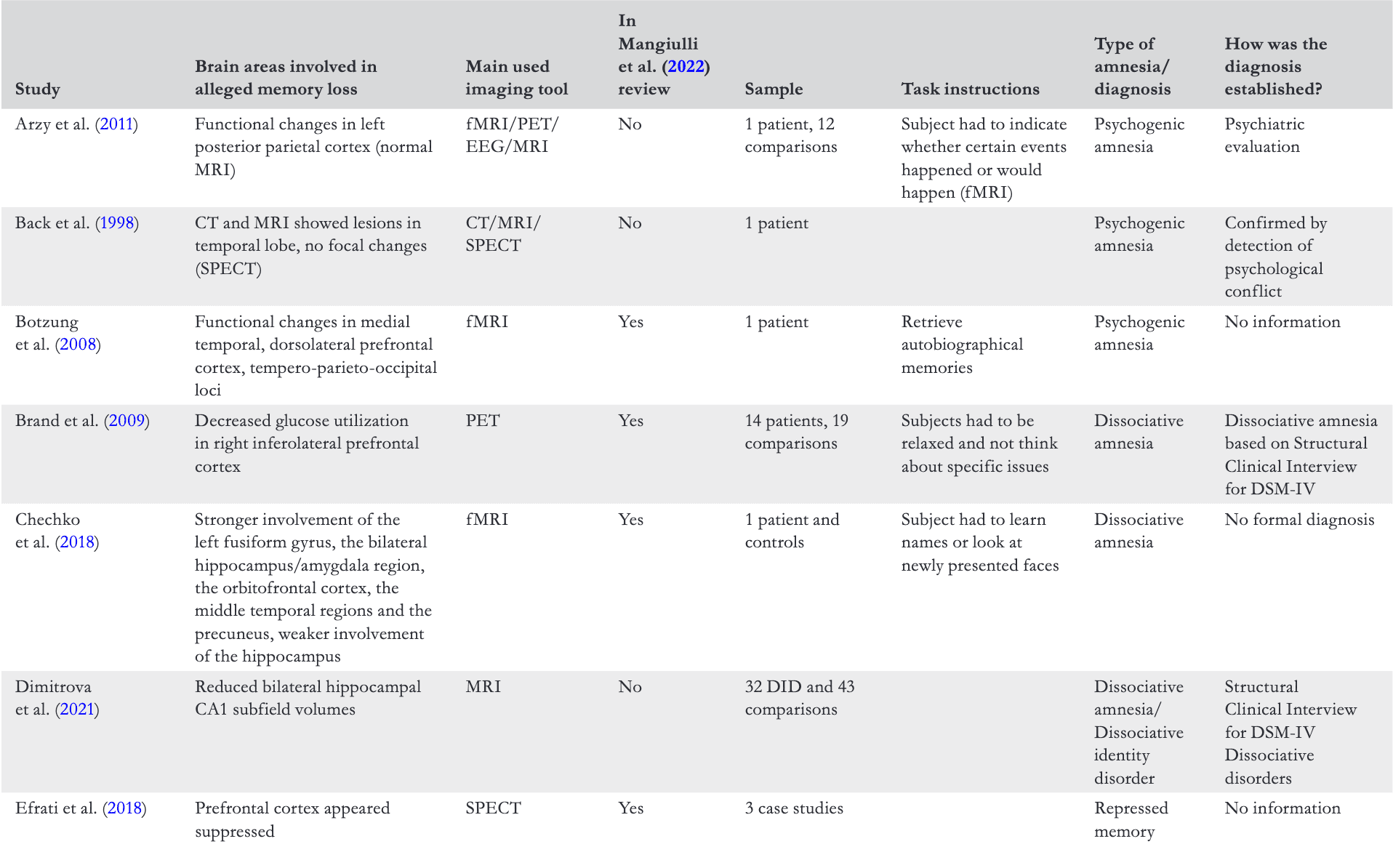
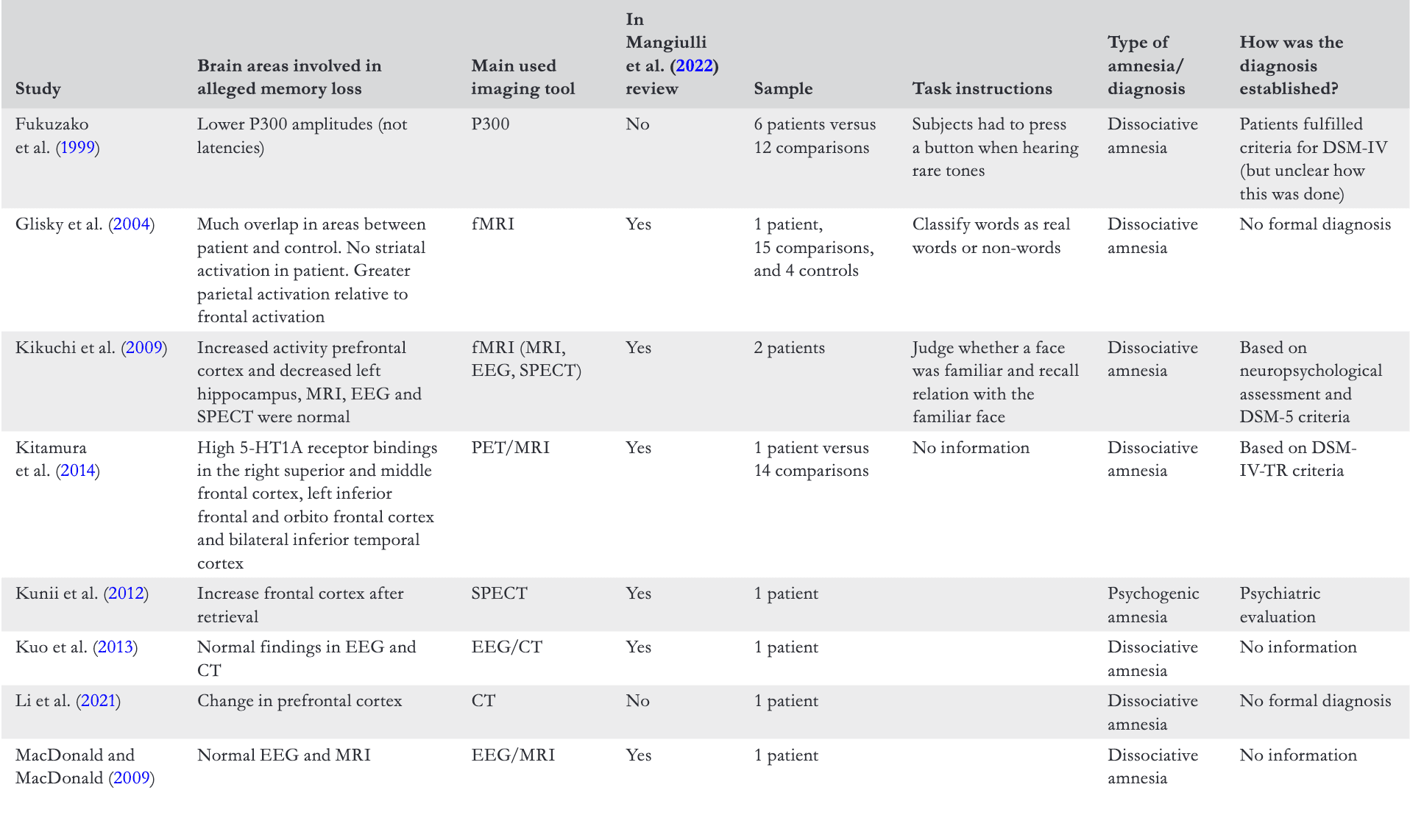
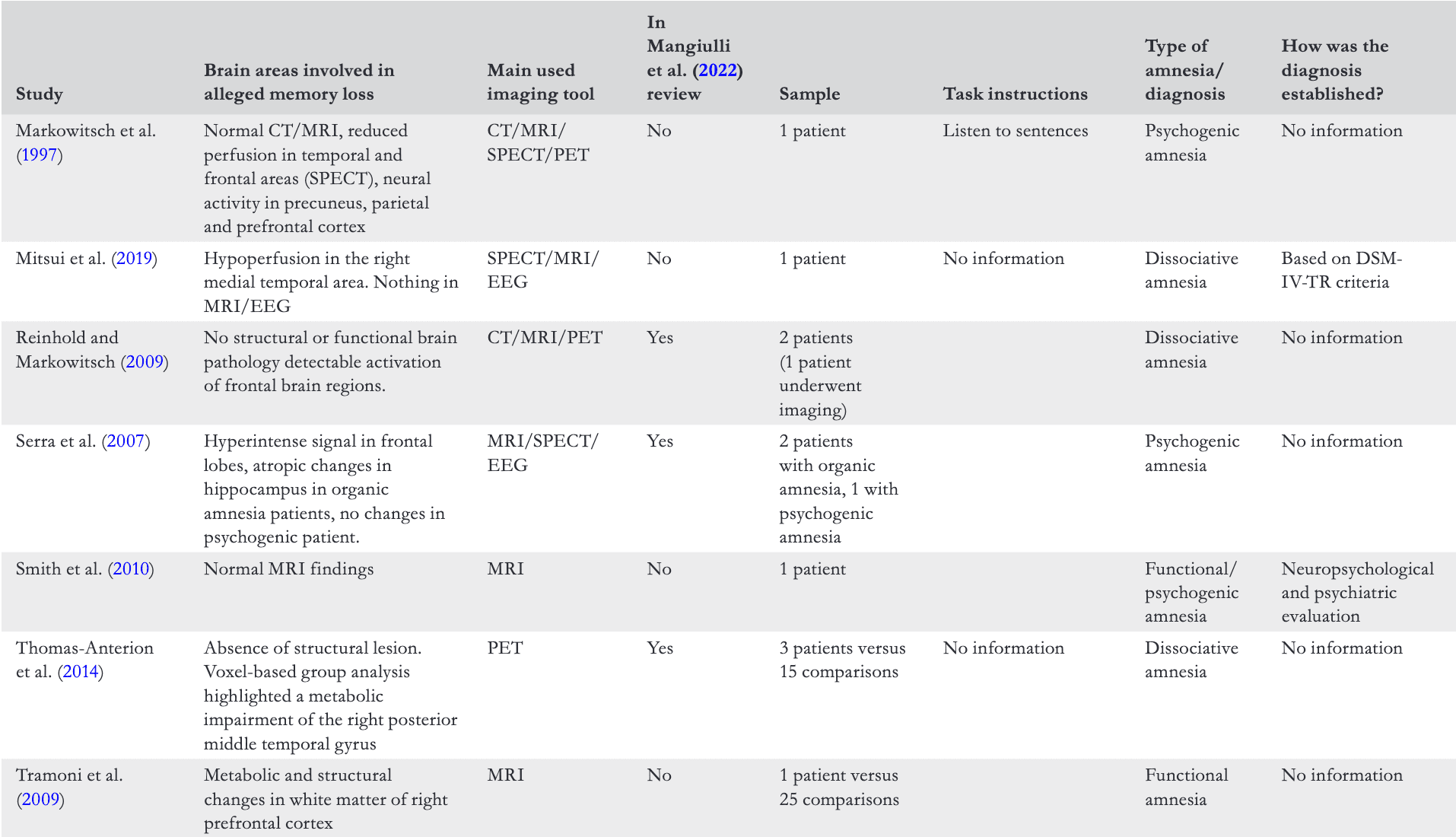
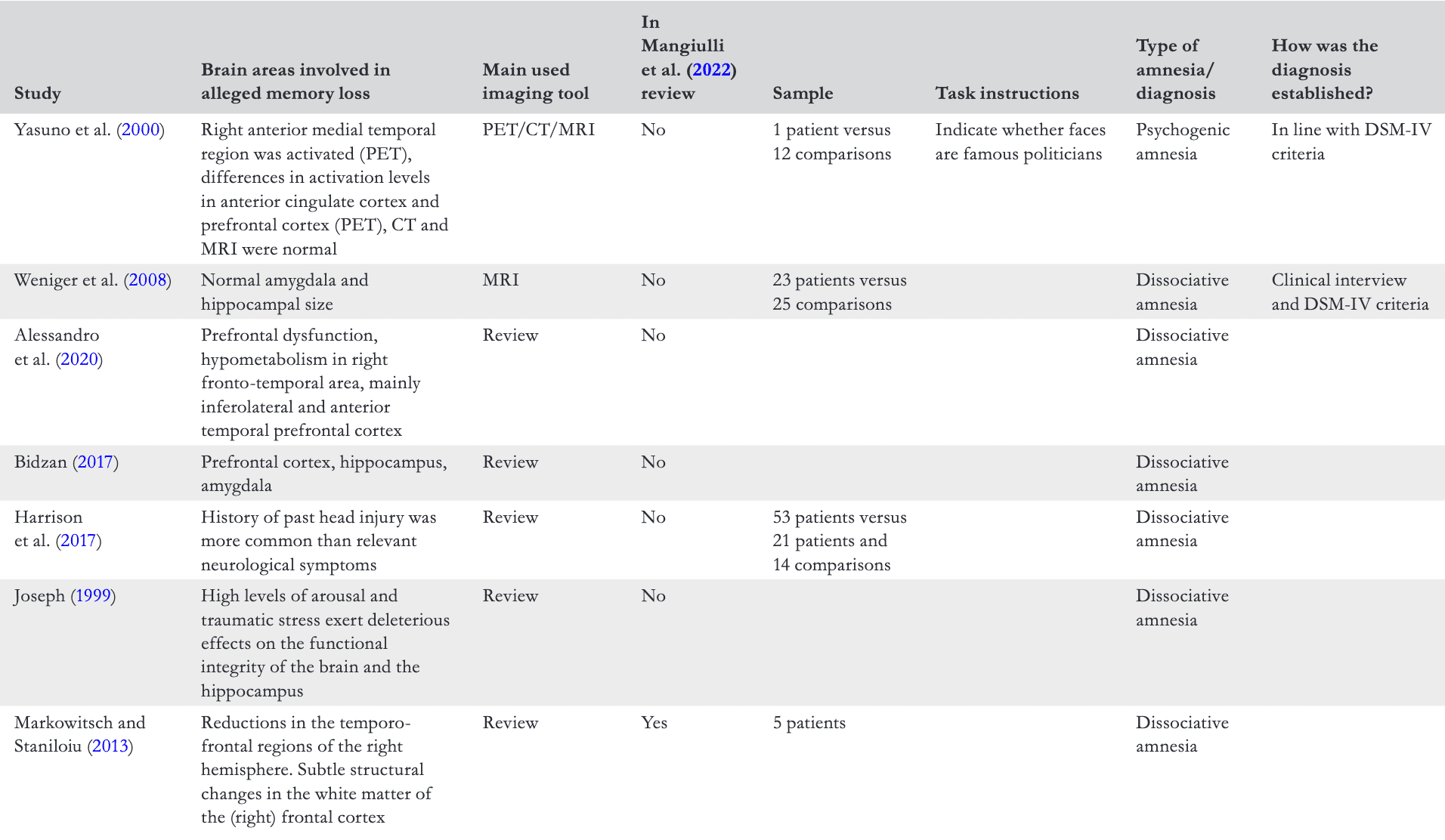
Note: The Efrati et al. (2018) specifically mentioned repressed memory in their study while others specifically stated dissociative amnesia; The instructions category were only added for studies using functional imaging tools and refers to the instructions that the subjects received during imaging. Review papers are added at the end of the Table. All studies including comparison groups used healthy control participants except for the paper by Harrison et al. (2017) and the paper by Serra et al. (2007).Note: The Efrati et al. (2018) specifically mentioned repressed memory in their study while others specifically stated dissociative amnesia; The instructions category were only added for studies using functional imaging tools and refers to the instructions that the subjects received during imaging. Review papers are added at the end of the Table. All studies including comparison groups used healthy control participants except for the paper by Harrison et al. (2017) and the paper by Serra et al. (2007).
A key result from our search was the great variability of brain regions found to be involved in reports of dissociative amnesia. Specifically, across papers, a bit over half of them (n = 19; 58%) noted that the (pre)frontal cortex was associated with the dissociative memory loss. However, which specific area of the prefrontal cortex (e.g. dorsolateral, orbitofrontal) was involved varied as well across studies. There was also much variation in other involved brain areas with papers mentioning areas such as left fusiform gyrus (1 paper; 3%), hippocampus (6 papers; 18%), temporal cortex (14 papers; 42%), parietal cortex (4 papers; 12%) and the precuneus (2 papers; 6%). Many of these brain areas are involved in the function of memory (e.g. Lundstrom et al., 2005), but it is remarkable that no clear and consistent pattern emerged in terms of which brain areas are associated with dissociative amnesia. Of course, this outcome might also be due to the use of different tasks that subjects performed during functional imaging (see Table 1) and the use of structural versus functional methods.
Another result from our search is that in most functional imaging studies, the tasks used or the instructions to participants during imaging were not specified or did not tap into dissociative amnesia for autobiographical events, but rather other memory systems or no memory systems at all. For example, in a study by Brand et al. (2009), participants were only instructed to be relaxed and to not think about specific issues (i.e. resting state). Other studies have included tasks as varied as classifying words as real words versus non-words, listening to rare tones and sentences. Unless in the context of DID, where patients may report deficits in other memory systems, these tasks and instructions are not related to the dissociative amnesia for autobiographical life events as defined in the DSM-5 dissociative amnesia criteria.
However, even within and among the use of these methods, there was large variation. To give some examples, Chechko et al. (2018) used fMRI in a patient with dissociative amnesia. They found that although the patient could not recognize the faces of friends and relatives, there was increased activity in the hippocampus. This finding is in stark contrast to Kikuchi et al. (2009) who also used fMRI and reported reduced activity in the hippocampus. To further complicate matters, Glisky et al. (2004) noted that there were not many differences in brain activations between patients and control participants. These inconsistencies also emerged when structural imaging methods (MRI) were used. For example, whereas MacDonald and MacDonald (2009) and Reinhold and Markowitsch (2009) found no brain structure abnormalities in their patients with dissociative amnesia, Tramoni et al. (2009) found structural changes in the prefrontal cortex.
This latter finding is interesting as it is reminiscent of discussions regarding whether traumatic stress can cause smaller hippocampal volumes in people with PTSD (e.g. Bremner, 1999, 2002). However, Jelicic and Merckelbach (2004) argued that most of these studies contained several methodological flaws (e.g. use of cross-sectional studies), and therefore, any causal relation between traumatic stress and reduced hippocampus could not be established. In fact, longitudinal MRI research on hippocampal volumes in trauma survivors showed that survivors who developed PTSD 6 months after exposure to a traumatic event did not have smaller hippocampal volume than survivors who did not develop PTSD (Bonne et al., 2001). Also, there is research suggesting that smaller hippocampal volumes are not a consequence, but a risk factor for developing PTSD that questions the direction of the causal relation, if any (see for a review Szeszko et al., 2018).
Taken together, the papers examining the brain areas associated with reported dissociative amnesia provide a far from consistent picture concerning its neural underpinnings. Although myriad reasons might be related to this heterogeneity, we now draw attention to what we believe is especially imperative in discussions of dissociative amnesia. That is, did the included papers really involve people with dissociative amnesia?
DID THESE CASES REALLY ASSESS DISSOCIATIVE AMNESIA?
A central issue when examining the neural correlates of dissociative amnesia (and repressed memory) is to know with a degree of certainty that patients who were tested did indeed suffer from dissociative amnesia. Mangiulli et al. (2022) reviewed 128 case studies on apparent dissociative amnesia that were published over the past 20 years (2000–2020). Their analysis showed that although all cases involved reported autobiographical memory loss, none was fully in line with the DSM-5 criteria for dissociative amnesia. For example, in a quarter of cases, no psychological trauma was reported to explain the claimed memory loss. Also, most case studies did not rule out alternative, but plausible explanations for the purported memory loss such as malingering or ordinary forgetting. In addition, in some cases it was not established that the traumatic events were actually inaccessible for a time, or in others whether the traumatic events were encoded initially and therefore available (i.e. recoverable) (see DSM-5 criteria for dissociative amnesia).
In the selected papers in Table 1, 45% (n = 15) were also included in the critical review conducted by Mangiulli et al. (2022). Arguably, the authors of these 15 papers did not truly examine patients with dissociative amnesia that met DSM-5 criteria, but perhaps something different such as malingering, amnesia with an organic cause and so on. Hence, any detected brain region might have nothing to do with dissociative amnesia but could be related to other reasons such as faking memory loss, organic amnesia or the co-occurrence of another psychological disorder.
A case in point on whether dissociative amnesia was truly involved in the tested patients is the study by Dimitrova et al. (2021). In that study, possible neurostructural markers of dissociative amnesia were examined using MRI. One problem with this study is that dissociative amnesia was measured using a subjective index of dissociative amnesia comprised of self-report scores on the dissociative amnesia scale of the Dissociative Experiences Scale (DES; self-report instrument). The DES amnesic subscale does not measure dissociative amnesia as defined in the DSM-5 but instead measures individual's self-reported experience of gaps in memory—and centrally problematic to this is both the subjective nature of the measure and the fact that all people experience gaps in memory through normal memory mechanisms. Hence, what they measured was subjective amnesia and not objective amnesia (i.e. the inability to retrieve information). This distinction is crucial, as the latter can only be measured by including a task that objectively indexes memory functioning rather than the DES. In the context of DID, a whole series of studies has indicated that once objective tasks are included to test subjective amnesia, the results indicate there is actually transfer of information between identities in DID, both on explicit and implicit memory tasks, neutral and trauma-related as well as autobiographical and other self-relevant material (e.g. as an example see Huntjens et al., 2012 and Marsh et al., 2018).
Subjective reports of dissociative amnesia may be explained by specific dissociation-related dysfunctional metamemory beliefs (i.e. metacognitive beliefs about one's own memory functioning). These include positive beliefs about amnesia (e.g. ‘I believe it is better to forget the painful events that I experienced in life’), fear of losing control (e.g. ‘I believe I would lose control of my life if I allowed myself to remember painful things that happened to me’), beliefs about fragmentation (e.g. ‘I believe I can remember distressing events in parts, but not as a whole’) and lack of self-reference (e.g. ‘I believe the bad things that I sometimes remember happening in my life actually didn't happen’). A recent study has indicated that patients with DID score high on a scale developed to index these dysfunctional beliefs and in the general population, these beliefs correlate strongly with scores on the DES (Huntjens et al., 2022).
Other examples similarly illustrate the possible misdiagnosis of dissociative amnesia. Fukuzako et al. (1999) examined the P300 amplitude with participants they labelled as having dissociative amnesia. Although the authors stated that they also examined malingering in their patients, it is unclear what they exactly did and which tests were used to detect feigning behaviour. Also, Fukuzako et al. reported which events might have caused the traumatic loss. Interestingly, at first sight, some of these events do not appear to meet the DSM-5 criterion for traumatic stress (i.e. actual or threatened death, serious injury or sexual violence) and are more related to ‘ordinary’ stress such as experiencing ‘trouble in love affairs’. Also, some of the patients might have tried to forget these distressing events, which is not the same as dissociative amnesia. Finally, Mitsui et al. (2019) describe a man who was diagnosed with dissociative amnesia, but they do not mention the specific psychological traumatic event that purportedly precipitated the alleged memory loss.
To obtain a more precise assessment of whether the cases in Table 1 reflected dissociative amnesia, we adopted the coding scheme as was used in Mangiulli et al. (2022) to code the studies in our table that were not mentioned in Mangiulli et al.'s review. Specifically, the case studies were coded on the following features: (1) was the person given a diagnosis of amnesia, (2) differential diagnosis (did the case descriptions differentiate between dissociative amnesia and other related conditions), (3) malingering, (4) alternative mechanisms and (5) diagnostic features (for a more detailed explanation, see https://osf.io/8hp2t; to view the coding, see https://osf.io/n87qa and https://osf.io/srpuk). The first and fourth author coded the features with interrater reliability agreements (Krippendorff's alpha) ranging from .70 to 1 (see https://osf.io/kch8n).
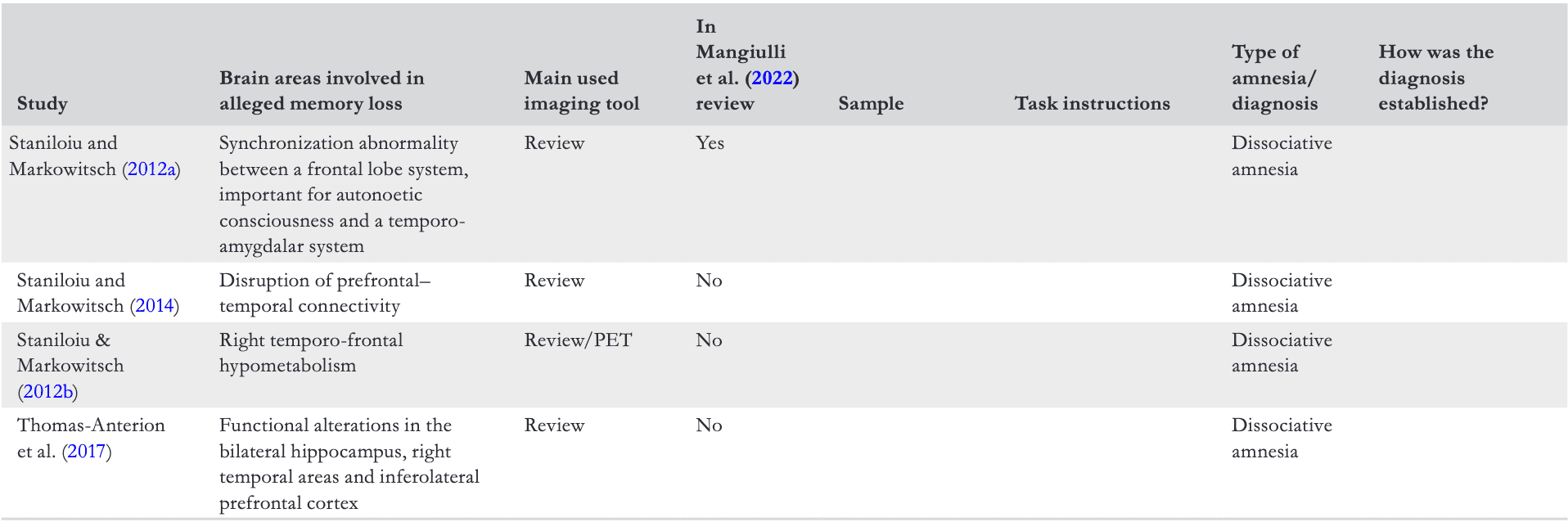
Following this coding, we examined all case studies (n = 51); including the ones included in Mangiulli et al. (2022) (see Table 1) and found the following. First, although in 38 cases (75%; for similar results see Taïb et al., 2023), the authors mentioned the presence of trauma, 10 cases (26%) were related to organic trauma. This is noteworthy as to qualify for a diagnosis of dissociative amnesia; memory non-reporting must not be the result of an organic cause. Second, we examined whether the case studies met the diagnostic features of the DSM-5. Only two cases (3.9%) met all diagnostic features of dissociative amnesia (i.e. mentioning of trauma, not due to substances, mentioning of type of dissociative amnesia, mentioning of duration of amnesic period and mentioning of impairment in functioning). However, even these two case studies were not convincing examples of dissociative amnesia because in one a car accident was mentioned as trauma indicating that an organic cause cannot be ruled out. In the other case, losing a job was regarded as the traumatic cause and it was unclear whether malingering could be fully ruled out. Equally interesting, in 13 cases (26%), no mention was even made of a possible traumatic cause (see Figure 2; https://osf.io/wkph9/).
FIGURE 2
Frequencies of type of alleged traumatic cause.
Collectively, case studies of dissociative amnesia are frequently hampered by the fact that it is not certain whether the diagnostic criteria for dissociative amnesia are met. Therefore, it is imperative that alternative explanations for amnesia be ruled out before the label of dissociative amnesia is warranted (Mangiulli et al., 2022).
ALTERNATIVE EXPLANATIONS
We next consider the important issue to discuss of whether neuroscientific studies on dissociative amnesia can be explained by alternative, more plausible explanations for patient reports of memory loss. For example, Mangiulli et al. (2022) found that organic brain damage, instead of psychological coping mechanisms for trauma, could explain many of the cases of reported autobiographical memory loss. In the reviewed studies (Table 1), Harrison et al. (2017) also shared this view. They reviewed 53 patients with purported dissociative amnesia and the authors found that ‘a history of past head injury was actually more common’ (p. 2498). Thus, it might well be the case that their autobiographical memory loss did not have a psychological origin but was caused by, for example, head injury.
Another alternative explanation for the neural correlates found in some dissociative amnesia cases is that the detected regions are actually related to other cognitive mechanisms. We already mentioned the possibility of metamemory beliefs explaining reports of dissociative amnesia (Huntjens et al., 2022). As another example, functional MRI research on motivated forgetting has shown that similar brain areas are recruited during such forgetting (i.e. prefrontal cortex) as the areas observed in the reviewed papers (Anderson & Hanslmayr, 2014). Thus, 21 (64%) of the identified papers mentioned involvements of the prefrontal cortex and some (or all) of them might have nothing to do with dissociative amnesia but instead be linked to motivated forgetting. Put another way, these areas may involve the conscious suppression of events people do not want to recall.
FMRI studies have shown that the prefrontal cortex is involved in memory suppression (Anderson & Hanslmayr, 2014). Although there is debate on the robustness of the memory suppression effect (e.g. Bulevich et al., 2006; Wessel et al., 2020) and the motivated forgetting effect (Patihis & Place, 2018), there is a possibility that the observed brain areas in the reviewed studies are not related to dissociative amnesia but instead to active memory suppression or cognitive control more generally. It is important to stress here that memory suppression is different from dissociative amnesia as the latter purportedly involve unconscious forms of memory loss whereas suppression is an intentional act to forget memories. Also, research shows that people who have experienced trauma frequently try to forget the trauma (McNally, 2005) and therefore, some neuroscientific studies on dissociative amnesia might actually involve cases of memory suppression or cognitive control.
The claimed involvement of the prefrontal cortex in dissociative amnesia might also be indicative of deception in some cases (e.g. malingering). Specifically, investigations into brain areas involved in deception have revealed the prefrontal cortex to play a chief role (e.g. Abe, 2011). This perspective fits well with concerns that some cases of autobiographical memory loss might be due to deceitful attempts to claim amnesia (Jelicic, 2018; Mangiulli et al., 2022). To recap, although the reviewed papers sometimes reported that the prefrontal cortex might be related to dissociative amnesia, we argue that memory suppression might equally apply as an alternative explanation.
To examine whether the authors of the included studies considered alternative explanations, we coded all case studies in terms of whether or not the authors ruled out the possibility that the claimed memory loss was due to normal forgetting, encoding failure or malingering. Importantly, the alternative explanations of normal forgetting and encoding failure can only be coded for case studies in which the amnesia was localized (memory loss for a specific period) or selective (remembrance of some aspects of an event but not all; American Psychiatric Association, 2013) (see Mangiulli et al., 2022). For these case studies, none mentioned that the memory loss might be attributable to normal forgetting or encoding failures. Regarding malingering, only 37% (n = 19) of the case studies mentioned this as a possible alternative explanation. However, of these 19 cases, most did not elaborate on potential malingering and, for example, did not refer to the context in which malingering might be a plausible explanation (e.g. criminal context, n = 17; 90%) or did not state how malingering was tested (n = 13; 68%). In short, only limited information was present in the case studies concerning alternative explanations of the claimed memory loss.
CONCEPTUAL AND METHODOLOGICAL PROBLEMS
In this final section, we concentrate on several conceptual and methodological problems that underlie neuroscientific investigations concerning dissociative amnesia and repressed memory. First, the aim to find a structural biomarker of dissociative amnesia is incompatible with the nature of the phenomenon (e.g. Dimitrova et al., 2021; Li et al., 2021; see Huntjens et al., 2022 for a critical commentary on this issue). The DSM-5 definition is that dissociative amnesia is always potentially reversible due to successful storage of the memory. It is for this reason that some neuroscientific investigations have attempted to exclude structural brain damage when diagnosing dissociative amnesia (e.g. Brand et al., 2009).
Second, neuroscientific studies on dissociative amnesia and repressed memory suffer from other methodological limitations such as small sample size and lack of comparison groups. For example, a minority of studies included comparison groups (n = 11; 33%). Furthermore, as can be seen in Table 1, it is not uncommon that only a few patients were tested and that conclusions were based on small sample sizes. Nonetheless, the small samples are understandable given the alleged low prevalence of the disorder and the difficulty in recruiting these patients who suffer great impairment in daily functioning. However, recent work has suggested that published studies on biomarkers for psychological phenomena might yield erroneous conclusions as many more participants are needed in such studies to obtain reliable results (Marek et al., 2022). This possibility is echoed by recent work conducted by Mertens et al. (2022) on the neural correlates of posttraumatic dissociation. The authors stressed that small sample sizes in this area limited the interpretation of neuroscientific research into dissociation. Their research contained the largest sample size using fMRI to identify neural regions of dissociation and they did not observe any reliable neural marker of dissociation. Moreover, most studies did not include corrections for multiple testing or make use of alternatives like robust testing, further compounding these problems (Huntjens et al., 2022).
Additionally, the extant research (1) usually did not entail structural clinical interviews in the diagnostic procedure, (2) did not consistently examine the role of comorbid psychopathology as a determinant of outcomes secured or as a source of variability across studies; (3) did not consistently include control groups of individuals matched for general psychopathology, distress, arousal and/or negative affect who do not report dissociative amnesia (Lynn et al., 2019, 2022); and (4) was not based on longitudinal studies that ascertain whether patterns of brain structure, activation or anomalies implicated in dissociative amnesia are present prior to the onset of amnesia or traumatic events. Moreover, what a biomarker is versus a correlate of dissociative amnesia is rarely defined and specified, and as stated, the study designs sometimes lacked (clinical) comparison groups (e.g. PTSD present/dissociative amnesia absent group) necessary to rule out confounds that may have accounted for the detected neurobiological patterns.
Finally, even if these conceptual and methodological limitations were remedied, the aforementioned investigations speak to relative differences in the magnitude of brain structures or activity in people with and without dissociative amnesia, but they do not suggest empirically based cut-off specifications needed to verify of dissociative amnesia, thereby showing limited utility in legal and clinical arenas. The correlations researchers report are generally so weak that they cannot be used for diagnostic purposes (see Huntjens et al., 2022)—in essence they are not biomarkers to the same extent that medicine has reliable biomarkers for diseases (e.g. blood tests for diabetes). To summarize, conceptual and methodological issues strongly limit the interpretation of neuroscientific investigations of dissociative amnesia and repressed memory.
CONCLUSIONS AND RECOMMENDATIONS
Debate continues regarding whether traumatic memories can be unconsciously repressed (Brewin et al., 2019; Otgaar et al., 2019). To investigate the potential mechanisms underpinning dissociative amnesia and repressed memory, researchers have examined the neural correlates of dissociative amnesia and repressed memory. We provided a critical discussion of these neurobiological studies on dissociative amnesia and repressed memory. Our main conclusion is that these studies fall short on many different levels (e.g. conceptual and methodological). Therefore, we argue that at present, these neuroscientific studies tell us little about whether traumatic memories can be unconsciously blocked. Importantly, none of these proposed biomarkers are sufficiently reliable for diagnosis in clinics or legal arenas. We will briefly summarize the main problems and we will then end with several recommendations for future research.
First, we have shown that neuroscientific studies have revealed a large number of brain regions potentially involved in dissociative amnesia and repressed memory. This heterogeneity makes it difficult to pinpoint whether any specific regions are involved in the purported traumatic memory loss. Second, it is questionable whether the reviewed case studies really are genuine dissociative amnesia cases—frequently they did not match the DSM-5 criteria. Third, alternative explanations involving ordinary mechanisms can oftentimes better explain traumatic memory loss, compared to the extraordinary mechanisms proposed by the dissociative amnesia concept. This criticism is crucial because explanations such as malingering, metamemory beliefs and/or cognitive control might be candidates for the observed brains regions claimed to be involved in dissociative amnesia. Finally, it can be said that many of the neurobiological studies are plagued by methodological flaws such as small sample sizes. All in all, the research on the purported neurological markers that underpin dissociative amnesia and repressed memory is poorly developed.
To improve the status of neuroscientific research in this area, we offer several recommendations. To begin with, considering the uncertain cause of the alleged memory loss, one might wonder why the term ‘dissociative’ is needed to describe this form of amnesia. Mangiulli et al. (2022) proposed to use the term ‘amnesia of uncertain etiology’ to describe extreme forgetting with no organic cause. We concur with this suggestion, and we have seen that researchers are already slowly using this terminology when describing unique case studies concerning unclear autobiographical memory loss (Basagni et al., 2022). Furthermore, using such a more neutral term would also benefit interpretating the possible causes of the traumatic loss. That is, at present, discussions of dissociative amnesia often gravitate to whether it has an organic, feigned or dissociative aetiology. According to Kopelman (2000), such dichotomies might be too simplistic as case studies on extreme forgetting might be due to an amalgam of organic, faked and other reasons (see also Mangiulli et al., 2022). Second, because we have noticed that neuroscientific studies on dissociative amnesia and repressed memory are plagued by small sample sizes, we believe it is imperative that investment be made in team science in this area (Forscher et al., 2022). That is, since cases of alleged traumatic memory loss are exceptional, working together with other teams worldwide would increase the amount of cases in one particular study thereby increasing statistical power and obtaining more reliable results.
Finally and relatedly, the field of dissociative amnesia (and repressed memory) would benefit from more transparency and adherence to open science practices. Future neuroscientific research on dissociative amnesia should include preregistration of research protocols that stipulate in advance (a-priori) hypotheses, sample size, details of the methodology, planned analyses and cut-offs for ascertaining a biological marker. Additionally, post-research implementation should make data available for other interested researchers to inspect, re-analyse and verify. Doing so is important because, as we have seen, in research in this area, many of these essential steps are not taken and multiple analyses are often conducted on the same data set, which might inflate false positive results (see Huntjens et al., 2022 for a detailed discussion). Preregistration might increase research transparency regarding which analyses were planned and which were done post-hoc in an exploratory fashion.
To conclude, we critically discussed neuroscientific research on dissociative amnesia and repressed memory and argued that this research must be interpreted with great caution and numerous caveats. Considering the fact that this area has been the subject of a controversial debate regarding whether traumatic memories can be blocked and accurately surface after many years, it is vital that neuroscientific research in this field is sound. At this time, there are no consistent or reliable biomarkers of dissociative amnesia. Accordingly, biomarkers cannot be used in diagnosis, and even the existence of the concept as a disease category still remains in doubt. Therefore, we encourage researchers to collaborate in order to critically examine the factors that underlie claims of extreme forgetting.