Abstract
Objective: The goal of this study was to examine the impact of substance use disorder on the risk of hospitalization, complications, and mortality among adult patients diagnosed as having COVID-19.
Methods: The authors conducted a propensity score (PS)–matched double-cohort study (N=5,562 in each cohort) with data from the TriNetX Research Network database to identify 54,529 adult patients (≥18 years) diagnosed as having COVID-19 between February 20 and June 30, 2020.
Results: Primary analysis (PS matched on demographic characteristics and presence of diabetes and obesity) showed that substance use disorder was associated with an increased risk of hospitalization (odds ratio [OR]=1.84, 95% confidence interval [CI]=1.69–2.01), ventilator use (OR=1.45, 95% CI=1.22–1.72), and mortality (OR=1.30, 95% CI=1.08–1.56).
Conclusions: The findings suggest that COVID-19 patients with substance use disorders are at increased risk for adverse outcomes. The attenuation of ORs in the model that matched for chronic respiratory and cardiovascular diseases associated with substance abuse suggests that the observed risks may be partially mediated by these conditions.
HIGHLIGHTS
Persons with substance use disorders, especially those using drugs that impair the cardiovascular and respiratory systems, may be particularly vulnerable to the adverse respiratory effects of COVID-19.
This double-cohort study of 11,124 adults diagnosed as having COVID-19 found that—after propensity score matching on demographic characteristics and presence of diabetes and obesity—substance use disorders were associated with increased hospitalization, ventilator use, and mortality.
The reduction of risks, particularly mortality—after additional matching on hypertension, chronic obstructive pulmonary disease, ischemic heart disease, and cerebrovascular diseases—suggests that observed risks may be mediated, at least in part, by drug-related respiratory and cardiovascular diseases.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) continues to rapidly spread worldwide. As health care systems across the globe battle this pandemic, identifying patients at high risk of contracting COVID-19 and associated complications has become critically important. Persons with a substance use disorder are likely to be at increased risk of contracting SARS-CoV-2 because of their higher rates of homelessness, having overcrowded living conditions or being incarcerated, and having poor access to health care (1). In addition, given the virus’s impact on the respiratory, cardiovascular, and immune systems—which can be impaired by opioids, tobacco, and abuse of other substances—persons with substance use disorders are at increased risk of COVID-19 complications, including acute respiratory distress syndrome (ARDS), renal failure, and death (1, 2).
Persons with substance use disorders, especially those using alcohol and drugs such as opioids, benzodiazepines, and methamphetamines, which damage the lungs and impair the respiratory system, may be particularly vulnerable to the adverse respiratory effects of COVID-19 (1, 2). Likewise, substance use disorders have long been linked with immunosuppression. There is ample evidence that opioids, alcohol, methamphetamines, smoking, and vaping all have strong immunosuppressive effects, resulting in greater susceptibility to infection, more severe and longer lasting illnesses, and lower levels of protective antibodies in the blood (3, 4). In addition, some substance use disorders, such as tobacco (smoking), cocaine, and alcohol use disorders, are associated with adverse cardiovascular effects, including hypertension, ischemia, venous thromboembolism, and brain hemorrhage (5, 6).
Given the range of pathways through which substance use disorders can adversely affect COVID-19 progression, understanding the impact of substance use disorders on such patients holds relevance to clinicians and public health planners as they seek clinical and policy approaches to this epidemic. The primary goal of this study was to examine the impact of substance use disorders on the risk of hospitalization, complications, and mortality among adult patients diagnosed as having COVID-19.
Methods
Data for this study were obtained from the TriNetX Research Network platform, a global federated network of electronic medical record (EMR) data from 35 health care organizations representing hospitals, primary care clinics, and specialty treatment providers. The platform was designed to facilitate research related to COVID-19. Health care organizations contributing EMR data to the TriNetX platform are typically large academic health centers and their affiliates. TriNetX provides access to continuously updated, deidentified aggregate EMR data, including demographic characteristics, diagnoses, procedures, medications, laboratory values, and genomics. At the time of this study, the network included data from approximately 54 million patients from 35 health systems across the United States. The TriNetX platform is described in detail elsewhere (7). The analyses of these data were conducted from June 17 through July 31, 2020. This study was reviewed and approved by the University of Texas Medical Branch Institutional Review Board.
We queried the TriNetx Research Network to select the adult patients (age ≥18) diagnosed as having a COVID-19 infection between February 20 and June 30, 2020. Patients were identified as COVID-19 positive if they had a billable code for COVID-19 (ICD-10 codes: B34.2, B97.29, J12.81, U07.1, U07.2) or a positive SARS-CoV-2 laboratory test result (Logical Observation Identifiers Names and Codes [LOINC]: 94500–6, 94315–9, 94309–2, 94533–7, 94534–5, 94559–2). Patients were excluded if they did not have at least one health care visit in the 12 months before COVID-19 diagnosis. We excluded patients with diagnosis codes indicating other specified viral infection (ICD-9: 079.89) or suspected exposure to other biologic agents (ICD-10: Z03.818) during the same time frame.
A diagnosis of substance use disorder in the 12 months prior to COVID-19 diagnosis was determined by using algorithms on the basis of ICD-10–Clinical Modification (CM) codes, defined in the Centers for Medicare & Medicaid Services chronic conditions disease warehouse (8). We examined demographic characteristics (age, sex, race, ethnicity) and the following comorbid conditions that have been linked to adverse outcomes in COVID-19 patients: diabetes (ICD-10-CM: E08–E13), hypertension (I10), chronic obstructive pulmonary disease (COPD) (J44), ischemic heart disease (I20–I25), obesity (E65–E68), and cerebrovascular disease (I60–I69).
Mortality and hospitalization were assessed directly from the EMR data. Mechanical ventilation was defined by using the following CPT codes: 39.65, 31500, 5A1935Z, 5A1945Z, 5A1955Z, 1015098, 0BH17EZ, 0BH13EZ, 0BH18EZ, and 1022227. All three outcomes were assessed at a follow-up time of 21 days from the date of COVID-19 diagnosis.
Descriptive statistics were presented as frequencies with percentages for categorical variables and as mean±SDs for continuous measures. Baseline characteristics were compared by using Pearson chi-square tests for categorical variables and independent-samples t tests for continuous variables. To account for differences in baseline characteristics between the groups, two propensity score (PS) matching models were developed by using logistic regression to derive well-matched groups for comparative outcomes analysis. Within the TriNetX cohort of COVID-19 patients (N=54,589), we identified two matched cohorts: the first cohort matched on demographic characteristics, obesity, and diabetes (N=5,562) and the second cohort matched on demographic characteristics, diabetes, obesity, hypertension, COPD, ischemic heart disease, and cerebrovascular disease (N=5,450). Given that many commonly abused substances increase the risk for chronic respiratory and cardiovascular diseases (1, 2, 5, 6), we determined that four of the comorbid conditions under study (hypertension, COPD, ischemic heart disease, and cerebrovascular disease) were possible mechanistic pathways between substance use disorder and adverse COVID-19 outcomes. We therefore excluded these four conditions from the primary PS-matched models. All statistical analyses were conducted with the TriNetX platform, which utilizes a combination of JAVA, R, and Python programming languages.
Results
Table 1 presents demographic and clinical characteristics in the PS-matched substance use disorder and non–substance use disorder COVID-19 cohorts. A total of 54,529 patients who were positive for COVID-19 were identified in the U.S. TriNetx database. Of those, 5,562 (10.2%) had a substance use disorder (see supplement). Males; Blacks; Hispanics; and persons with diabetes, hypertension, COPD, ischemic heart disease, obesity, or cerebrovascular disease were overrepresented in the subgroup of individuals with substance use disorder. Both PS-matched cohorts achieved strong balance on all matched variables.
TABLE 1. Characteristics and outcomes in propensity score–matched COVID-19 cohorts of individuals with and without a substance use disorder
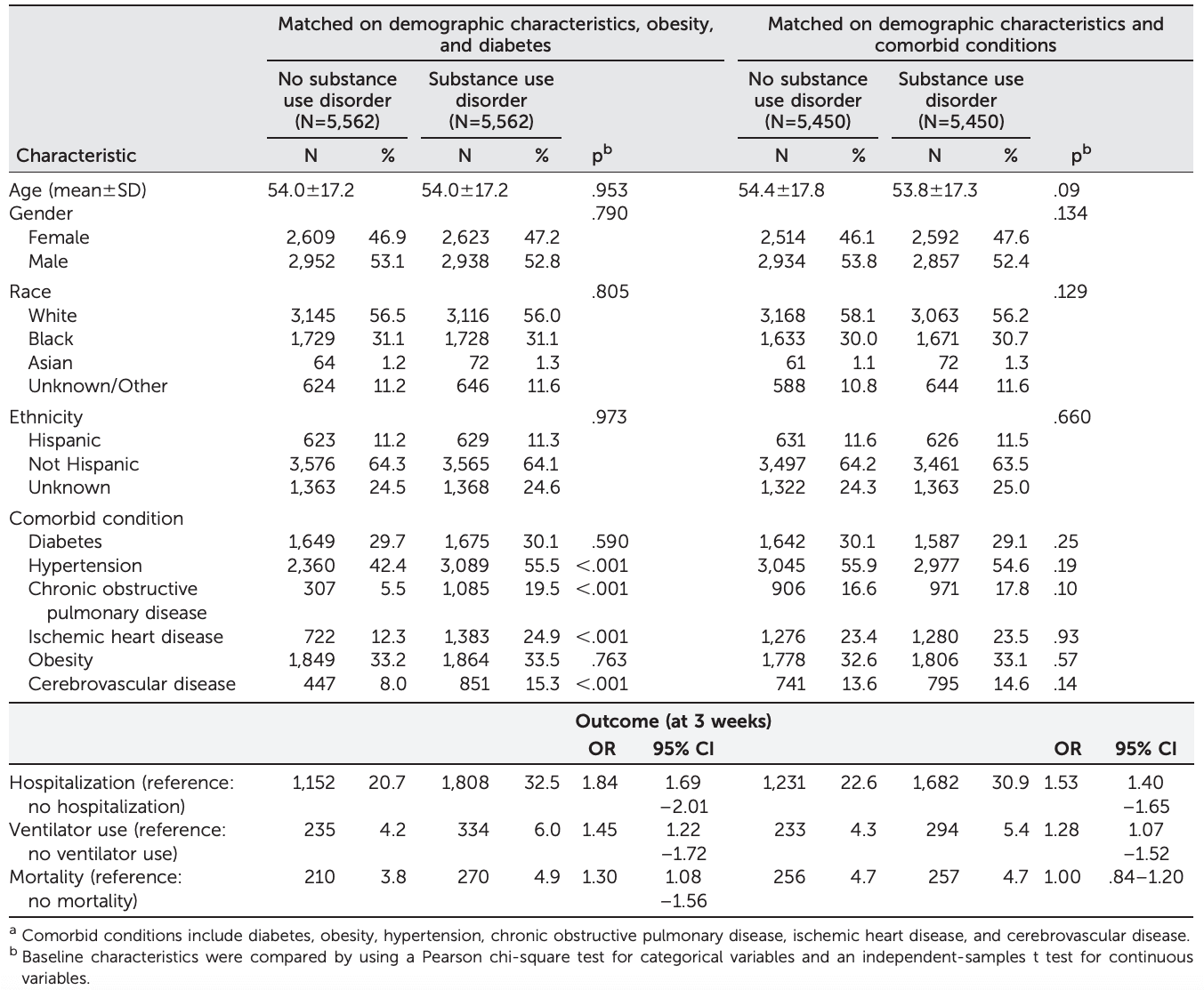
Three outcomes—hospitalization, ventilator use, and mortality—within 21 days of COVID-19 diagnosis were examined in the substance use disorder versus non–substance use disorder cohorts. In the unmatched analysis (see supplement), substance use disorder was associated with an increased risk of hospitalization (32.5% versus 17.4%, odds ratio [OR]=2.29, 95% confidence interval [CI]=2.16–2.44), ventilator use (6.0% versus 3.1%, OR=2.02, 95% CI=1.79–2.28) and mortality (4.9% versus 2.8%, OR=1.81, 95% CI=1.58–2.07). In the PS-matched cohort that was matched on demographic characteristics, diabetes, and obesity, substance use disorder was associated with an increased risk of hospitalization (32.5% versus 20.7%, OR=1.84, 95% CI=1.69–2.01), ventilator use (6.0% versus 4.2%, OR=1.45, 95% CI=1.22–1.72), and mortality (4.9% versus 3.8%, OR=1.30, 95% CI=1.08–1.56). The final PS-matched cohort included four additional comorbid conditions—hypertension, COPD, ischemic heart disease, and cerebrovascular disease—that were potentially mechanistic pathways between substance use disorder and adverse outcomes. This model showed that substance use disorder was still associated with an increased risk of hospitalization (30.9% versus 22.6%, OR=1.53, 95% CI=1.40–1.65) and ventilator use (5. 4% versus 4.3%, OR=1.28, 95% CI=1.07–1.52) but not with mortality (4.7% versus 4.7%, OR=1.00, 95% CI=0.84–1.20).
Discussion
In this double-cohort study of 11,124 adults diagnosed as having COVID-19, we found that after PS matching on demographic characteristics, diabetes, and obesity, having a substance use disorder was associated with increased hospitalization, ventilator use, and mortality. When hypertension, COPD, ischemic heart disease, and cerebrovascular disease—possible mediators between substance use disorder and COVID-19 adverse outcomes—were added to the matching algorithm, the increased risks for hospitalization and ventilator use persisted, but the mortality risk was attenuated. Overall, our findings are consistent with a broad literature that has reported adverse effects of substance use disorder on the respiratory, cardiovascular, and immune systems (1–3, 9). The attenuation of risks, particularly mortality, in the final model—after matching on respiratory and cardiovascular diseases—suggests that the increased risks experienced by patients with a substance use disorder may be driven, at least in part, by drug-related respiratory and cardiovascular disease (1–3, 9–13).
Hypertension, COPD, ischemic heart disease, and cerebrovascular disease all represent important mechanistic pathways between substance use disorder and COVID-19 adverse outcomes. For example, smoking and vaping tobacco or cannabis damage lung tissue, cause inflammation, diminish lungs’ capacity to respond to infection, and increase angiotensin-converting enzyme 2 receptor density, all of which can exacerbate respiratory disease caused by SARS-CoV-2 (1, 2, 11). Likewise, prolonged alcohol use is linked to impaired mucociliary clearance and lung function, and methamphetamine use is linked to noncardiac pulmonary edema, ARDS, alveolar hemorrhage, pneumonia, and pneumoconiosis (10, 11). In addition, cocaine, methamphetamines, alcohol, tobacco, and opioids are reported to have adverse effects on the cardiovascular system, including hypertension, ischemia, venous thromboembolism, and brain hemorrhage (5, 12, 14).
Substance use disorders can also increase the risk of adverse COVID-19 outcomes through immunosuppression (3). For example, opioids exert various suppressive effects on both the innate and adaptive immune systems, especially among those who have long used substances (≥90 days in a year). Largely by binding to the mu receptor and modulating various downstream cellular signaling pathways, opioids impair the recruitment and function of virtually all immune cells, such as macrophages, NK cells, granulocytes, and B and T lymphocytes (3). Methamphetamines are also reported to increase immune dysregulation, particularly in the lungs (15). Similarly, chronic alcohol use interferes with all aspects of the adaptive immune response, including both cell-mediated and immune responses, which increase the susceptibility of persons with alcohol use disorder to viral and bacterial infections.
The results of our study may have been influenced by several limitations. First, the diseases and medical conditions examined in this study were based on ICD-10-CM codes. Such codes are not always accurate or complete. Second, the TriNetX platform does not represent the general U.S. population, but rather only people who receive clinical care within the 35 health care organizations in the network. Third, reliance on EHR data precluded assessment of a number of potential confounding factors, such as region, and markers of adverse socioeconomic disadvantages, such as neighborhood density, occupational exposure hazards, access to care, access to timely COVID-19 testing, and quality of care for preexisting chronic conditions not related to COVID-19. Despite these limitations, this study had a number of strengths, including a large sample from 35 health systems covering all major regions of the United States and a rigorous analysis based on PS matching.
Conclusions
Our findings suggest that among patients with COVID-19, those with a comorbid substance use disorder have an increased risk of adverse outcomes. The attenuation of the risk for mortality in the final model may reflect an important mediating role of drug-related respiratory and cardiovascular disease. More longitudinal research is needed to further understand the relationship between short- and long-term use of various commonly abused substances, the interactions of the substances with medications related to COVID-19, and the pathways for COVID-19 complications. Continued research on this important topic will inform clinicians, health system leaders, and policy makers on delivery of care for the growing number of Americans living with substance use disorders who are at high risk for COVID-19 and other infections.