Abstract
Applying a social determinants of health framework, this review brings attention to evidence from social sciences and neuroscience on the role of selected social factors in individual and population-level vulnerability to substance use and substance use disorders (SUDs). The understanding that social vulnerability to substance use and SUDs is multifaceted and occurs across different levels of influence (individual, interpersonal, community, and societal) is underscored. We propose that socially based stressors play a critical role in creating vulnerability to substance use and SUDs, and as such, deserve greater empirical attention to further understand how they “get under the skin.” Current knowledge from social sciences and neuroscience on the relationships among vulnerability to substance use resulting from stressors, exposure to socially toxic childhood environments, and racism and discrimination are summarized and discussed, as are implications for future research, practice, and policy. Specifically, we propose using a top-down approach to the examination of known, yet often unexplored, relationships between vulnerability to substance use and SUDs, related inequities, and potential differential effects across demographic groups. Finally, research gaps and promising areas of research, practice, and policy focused on ameliorating social vulnerabilities associated with substance use and SUDs across the lifespan are presented.
1. Introduction
A prodigious scientific literature has documented the multiform influence of life stress on human biology, mental health, and behavioral sequelae. Social determinants are pervasive sources of life stress experienced differentially in social systems. The ramifications of adverse stress exposures are demonstrably injurious to health, yet these exposures have been historically beyond the scope of societal responsibility to redress and outside the official scope of medical care practice. Informed by conceptual frameworks on the social determinants of health (Marmot and Wilkinson, 2006), health disparities (Alvidrez et al., 2019), and stress (Aneshensel, 1992). This paper explores how socially based stressors play a critical role in creating vulnerability to substance use.
Alcohol and drug misuse and related substance use disorders (SUDs) affect millions of individuals in the United States and throughout the world, with significant health consequences and economic costs to societies, communities, families, and individuals (Grant et al., 2015; U.S. Department of Health and Human Services [USDHHS], 2016). Although evident across all sectors of society, the prevalence and negative consequences of alcohol and drug use are generally greater among groups characterized by disenfranchised social status (e.g., poverty, stigmatized identity; Cerdá et al., 2010; Chartier and Caetano, 2010; Glass et al., 2020; Grant et al., 2015; Green and Feinstein, 2012; Reilly et al., 2019; USDHHS, 2016). A robust literature has documented the powerful effects of social environment and context on substance use initiation and disorders, their negative consequences, and treatment access and outcomes (Institute of Medicine [IOM], 2006; National Academies of Sciences, Engineering, and Medicine [NASEM], 2017, 2019a, 2019b; Prom-Wormley et al., 2017). A promising new area of research in the field of SUDs is investigating the interaction between genetic and environmental factors and how slight changes in gene expression can occur over time without altering DNA, known as epigenetics (IOM, 2006; NASEM, 2019a, 2019b; Prom-Wormley et al., 2017).
The vast literature on the neurobiology of substance use has largely focused on a “bottom-up” approach, defined as an approach focused on genetic and biological factors for understanding psychological and behavioral contributors to substance use vulnerability (Camarini et al., 2018; Heilig et al., 2016; Pelloux et al., 2019; Shimamoto, 2018; Tomek and Olive, 2018; Vannan et al., 2018; Yanovich et al., 2018). Only recently has neuroscience employed a “top-down” approach, defined as an approach focused on “diligently looking at the effect of social factors on drug use and addiction in animal models” (Pelloux et al., 2019, p. 1; also see Heilig et al., 2016). Because all human behavior, including and perhaps especially substance use, occurs in a social context (Galea et al., 2004), strict bottom-up approaches present a significant challenge for the translation of basic science to prevention and treatment. Likewise, social science research has much to gain by investigating how “social factors may modify relations between endogenous variables and substance use behavior” (Galea et al., 2004, p. 37). The distinct disciplinary differences in employing bottom-up versus top-down approaches to scientific inquiry on health are not specific to substance use. In fact, this difference was highlighted by the National Academies as a major challenge to interdisciplinary health research and yet key to the advancement of knowledge (IOM, 2006).
Interdisciplinary collaborations between basic and behavioral sciences have facilitated the investigation of biological factors that interact with social and societal factors to place individuals at risk of developing SUDs. Chronic exposure to stressors and a maladaptive stress response to those stressors can influence the development of physical dependence and SUDs. Multiple societal factors outside of an individual’s control may lead to increased exposure and vulnerability to chronic stress, including poverty (Evans et al., 2005), hunger and food insecurity (NASEM, 2019a, 2019b, 2020), homelessness and housing insecurity (NASEM, 2019a, 2019b, 2020), and discrimination (Metzger et al., 2017; NASEM, 2019a, 2020; Williams et al., 1997). Social stress theory (Aneshensel, 1992) suggests that people with disadvantaged social status (such as living below the poverty line and experiencing racial discrimination) are exposed to more stressors (Myers, 2009) and may be more vulnerable to maladaptive responses to stressors due to their chronicity and overwhelmed psychosocial coping resources (Cunliffe, 2016). Such exposure and resulting vulnerability, as explained by social stress theory, may lead to a higher risk of mental illness, including SUDs (Aneshensel, 1992). Approaches focused on downstream factors1 such as individual-level interventions, medical care, and treatment address consequences of these adverse conditions (e.g., substance use vulnerability and disorders). On the other hand, approaches that focus on upstream factors,2 such as those that seek to improve the conditions in which people live via changes in policies, housing, neighborhood conditions, and increased socioeconomic status, could have a more powerful impact at the population level by reducing exposure to modifiable chronic stressors (Braverman et al., 2011; Williams et al., 2008). Such upstream prevention efforts might include structural changes that alter how resources are distributed or how regulatory systems are governed; for example, health care policy and training for providers to assess social determinants of health (housing, access to food, neighborhood safety, chronic stress, and trauma) during medical appointments and a referral process to address areas of concern (NASEM, 2017, 2019a, 2019b).
The current paper brings attention to evidence from social sciences and neuroscience on the role of selected social factors in individual and population-level vulnerability to alcohol and illicit drug use and development of SUDs. We propose that socially based stressors play a critical role in creating vulnerability to substance use and as such, deserve greater empirical to further our understanding of how they “get under the skin.” More specifically, we focus attention on early and ongoing exposure to socially toxic environments, racism, and discrimination as foundational social factors in the psychobiological cascade that creates vulnerability to substance use and its consequences. Using a top-down approach (i.e., in which environmental, external, and human behavioral factors are mapped onto an individual’s psychological response, which can then be observed in biological processes; IOM, 2006), we bring attention to the known and yet often unexplored relationships between vulnerability to substance use and SUDs. Further, we underscore inequities in these foundational social factors and their potential differential effects across race and ethnic groups while noting the moderating and mediating effects of cultural, family, and individual factors.
We first present a conceptual framework to set the discussion in relation to social determinants of health and health disparities. Then, we present evidence from social sciences and neuroscience on the relationships among vulnerability to substance use resulting from stressors, exposure to socially toxic childhood environments, and racism and discrimination. Finally, we highlight research gaps and promising areas of research for deepening the understanding of these factors. Enhancing interdisciplinary approaches is critical to knowledge development because evidence from various disciplines indicates that the etiology of substance use and SUD is multifactorial. These etiological factors include genetic, psychological, and social factors that interact dynamically through the life course at multiple levels to influence vulnerability to substance use at the individual and population levels (Galea et al., 2004; IOM, 2006).
2. Role of social factors and their inequitable distribution in health and substance use
More than 100 years ago, scholar W.E.B. Du Bois (1899) documented the critical role of what today is referred to as social determinants of health, noting that they were systemically and unequally distributed across populations and resulted in health inequities. Differences in health between Whites and non-White populations were largely attributed to the biological inferiority of non-White populations (White, 2011). Dr. Du Bois, a sociologist of significant academic gravitas, challenged these prevailing notions through systematic studies, which provided epidemiological data on the social factors contributing to disease and disparities in the health of Black Americans (White, 2011). Arguably, his legacy informed the framing of our contemporary scientific understanding of how the health of populations is shaped by structural social factors and their cascading and interacting effects on intermediary life conditions they create.
Since that time, volumes of research have verified and expanded the evidence base on social determinants of health (IOM, 2003, 2006; NASEM, 2017, 2019a, 2019b, 2020; Takeuchi and Williams, 2011; White, 2011; Williams and Sternthal, 2010). The role of social factors in health is widely recognized by prestigious and credible scientific and public health organizations. The Institute of Medicine report Genes, Behavior and the Social Environment concluded that research has documented associations between social factors and health, behaviors and health, and genetics and health (IOM, 2006). Likewise, the World Health Organization has recognized the critical role of social factors in health and adopted a social determinants of health framework for understanding and addressing major health conditions and health disparities (Solar and Irwin, 2010). A robust body of scientific work has documented that structural factors (i.e., socioeconomic and political context and socioeconomic position) and intermediary factors (i.e., material circumstances, behavioral and biologic factors, and psychosocial factors) known to affect the health of populations are systematically and disproportionately distributed across population groups (e.g., economic status, gender, race, ethnicity; Adler et al., 2016; Commission on Social Determinants of Health, 2008; IOM, 2006; Marmot and Wilkinson, 1999; NASEM, 2017, 2019a, 2019b, 2020; Singh et al., 2017; Tarlov, 1996).
Applying a social determinants of health framework to the study of vulnerability to substance use, Galea et al. (2004) brought attention to the importance of investigating the contributions of structural determinants; that is, the socioeconomic and political context (i.e., features of governance, macropolitical policies, social and public policies, and cultural and societal values) that affect substance use and related health disparities. Additionally, how do these influence, and get influenced by, socioeconomic position (i.e., social class, occupation, income, gender, racism, education)? This, in turn, is thought to shape intermediary social determinants of health (i.e., material circumstances and behavioral, biological, and psychosocial factors) to affect health outcomes and health equity at the individual and population levels. As a result, these create consequential conditions of health inequities, including vulnerability to substance use (e.g., Boardman et al., 2001; Cave et al., 2020; Earnshaw et al., 2020; Fairman et al., 2020; Galea et al., 2004; Goldstein et al., 2020; Kamiker-Jaffe, 2011; Paradies et al., 2015; Savage and Mezuk, 2014; Spooner and Hetherington, 2004; Thompson et al., 2020; Tsai et al., 2019; Zoorob and Salemi, 2016).
3. Social determinants of health and disparities framework
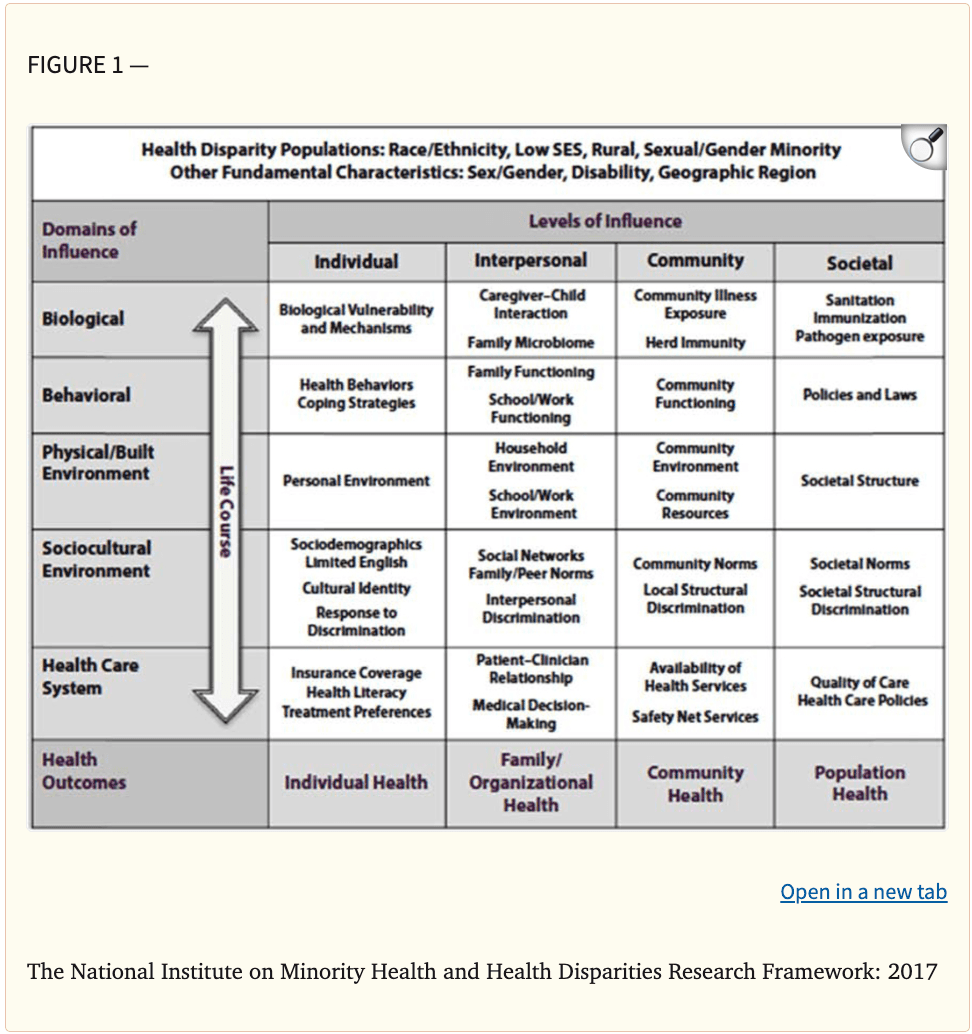
Building on this framework, more recently, the National Institute on Minority Health and Health Disparities (NIMHD) proposed a more detailed framework (see Figure 1) describing the wide array of determinants that promote or jeopardize health and health disparities (Alvirez et al., 2019). The NIMHD framework relies on an earlier framework proposed by the National Institute on Aging (Hill et al., 2015) and augments it by incorporating multifactorial levels (i.e., from individual to societal levels) of the widely used socioecological model of health and human development introduced by Bronfenbrenner (1977). As shown in Figure 1, the framework is represented as a matrix with domains of influence on health (y-axis) and levels of influence on health (x-axis), in which cells specify unique determinants applicable to the study of a particular health outcome or disparity, such as vulnerability to substance use. For example, stemming from the biological domain of influence in Figure 1, vulnerability to substance use, development of SUD, and related disparities are thought to be driven by multiple levels of influence (Galea et al., 2004). These include genetics (e.g., familial genetic predisposition) and biological factors such as sex and age (individual level), quality of parent–child relationships (interpersonal level), prevalence of SUDs in the community (community level), and availability of alcohol and illicit drugs (societal level). Starting from the sociocultural environment domain of influence, vulnerability to substance use, development of SUD, and related disparities may also be driven by socioeconomic position, cultural identities, and response to discrimination (individual level); social networks or family and peer norms and exposure to discrimination from others (interpersonal level); community norms regarding substance use and community-level structured discrimination including school policies, housing or law enforcement practices, and prevalence of violence and criminal activity (community level); and regional or national norms about substance use, structured discriminatory policies or practices that result in riskier environments, differential treatment of individuals and groups based on race and ethnicity, access to resources such as high-quality or evidence-based substance use prevention and treatment, and access to health insurance for such services (societal level). Importantly, the framework indicates that the domains of influence can act in dynamic and interactive ways through the lifespan and that health outcomes such as substance use may be observed beyond the individual (e.g., initiation of use or SUD diagnosis at an individual level) to the aggregate (e.g., prevalence of SUDs in a school or work setting, communities, or geographic areas; availability of SUD treatment and related rates of treatment utilization and treatment success in municipalities, states, territories, tribes, or nationally).
The NIMHD framework is aspirational and meant to promote greater scientific attention to research on levels of influence beyond the individual. In reality, R01 grants funded by the NIMHD, and arguably by the National Institutes of Health, predominantly focus on individual-level determinants (91%; Alvidrez et al., 2019). Studies that shed light on how socially activated disease-promoting exposures and inequitably structured conditions get under the skin via biological pathways are especially critical in furthering the understanding of how inequities in social determinants of health create, foster, or mitigate substance use vulnerability at individual and population levels.3
4. Public health parable and an illustrative case example
To highlight the importance of addressing upstream factors in health and the important role of social determinants of health and disparities, we turn to the quintessential public health parable and an illustrative case example. The parable shifts the focus from downstream (i.e., individual treatment or approaches) to upstream (i.e., population-level prevention strategies or approaches for the community at large).
In the classic public health parable credited to medical sociologist, Irving Zola, a member of the local community sees a man caught in a river current. She saves the man, only to be drawn to the rescue of more drowning people. After many have been rescued, she walks upstream to investigate why so many people have fallen into the river. She discovers a beautiful overlook along the river’s edge without any warning signs or protective barriers. (National Collaborating Centre for Determinants of Health, 2014, p. 1)
As in this example, addressing substance use and SUDs primarily via individual-level strategies once risk or disease states are evident is insufficient to influence and prevent ongoing exposures at the population level.
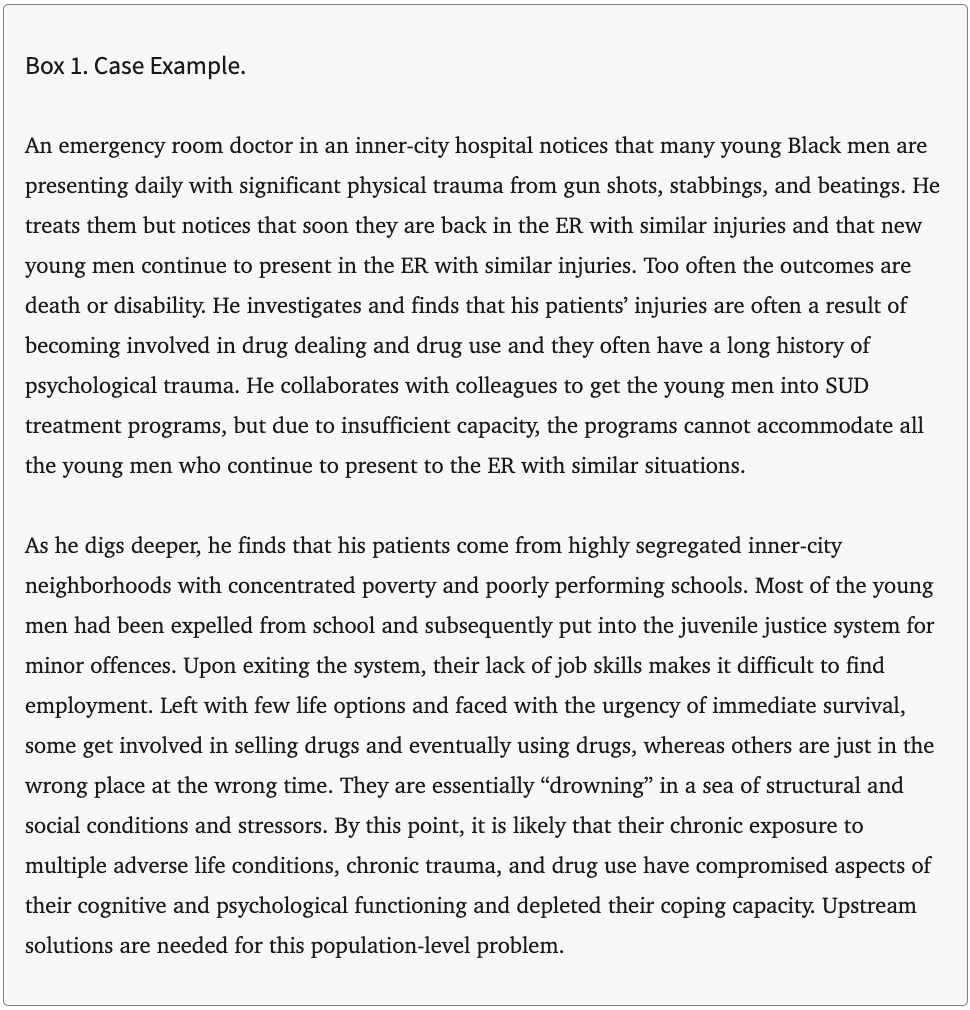
A case example specific to substance use is provided here to highlight the complexities and roles of social determinants of health in the etiology of vulnerability to substance use addressed in this paper (see Box 1). To construct this fictitious but likely representative case example, we relied on the work of Dr. John Rich, whose research has clearly elucidated the role of structural factors on the health of his patients and roots of their vulnerability (Rich, 2000, 2009; Rich and Grey, 2005).
Next, we discuss evidence regarding three social factors (i.e., socially determined stressors, exposure to socially toxic environments, and racism and discrimination) as examples of how social determinants of health and their consequential inequities produce vulnerability to alcohol and drug use, SUDs, and related consequences.
5. Role of stress, stressors, and stress response in vulnerability to substance use
The term stress has long been defined as “the nonspecific response of the body to any demand” (Selye, 1974, p. 27). It is important to highlight the critical role of a demand or stimulus (stressor) being present to activate the stress response. The stress response is a multifaceted reaction to a perception of danger or threat, which includes activation of the hypothalamic-pituitary-adrenal (HPA) axis, increased heart rate and blood pressure, decreased function of the digestive system, and tunnel vision; this is sometimes referred to as “fight or flight” (Cannon, 1929). When an acute stressor occurs, this physiological response can help individuals escape dangerous situations, making it advantageous and increasing survival among those with this response (Romero et al., 2015). However, chronic exposure to stressors leading to overactivation of the stress response has been shown to be disruptive to the body and interfere with other functions, such as reward pathways in the brain (Hughes et al., 2017; NASEM, 2019a, 2020; Shin et al., 2009; Thompson et al., 2017) and cardiovascular health and heart rate variability (Kim et al., 2018; Schubert et al., 2009), placing individuals at greater risk of substance use (NASEM, 2020) and developing a SUD (Sinha, 2008).
Social determinants of health such as socially derived chronic and prolonged stressors (e.g., loss or separation from a parent at an early age; incarceration; concentrated poverty; systemically thwarted opportunities due to discrimination; parental divorce or conflict; emotional, physical, or sexual abuse; violence; neglect; isolation; and loss of home to natural disaster) are predictive of SUDs (Balk et al., 2009; Buzawa and Buzawa, 2014; Hughes et al., 2017; NASEM, 2019; Rivas-Rivero et al., 2020; Shin et al., 2009; Sinha, 2008; Thompson et al., 2017). Broadly speaking, social determinants of health and inequities are systemic and structured external forces or stimuli that can result in chronic activation of the stress response. Throughout this section, we use the term stress to refer to the body’s response to stimuli and refer to the stimuli as stressors.
5.1. Stressors and stress response in the social determinants of health framework
As proposed in Figure 1, socioeconomic and political contexts create an environment in which populations are systematically and differentially exposed to varying degrees of risk and protective factors for health and well-being based on their social class, gender, ethnicity, education, occupation, and income (Alvidrez et al., 2019). Based on where someone fits in each of those categories, they have access to material circumstances such as safe living or working conditions, food, or health care. When considering how stressors and the stress response fit in this framework, we can start by acknowledging the stressors associated with the experience of having lower social status than others. In human and animal studies, prior research has found subordinate social status (i.e., lack of respect from peers, perceived as less competent or less important) to be associated with increased pro-inflammatory cytokines (Muscatell et al., 2016), increased risk of chronic social defeat stress (Larrieu et al., 2017), and increased cortisol (Sherman and Mehta, 2020), all of which influence an individual’s health, well-being, and vulnerability to substance use (Sinha, 2008). The presence of these chronically (and sometimes intergenerationally) occurring stressors creates an overactivated stress response, which leads to a feedback loop of challenges in the environment such as access to health care, costs of stress-related illness creating financial hardship, and difficulty obtaining and maintaining employment or completing educational training, reducing one’s social positioning (Howe et al., 2017).
There are many ways to assess stressors and the body’s response to exposure to those stressors. For example, the Perceived Stress Scale is commonly used to assess the degree to which individuals perceive their lives to be stressful and perceived physiological responses to those stressors, such as the frequency of upsetting events happening unexpectedly and the frequency of feeling physically nervous, anxious, or stressed by these events. This scale has been associated with poor self-reported health, elevated blood pressure, depression, and susceptibility to infection (Cohen et al., 1983). To assess the perception of external stressors, it is important to also explore the internalization of these stressors and biological mechanisms of the stress response. For example, many clinical studies use salivary cortisol as a measure of stress; salivary cortisol gives us an estimate of the HPA function (Sampedro-Piquero et al., 2020). Cortisol can also be measured using hair samples, which is thought to be less invasive but requires further investigation in human and animal models before validity and reliability can be concluded (Burnard et al., 2017). Neuroimaging techniques are also used to assess brain region activation in areas such as the nucleus accumbens and the dorsal medial prefrontal cortex during experimental manipulations designed to activate the stress response (Muscatell et al., 2016).
5.2. Epidemiology and population-level research on stress and substance use
The relationship between stress and substance use has been established in the literature from bench and laboratory to clinical and bedside science and is acknowledged as bidirectional and complex, with evidence to support stress leading to greater substance use, and substance use leading to greater stress (Ramchandani et al., 2018). It is also well documented that stress vulnerability is a significant risk factor for initiation of alcohol and drug use and development of SUDs (Sinha, 2001, 2008). Stress vulnerability is a term used to describe a weakened stress response in the brain, possible due to a prolonged disruption of neurotransmitters such as gamma-aminobutyric acid. The stress–vulnerability hypothesis suggests the relationship between stress and substance use is mediated by risk and protective factors, such as social support, history of depression, coping, and self-efficacy (Brown et al., 1990; Brown et al., 1995).
Stressors do not occur in isolation, making it difficult if not impossible to assess a single stressor’s impact on an individual. The response to a single stressor is based on a lifetime of development and adaptions to prior stressors (Lloyd and Turner, 2008). Evolutionarily, it is beneficial for the stress response to be malleable to help people adapt to the environment, learn from dangerous situations, and respond more efficiently. Rodent and human studies have identified similarities in the threat evaluation and response system, which favors (at least in the short term) sensitivity to false positive responses (i.e., evaluating a threat when there is no threat, like running from a shadow that is not a predator) over false negatives (i.e., evaluating no threat when there is a threat, or not running from a predator at the first sight of a shadow; Moscarello and Hartley, 2017). However, in the long term, frequent exposure to stressors, including those that an individual cannot avoid or control, can lead to overactivation of the stress response throughout the lifetime, resulting in a blunted stress response in adulthood and later in life (Lupien et al., 2009; Moscarello and Hartley, 2017). Overactivation of the stress response can lead to higher basal state of arousal (even in the absence of immediate danger) and less functional stress response following exposure to stimuli designed to activate the stress response (Koob, 2009; Sinha, 2008). This pattern of a higher basal level of stress and poorer stress response activation is also present in individuals with SUDs (Blaine et al., 2019). Individuals may be more likely to develop an alcohol use disorder if they consume alcohol as a form of coping with social anxiety or stress during negative social interactions (Sinha, 2001).
5.3. Biological and clinical research on stress and substance use
The complexity of the relationship between stress and substance use cannot be explained through social environment alone. An interdisciplinary integration of neuroscience and social science is necessary to identify factors that produce increased susceptibility to substance use initiation, addiction, and relapse (Koob and Le Moal, 1997). Neurobiological studies have provided evidence, through rodent models, of genetic vulnerability and sensitivity to stress leading to adaptations in the HPA axis responsiveness related to the development and maintenance of addiction (Koob and Volkow, 2016; Sinha, 2001). These adaptations cause dysregulations, interfere with reward and motivational processes in the brain, negatively influence the ability to cope with stressful events (Cadoni, 2016). Neuroimaging evidence supports a link between the stress response pathways in the brain and the reward pathways involved in complex decision making, memory, learning, and risk taking (Koob, 2008; Sinha, 2001, 2008). Beyond the initiation of substance use, it is well established that the motivation to continue using can be explained by a change in the function of neurotransmitters associated with reinforcing effects, such as dopamine, serotonin, and gamma-aminobutyric acid, which also includes pathways in the brain associated with stress systems and disruption of those systems (Koob and Le Moal, 2005).
Sinha (2008) identified three types of stress vulnerability factors that increase risk of developing SUDs: (1) genetic influences and family history of psychopathology; (2) developmental and individual-level factors such as executive function, negative emotionality, impulsivity, and altered initial sensitivity to rewarding effects of drugs; and (3) early adverse life events, trauma and child maltreatment experiences, and prolonged and chronic stress experiences. These three factors can be seen in the first three columns of Figure 1—individual, intrapersonal, and community factors of health and well-being—each of which influences the others and the rows in the framework across the life course, including biological pathways involved in stress regulation and behavioral control.
Activation of the stress response is related to craving of alcohol and other substances (Cavicchioli et al., 2020). In two samples of individuals with alcohol use disorder, craving mediated the relationship between the activated stress response following exposure to stressors and next-day alcohol intake (Wemm et al., 2019). The relationship between activation of the stress response and craving has also been investigated in animal models; for example, studies using animals with drug or alcohol dependence have shown increases in drug seeking (comparable to craving in humans) when presented with stimuli designed to provoke the stress response (Le et al., 2000; Mantsch et al., 2016). Similar findings emerged in human models when provoking an acute stress response in the laboratory, which resulted in an increase in alcohol and drug craving (Sinha, 2001, 2009; Sinha and Li, 2007).
Animal models have provided evidence of potential protective factors that may help reduce substance use and abuse. For example, Venniro and colleagues (2018) found that rats deprived of social interactions with other rats self-administered available drugs, but when given the opportunity and choice, they preferred social interactions over drug administration. This finding was consistent across drug class, drug dose, gender, sex, and abstinence duration. This research supports the important role of social interaction and support in substance use treatment. Other animal model research has compared enriched environments with deprived environments and found differential changes in brain development among adolescents raised in these environments, specifically documenting negative effects in deprived environments and positive effects in enriched environments regarding the amygdala, hippocampus, and frontal cortex, which all play an important role in stress response and behavioral and impulse control (Lupien et al., 2009).
A promising new area of research in the field of SUDs is investigating the interaction between genetic and environmental factors and how slight changes in gene expression can occur over time without altering DNA, known as epigenetics. A recent literature review discussed how early life experiences and environmental factors can interact to influence gene expressions in addiction phenotypes, which may help explain how behavioral traits are passed between generations (Ajonijebu et al., 2017). The investigation of specific genes involved in epigenetic changes that may be regulated by the environment, such as the proprotein convertase subtilisin/kexin 9 enzyme (PCSK9), may lead to the development of innovative pharmacological treatments and manipulations of gene expressions to create protective phenotypes. Lee and colleagues (2019) found that treatment based on this enzyme attenuated alcohol-induced steatohepatitis in a rat model, which suggests the potential for future novel treatments for humans with liver disease resulting from alcohol use. Although such treatments are critical for individuals with SUDs, using this information to create population-level interventions is also needed to reduce exposure to chronic stressors and create protective factors among the most vulnerable. More research is needed to determine the intergenerational effects of adverse life events altering gene expression and how this information can be used to create long-term upstream prevention programs for vulnerable populations.
6. Role of socially toxic environments in childhood and substance use vulnerability
The foundation for a lifetime of social, emotional, and physical health is set during childhood. Some have argued that these developmental processes begin prenatally through dynamic ongoing interaction between biology and the environment and can have lasting impacts across the life span (Entringer et al., 2011; Oberlander et al., 2008; Paul et al., 2021). Early positive experiences strengthen developing biological systems and cognitive and emotional development, whereas exposure to toxic environments increases morbidity and mortality and limits access to life opportunities (Felitti et al., 1998; Metzler et al., 2017; Shonkoff, 2016). Exposure to socially toxic childhood environments has been linked with most major causes of death in U.S. adults (Campbell et al., 2016), with particularly robust associations with substance use (Hughes et al., 2017) including early initiation (Dube et al., 2003), SUDs (Halpern et al., 2018), and relapse (Hyman et al., 2008).
Socially toxic environments in childhood can be defined as stressful chronic experiences that occur during childhood that either directly (e.g., physical abuse or neglect) or indirectly (e.g., housing, economic instability, community violence, experiences of racism) affect children through their living environments. Various terms have been used to refer to life conditions that pose adversity and threaten well-being. For example, Garbarino (1995) coined the term “socially toxic environment” to refer to social contexts (e.g., violence, poverty, other economic pressures on parents and their children) in which children grow up in a state of degradation that presents serious threats to their healthy psychological and social development. During the same period, the term “adverse childhood experiences” (ACEs) originated in a groundbreaking study of the prevalence of various forms of physical and emotional abuse, neglect, and household dysfunction and their association with negative life outcomes including substance abuse (Felitti et al., 1998). Subsequently, the National Scientific Council on the Developing Child (2004) coined the term “toxic stress” to describe the well-documented effects of excessive activation of stress response systems on a child’s developing brain, immune system, metabolic regulatory systems, and cardiovascular system. Importantly, in addition to sources of adversity captured in ACEs, it also included community and systemic issues (e.g., community violence, experiences with racism and chronic poverty; Center on the Developing Child, 2020; Shonkoff et al., 2009; Shonkoff et al., 2012). In this paper, we use the term “socially toxic environments” to refer to these multiple sources of adversity that begin in childhood and have lifelong consequences for health and vulnerability to substance use.
6.1. Exposure to socially toxic environments in the framework of social determinants of health
In the framework presented in Figure 1, exposure to socially toxic environments is in the sociocultural environment domain of influence. It operates at the individual, interpersonal, community, and societal levels and is associated with health disparities at each level throughout the lifecycle (Amaro et al., 2020; NASEM, 2017). As noted in national reports on key factors affecting childhood health (NASEM, 2019a) and adolescent health (NASEM, 2019b), the manifestations and mechanisms of exposure to socially toxic environments at different socioecological levels are well documented.
Examples of the mechanisms through which socially toxic environments work include individual-level factors like economic insecurity, housing instability (Buu et al., 2009; Cambron et al., 2019), and exposure to child maltreatment (Dubowitz et al., 2020); and interpersonal factors like family conflict (Wadman et al., 2020), parental substance use (Abar et al., 2015), parental separation (Jackson et al., 2016) and perceived discrimination (Chavez et al., 2018; Davis et al., 2019; Rogers et al., 2020). At the community level, mechanisms include concentrated neighborhood disadvantage and crime (Burlew et al., 2009; Handley et al., 2015) and exposure to community violence (Motley et al., 2017), whereas policies that separate immigrant families and limit economically disadvantaged children’s access to high-quality early childhood education are a societal influence (NASEM, 2019a).
6.1.1. Biological perspectives: How toxic environments get “under the skin”
Increasing biomedical evidence supports the plausibility of causal epigenetic changes in people exposed to adversity, many of which have been linked to greater susceptibility to acquiring a SUD (Kundakovic and Champagne, 2015; Iacono et al., 2018; McLaughlin et al., 2019; Shin et al., 2018; Somaini et al., 2011; Teicher et al., 2016). Exposure to toxic stress during childhood can disrupt developing brain architecture and other maturing organs, dysregulate metabolic processes, and excessively activate the stress system (Hughes et al., 2017; Scheidell, 2018; Shonkoff and Garner, 2011). It can also disrupt neurodevelopment and various neurological functions, including cognition, memory, and emotional functioning, that have been linked to drug initiation and continued use (Franke, 2014; Zannas and West, 2014).
McLaughlin and colleagues (2019) conducted a systematic review of 109 studies examining associations between neural development and multiple exposures to toxic environments in children (physical, sexual, and emotional abuse; domestic violence; other forms of violence; multiple forms of deprivation like institutional rearing; physical and emotional neglect; and extreme material deprivation). Findings indicated that children exposed to such threats had (a) reduced amygdala, medial prefrontal cortex (mPFC), and hippocampal volume and heightened amygdala activation to threat; and (b) reduced volume and altered function in frontoparietal regions. There is also some limited evidence for accelerated development in amygdala-mPFC circuits, with most studies suggesting a delay among maturation in children exposed to adversity (McLaughlin et al., 2019).
A substantial body of evidence also suggests that the possible dysregulation of neuroendocrine responses and neurotransmitter function induced by exposure to trauma and neglect during childhood could constitute one of the essential biological changes that link these early adverse experiences with substance abuse vulnerability (Gerra et al., 2008; Heim et al., 2002; Shea et al., 2005). Somaini and colleagues (2011) conducted a review of existing evidence on the associations between biological changes induced by childhood adversity and substance use. Evidence indicated that HPA function based on secretion levels of cortisol is associated with childhood adversity and contributes to addiction vulnerability later in life. Additionally, higher frequency of the serotonin transporter 5-HTT SS genotype is associated with an increased susceptibility in the use of illegal psychotropic drugs among adolescents, suggesting that the low-activity S allele may influence behavioral traits and substance use vulnerability (Gerra et al., 2005), likely prompting an impairment of brain serotonin transmission (Blier et al., 1987; Coccaro et al., 1996). Parental neglect is also associated with higher plasma levels of two HPA hormones linked to drug use. Specifically, studies have found positive associations between basal plasma levels of cortisol and adrenocorticotropic hormone (ACTH) and parental neglect scores on Childhood Experiences of Care and Abuse Questionnaire (Somaini et al., 2011). Interactions between genetic factors and parental behavior have also shown to predict drug use susceptibility among youth exposed to adverse childhood conditions (Somaini et al., 2011). Additionally, studies have found exposure to toxic environments and adversity during childhood can also affect immune function and permanently change the responsiveness of the peripheral immune system to a substance of abuse, such as cocaine (Iacono et al., 2018).
Although there is a burgeoning field of knowledge on the biological mechanisms underlying the associations between socially toxic childhood environments and substance use vulnerability, limitations remain. Notably existing evidence comes primarily from small and heterogeneous samples with cross-sectional research designs that hinder a comprehensive understanding of the neurobiological consequences of socially toxic childhood environments. Future research with larger samples and pooled data across labs, more precise measurements of adversity, and longitudinal studies that track these biological mechanisms over time are needed to further elucidate these associations (McLaughlin et al., 2019).
6.2. Mechanisms linking socially toxic childhood environments to SUD
Various mechanisms have been posited to explain how childhood adversity affects subsequent SUDs. Childhood is a highly formative development period; thus, exposure to traumatic events and co-occurring chronic stress can lead to cognitive and social disruption from an early age. Extant evidence indicates associations between socially toxic childhood environments, unhealthy coping mechanisms, and depression and other mental health disorders, leading to self-medication with drugs in an attempt to regulate negative emotions (Dube et al., 2001; Heim et al., 2009; McCauley et al., 1997). The following sections provide an overview of biological and social factors associated with childhood adversity, limitations in the current body of evidence, and suggestions for future directions of research.
6.2.1. Social perspectives on socially toxic environments in childhood
As previously noted, along with the biological implications associated with socially toxic childhood environments, social factors are related to these conditions across multiple levels of influence. In the following section, we provide a few examples of these risk factors across domains. At the individual level, economic insecurity is often a key driver associated with socially toxic environments in childhood. Socioeconomic disparities exist across race and ethnicity and geographic region. For instance, Black, American Indian or Alaska Native, and Hispanic children are more likely to live in low-income and poor households or in deep poverty (below 50% of the federal poverty threshold). Racial and ethnic disparities also exist in social mobility. Evidence suggests that Black and American Indian or Alaska Native children have the lowest rates of upward mobility, even when controlling for parental income (Chetty et al., 2018). Vast evidence exists linking economic insecurity with numerous adverse health outcomes in youth, including greater vulnerability to substance use (Buu et al., 2009; Lee et al., 2013).
At the interpersonal level, research on resilience has overwhelmingly demonstrated that that a key protective factor for children facing childhood adversity is a safe, stable, and nurturing relationship with at least one caretaker. These parent–child bonds help foster positive outcomes across domains ranging from healthy psychological adjustment to positive peer relationships (Bornstein and Leventhal, 2015; Bronfenbrenner and Morris, 2006; Centers for Disease Control and Prevention, 2014; Luthar, 2006; Masten et al., 2014; National Scientific Council on the Developing Child, 2004). Supportive relationships early in life also play a key role in buffering stress responses, thereby allowing children to more easily confront stressful situations (Hostinar and Gunnar, 2015).
Because most studies have examined individual and interpersonal factors associated with socially toxic environments in childhood, it is important to consider the broader contextual factors that lead to socially toxic environments. Indeed, a child’s ZIP code, which captures upstream features of the social and economic environment and related resources, has been found to be more important than genetics in determining future health and life chances (Lavizzo-Mourey, 2014). Although not an exhaustive list, these community and societal factors include neighborhood and community conditions such as concentrated neighborhood disadvantage (Handley et al., 2015), neighborhood and exposure to community violence (Burlew et al., 2009), economic insecurity, housing instability (Buu et al., 2009), access to health care and early education (Cannon et al., 2017; Jones et al., 2015), immigration-related factors (Schwartz et al., 2015; Unger, 2015), and discrimination (Cave et al., 2020), all of which have been linked with increased substance use vulnerability (Trucco, 2020).
For instance, previous studies found associations between higher unemployment rates and adolescent risk of marijuana use initiation (Tucker et al., 2013). Similarly, neighborhood disadvantage was linked with greater marijuana dependence symptoms, but only among youth exposed to child maltreatment (Handley et al., 2015). Youth exposed to high-risk contexts including neighborhood criminal activity (e.g., neighborhood rates of arrests, robbery, illicit drug use) have shown higher rates of early substance use initiation by middle school (Burlew et al., 2009). Similarly, children exposed to unstable housing and residing in unstable neighborhoods characterized by high residential mobility (i.e., residents moving in and out frequently) were more likely to develop various SUDs during late adolescence (Buu et al., 2009). Moreover, adolescents residing in neighborhoods with greater concentrated disadvantage were more likely to be exposed to substances, which in turn, enhanced availability of and opportunities for substance use (Cerdá et al., 2010). Neighborhood features such as social cohesion (i.e., extent of connectedness and solidarity among groups in a community) and social capital (features of social structures such as interpersonal trust, norms of reciprocity, and mutual aid) vary across neighborhoods and are associated with better health (NASEM, 2017). They serve as resources for individuals, facilitate collective action, and when absent, can contribute to health disparities (Amaro et al., 2020; Kawachi and Berkman, 2000; NASEM, 2017). For example, neighborhoods with low levels of collective efficacy (i.e., residents’ willingness to intervene in the face of neighborhood problems such as criminal activity on behalf of the community)—one aspect of social capital (Amaro et al., 2020; NASEM, 2017)—are less likely to have the capacity to monitor and enforce proper conduct among residents, thereby leading to increased levels of substance use (Handley et al., 2015; NASEM, 2017). Some investigators have suggested that under certain conditions (e.g., low socioeconomic status, high-crime communities), some aspects of social capital may present additional sources of strain and facilitate high-risk behaviors such as substance use via contagion effects (NASEM, 2017). Longitudinal studies have shown the impact of neighborhood-related factors on vulnerability to substance use does not halt in adolescence but can have lasting impacts well into adulthood and throughout the lifespan (Lee et al., 2018; Zimmerman et al., 2017).
Yet another important factor to consider is children’s access to early care and education (ECE). ECE is defined here as nonparental care provided outside the child’s home. ECE services can be delivered in various venues including center- and school-based settings (i.e., a setting other than a child’s home; NASEM, 2018). ECE provides numerous pathways to improving health and achieving health equity, including academic readiness; cognitive and socioemotional development; and overall positive impacts on physical, emotional, and mental health and well-being among youth and into adulthood (Campbell et al., 2014; D’Onise et al., 2010; Hahn et al., 2016; Muennig et al., 2011; NASEM, 2019a). Specifically, engagement in ECE programs has been associated with reduced externalizing and internalizing behaviors (Carney et al., 2015), including reduced substance use (Cannon et al., 2017; Jones et al., 2015). Currently, eligibility for ECE programs is limited. Even among families that are eligible, accessibility is low due to funding deficits and limited availability of programs and services (NASEM, 2018). As such, publicly funded ECE programs do not reach most children, and this is especially true for children exposed to socially toxic environments (NASEM, 2019a). For instance, parents with lower levels of education, income insecurity, and limited English proficiency are less likely to participate in ECE programs. It is also important to note that access to ECE does not guarantee equitable access to quality care, particularly for children from economically disadvantaged homes and racial and ethnic minorities such as Black and Hispanic children, who are more likely to receive lower-quality care compared to White and Asian children (Barnett et al., 2013; Valentino, 2018).
Children from immigrant families also face unique barriers that have the potential to make them particularly vulnerable to socially toxic environments. Although most children in immigrant families are U.S. citizens (90%), approximately one quarter have an unauthorized immigrant parent (Koball et al., 2015). Regardless of their own citizenship status, many are adversely affected by their household context and the sociopolitical context surrounding U.S. immigration policies (Filindra et al., 2011; Koball et al., 2015). Current U.S. immigration policies have become a salient source of toxic stress for these families and their children. For instance, fears of parental deportation among children have been linked with adverse physiological and psychological outcomes including eating and sleeping problems, headaches, stomachaches, depression, and anxiety (Artiga and Ubri, 2017; Rojas-Flores et al., 2017). Dramatic recent increases in immigrant deportation and the detention of parents seeking asylum at the border have resulted in thousands of children being separated from their families (HHS Office of Inspector General, 2019). Additionally, recent immigration policies have affected parents’ willingness to enroll their children in public programs, including ECE settings (Cervantes et al., 2018). These barriers could be exacerbated as increasing efforts to limit access to government services, such as health care, through the public charge rule take effect at the federal or state levels (Kaiser Family Foundation, 2019).
Numerous sociocultural factors have also been linked with elevated prevalence of substance use among youth from immigrant families. For instance, previous research has found increased substance use among Hispanic youth is associated with decreased family cohesion as children adopt individualistic U.S. values more rapidly than their parents; traditional cultural values such as religiosity and familism erode; and families face immigration, cultural, and economic stressors and exposure to ethnic discrimination (Schwartz et al., 2015; Unger, 2015).
In this section, we reviewed a few key factors associated with socially toxic childhood environments and subsequent substance use vulnerabilities. Given the multitude and complexity of factors that trigger such conditions, there remains a pressing need to address socially toxic childhood environments through multisectoral efforts that build comprehensive resources by combining individual, interpersonal, community, and policy efforts and interventions at the local, state, and national levels. Notably, one element of socially toxic childhood environments cuts across all levels of influence: racism and discrimination. Racism and discrimination shape the lived experiences of racial and ethnic minority children and families. It manifests in the unequal distributions of social, economic, and environmental resources that lead to deep-rooted biological, psychological, social, and environmental consequences (NAMEM, 2017, 2018). The following section is dedicated to the impacts of racism and discrimination on social vulnerabilities in substance use.
7. Role of discrimination and racism in vulnerability to substance use
The history of science and the social construction of race has been inextricably connected in the United States. Racialized views and perspectives played an important role in the intellectual freedom of the United States from Europe. As Gould (1996) argued, American polygeny, the belief that human races stem from different species, was a primary theory that gained recognition in the international science arena. Keel (2013) further pointed out that this scientific movement developed right before the American Civil War, during a time of uncertainty when the country was fervent about establishing racial inequalities (Cox, 2020).
The term racism was scarcely used in the early part of the 20th century. It first appeared in an unabridged version of the Merriam-Webster Dictionary in the late 1930s. Since then, the definition has been revised numerous times (most recently in June 2020) to capture its multiple dimensions. According to Merriam-Webster (2020), “racism is a belief that race is a fundamental determinant of human traits and capacities and that racial differences produce an inherent superiority of a particular race, which manifests in behaviors or attitudes that reflect and foster discrimination or prejudice; the systemic oppression of a racial group to the social, economic, and political advantage of another; and a political or social system founded on racism and designed to execute its principles.” In summary, “racism is often defined as individual prejudice, but racism is also systemic, existing in the advantages and disadvantages imprinted in cultural artifacts, ideological discourse, and institutional realities that work together with individual biases” (Salter et al., 2017, p. 1). As noted by Williams and colleagues (2019), racism manifests via institutional, cultural, and interpersonal forms in which individuals or institutions, with or without intent, treat racial and ethnic groups differently, resulting in inequitable access to opportunities and “self-reported discrimination, a subset of these experiences that individuals are aware of” (p. 111). A key aspect of racism is differential power relations, which disadvantages the less powerful group(s) in decisions related to allocation of goods and resources (e.g., placement of environmental hazards in or near minority communities, quality of public services, education and housing quality, employment opportunities, and access to and quality of health care; Adler et al., 2016; IOM, 2006; Jones, 1997; NASEM, 2017, 2019a, 2019b).
7.1. Racism in the framework of social determinants of health
In the framework presented in Figure 1, racism is identified as part of the sociocultural environment domain of influence. It operates at the intrapersonal, interpersonal, community, and societal levels and is associated with differential health outcomes and disparities at each level and throughout the lifecycle (Alvidrez et al., 2019; NASEM, 2017). As noted in various national reports (IOM, 2003; NASEM, 2017, 2019a, 2019b, 2020), the manifestations of racism are vast and its mechanisms at different socioecological levels are well documented.
Not intended to be comprehensive, the following list provides some examples of mechanisms through which racism works. These mechanisms include stereotype threat, which manifests as self-doubt and can undermine performance (Aronson et al., 2013; Spencer et al., 2016) and have other negative consequences (see review by Williams et al., 2019); implicit racial bias or unconscious cognitive biases (Dasgupta, 2013; Dovidio et al., 2002; FitzGerald and Hurst, 2017; Gershenson and Papageorge, 2018; Maina et al., 2018; Williams and Mohammed, 2013) that shape attitudes and behaviors toward members of racial and ethnic minority groups (interpersonal level); and racial profiling by police (Fagan et al., 2010; Fagan et al., 2014; Geller and Toch, 1996; Plant and Peruche 2005), inequitable practices by the criminal justice (Kovera 2019; Kurlychek and Johnson, 2019) and child welfare (Dettlaff et al., 2020; Gourdine, 2019; Maguire-Jack et al., 2020) systems, and differential disciplinary practices in schools (Amemiya et al., 2020; Okonofua and Eberhardt, 2015; Riddle and Sinclair, 2019) and health care institutions (IOM, 2003; Johnson, 2020; NASEM, 2017, 2019a, 2019b, 2020; institutional level). In addition, at the social environment level, it operates via systemic and interactive mechanisms facilitated by policies and practices such as residential or neighborhood and school segregation, disproportionate exposure to environmental toxins, discriminatory banking and lending practices, gerrymandering, and redlining voter suppression (community, state, and federal levels; see Bell and Ebisu, 2012; Bravo et al., 2016; Williams et al., 2019 for reviews; also see NASEM, 2017). As such, “racism is considered a fundamental cause of adverse health outcomes for racial/ethnic minorities and racial/ethnic inequities in health” (Williams et al., 2019, p. 1).
7.2. Epidemiology of racism and discrimination and manifestation of differential vulnerability
Although a robust literature has documented significant racial and ethnic disparities in many physical health indicators (Adler et al., 2016; IOM, 2003, 2006; NASEM, 2017, 2019a, 2019b, 2020; Williams and Collins, 2001; Williams and Jackson, 2005), the evidence on racial and ethnic disparities in mental health, including SUDs, indicates a more complex relationship (Carter, 2007; Chartier and Caetano, 2010; Mezuk et al., 2010). The epidemiological evidence indicates that the prevalence of substance use and SUDs varies by race and ethnicity (USDHHS, 2016). The latest data from the Monitoring the Future national survey show that in the eighth and 12th grades, Hispanic students have the highest use rates for most drugs compared to other groups, whereas African American students have lower levels of use for certain drugs other than heroin and bath salts (Johnston et al., 2019; note the report does not provide data for other racial and ethnic groups). Data from the 2015 National Survey on Drug use and Health suggest that members of minority groups aged 12 or older have similar or lower rates of binge drinking and alcohol use disorder as Whites—with the exception of American Indians or Alaska Natives, who have higher rates (USDHHS, 2016). Past-30-day illicit drug use is similar or only slightly higher among most minority groups compared to Whites. Exceptions are American Indians, Alaska Natives, Native Hawaiians, and other Pacific Islanders, who have higher rates of drug use disorder (USDHHS, 2016). However, important within-group variations exist in substance use and SUDs—for example, factors related to ethnic heritage, immigration, cultural affiliation and identity, acculturation processes, and acculturative stress are associated with substance use among both youth and adults (Abraido-Lanza et al., 2016; Ahmmad and Adkins, 2020; Blanco et al., 2013; Cano et al., 2017; Fish et al., 2017; Lui and Zamboanga, 2018; Meca et al., 2017; Meca et al., 2019; Myers, 2009; Pittman et al., 2017; Salas-Wright et al., 2018; Savage and Mezuk, 2014; Unger et al., 2014; Vilsaint et al., 2019).
Notably, a different pattern emerges if substance use and substance-related disorders are analyzed at different stages of the life course. Specifically, noninstitutionalized Blacks have lower levels of substance use (Johnston et al., 2020) and substance use-related disorders (Wu et al., 2011) during adolescence compared to Hispanics and Whites, and this also seems true among juvenile justice-involved youth (Welty et al., 2016). However, after age 25, a racial and ethnic crossover effect has been documented, primarily among Blacks, featuring an increase in the prevalence of substance use and SUD (Banks and Zapolski, 2018). For example, Watt (2008) found that after age 35, Black men report a higher prevalence of overall illicit drug use and Black women report a higher prevalence of heavy drinking compared to Hispanics or Whites. Study findings also suggest the crossover effect reverses after controlling for compositional characteristics (all factors influenced by racism and discrimination) such as socioeconomic status, education, employment, social support, and drug exposure. Further, numerous studies report significant associations between experience of discrimination and substance use and SUD among minorities (Ornelas et al., 2011; Otiniano Verissimo, Gee et al., 2014; Otiniano Verissimo, Grella et al., 2014). These findings suggest that the compounded and systemic effects of racial and ethnic discrimination may lead to increased substance use and SUDs later in life (Assari et al., 2017).
Reports of race- and ethnicity-based discrimination are ubiquitous among minorities (e.g., Assari, 2020; Bleich et al., 2019; Casey et al., 2019; Findling et al., 2019; Lee et al., 2019). The effects of social exclusion can affect almost every aspect of well-being. For example, racially segregated entrenched schools (Reardon and Owens, 2014) and neighborhoods (Hardy et al., 2018) have been linked with decreased intergenerational mobility (Andrews et al., 2017). In addition, higher education does not confer the same health benefits for Blacks compared to Whites (Shuey and Willson, 2008), and the compounded effects of the widening racial wealth gap (Darity et al., 2018) have been associated with poorer health (Shuey and Willson, 2008).
Racial and ethnic disparities in employment are also pervasive. Black workers are two times as likely to be unemployed as White workers at virtually every level of education. Blacks are also more likely to be underemployed and earn substantially less when employed compared to Whites (Pettit and Ewert, 2009; Western and Petit, 2005; Williams and Wilson, 2019). Currently, unemployment rates are higher in all minority groups compared to Whites (Pew Research Center, 2020). These disparities are further exacerbated when considering the effect of criminal records on employment access and earnings among racial and ethnic minorities, and this is further exacerbated by incarceration (Holzer et al., 2005; Lyons and Pettit, 2011; Pager, Bonikowski, et al., 2009; Pager, Western, et al., 2009).
Prior research has also documented the deleterious effects of racism on health outcomes, including access to health care, quality of health care, health care policies and practices, and ultimately, the overall health of people of color. A robust body of evidence has established a link between discrimination experiences and negative health outcomes in children, youth, and adults. The cumulative negative effects of discrimination on health using varied health outcomes have also been documented (see review by Williams et al., 2019). Further, previous research on discrimination in health care settings has also shown that minorities experience discrimination significantly more than non-Hispanic Whites (Williams et al., 2019) and that such experiences are associated with more negative patient experiences of health services, including distrust, dissatisfaction, and communication barriers and related outcomes such as delaying or not getting health care and lack of adherence to treatment (see meta-analysis by Ben et al., 2017). Research on personal experiences of discrimination or racism among individuals with SUDs is limited. Such studies have shown that active drug users experience high rates of discrimination and stigma based on their drug use and many other factors such as race and ethnicity, criminal justice history, and mental health problems (Ahern et al., 2007; Kulesza et al., 2013; Minior et al., 2003; Otiniano Verissimo, Grella et al., 2014; Matsumoto et al., 2020; Yang et al., 2017; Young et al., 2005).
Arguably, no indicators of the cumulative disadvantage of racial discrimination are more obvious than racial disparities in health and criminal justice system involvement, and these two are intricately connected regarding substance use and misuse. However, when it comes to substance use treatment and prevention, more emphasis has been placed on individual, behavioral, or criminal justice approaches, with little attention to social, structural, and institutional factors that might lead to greater incidence, prevalence, and morbidity of the disease.
7.3. How racism gets under the skin to create vulnerability to substance use
This section focuses on the role of the structural factor of racism in initiation and severity of substance use; as such, it conceptualizes SUDs in a racial health disparities framework. Race and ethnicity are thought to primarily influence health through racism and discrimination. As previously mentioned, racism creates social and economic barriers that lead to an inequitable distribution of resources, which ultimately affects health and health behaviors. Although many studies have focused on perceived discrimination, it should be noted that racial and ethnic discrimination does not have to be perceived to negatively affect well-being (Harrell et al., 2011).
The direct and indirect effects of racism have been linked to higher allostatic load (Ong et al., 2017), accelerated cellular (biological) aging (Geronimus et al., 2010; Rewak et al., 2014), poor birth outcomes for mother and child (Alio et al., 2010; David and Collins, 1997; Turner, 2009), chronic illnesses and mortality (Chae et al., 2015; Jackson et al., 2010; Turner, 2009), and substance use initiation and misuse (Gilbert and Zemore, 2016; Turner, 2009).
The relationship between race and health in general, and substance use in particular, is often modeled through psychosocial stressors and coping channels resulting from cultural, structural, or interpersonal discrimination. This approach posits that racism leads to greater psychological stress, economic barriers, and changes in behavior and psychobiological processes, which could also affect future generations (Brondolo et al., 2009; Mezuk et al., 2010). These models are based on the stress response model, which has been the dominant framework to understand how social factors affect mental health (Turner, 2009). The stress process model links social characteristics to physical, mental, and overall well-being through social stress (Turner, 2009). Nonetheless, the relationship between racism discrimination and health is not always straightforward. For example, even though morbidity and mortality are worse for Black Americans, noninstitutionalized Blacks have been found to have surprisingly lower rates of major mental disorders than non-Hispanic Whites (Mezuk et al., 2013). Although this may seem paradoxical, Jackson and colleagues proposed a stress-coping model that demonstrates that African Americans may engage in unhealthy behaviors such as overeating and substance use to relieve the symptoms of stress in the short run at the expense of their long-run health (Jackson, and Knight, 2006; Jackson et al., 2010).
The environmental affordances model, which builds on the stress-coping framework of Jackson and Knight (2006), uses a transdisciplinary approach to investigate how individual actions relate to environmental resources and circumstances to understand racial gaps in physical and mental health (Mezuk et al., 2013). The benefit of this model is it relates social circumstances, such as residential segregation, which is also affected by systemic racism (Rothstein, 2017), to health behaviors, the social environment, and mental and physical well-being. Moreover, the model explicitly considers the role of race in this relationship by postulating that “the motivation for and availability to engage in poor health behaviors as stress-coping or self-regulation strategies is influenced by social structures and contexts (e.g., poverty, segregation, access to goods) and that these social structures are in turn differentially distributed across racial groups)” (Mezuk et al., 2013, p. 83). Previously discussed is a social concept that developed from phenotypical differences, race in this context is an indicator of experiences, not variations in genetic, epigenetic, or neurobiological factors. The model postulates that environmental circumstances provide stress and affordances (or occasions to relieve stress); that coping behaviors are influenced by cultural, social, and contextual factors; and that all organisms engage in actions to immediately relieve distress from stressful events.
As proposed by Mezuk and colleagues (2013), the social environment can increase contact with chronic stress for marginalized populations and the relationship between environmental circumstances and the variety of health-related coping activities. These coping behaviors can mitigate the negative effects of stress on mental health in the short run but lead to discrepancies in physical health in the long run. These poor health behaviors can mediate the relationship between stress and the occurrence of psychopathology. Furthermore, environmental, social, and economic inequities worsen the effects of these coping strategies on physical well-being. Overall, chronic stress directly and indirectly (through participation in negative health behaviors) can lead to large differences in morbidity and mortality over the life course (Mezuk et al., 2013). Walters et al. (2002) developed a similar “Indigenist” stress-coping model. They model discrimination as a form of traumatic stress and explicitly incorporate historical trauma and unresolved grief into their framework, which are highly relevant to groups such as American Indians, Alaska Natives, and Blacks, who have a deep-rooted history of subjugation and trauma in the United States with insufficient reconciliation and atonement regarding past injustices. Historical trauma, unresolved grief from this historical trauma, and continued discrimination can result in greater substance use through its effect on mental health.
Neurologically, stress activates the HPA axis to release corticotropin-releasing hormone (CRH) from the hypothalamus. This, in turn, causes ACTH to discharge from the pituitary gland, which then travels to the adrenal cortex to cause the secretion of glucocorticoids. These glucocorticoids then travel back to the hypothalamus and pituitary gland to stop the discharge of ACTH and CRH through a negative feedback loop (Charmandari et al., 2005). Chronic stress disrupts the cortisol’s negative feedback, leading to continued secretion of CRH (Charmandari et al., 2005; Jackson et al., 2010). Chronic activation of this system leads to increased anxiety and ultimately, poor mental health outcomes (Marin et al., 2011). Jackson and Knight (2006) hypothesized that negative health behaviors such as substance use or misuse can protect against the negative psychological effects of chronic activation of this system caused by chronic exposure to negative adverse environmental factors and stressors, such as racial and ethnic discrimination. Specifically, this mechanism is triggered through substance use by the release of dopamine and beta-endorphins, which relieve feelings of anxiety and stress while also reinforcing addictive behavior through the reward system in the brain (Volkow et al., 2017). Therefore, although substance use can lessen feelings of stress and anxiety, it also reinforces the behavior as linked to stress relief through its impact on the brain’s reward system (Volkow and Boyle, 2018; Volkow et al., 2016).
Research has found that unhealthy behaviors strengthen the relationship between stress and depression for Whites but attenuate the relationship for Blacks. In other words, Blacks who engage in unhealthy behaviors have a lower likelihood of depression than Blacks who do not (Jackson et al., 2010; Mezuk et al., 2010). Clark (2014) also tested the stress-coping model among Blacks and found that depressive symptoms completely mediated the relationship between perceived discrimination and recent substance use and partially mediated the relationship between perceived discrimination and lifetime substance use. Another study by Gerrard et al. (2012) found that experiencing discrimination led to a greater willingness to initiate substance use and perceived discrimination was positively associated with substance use among Black adolescents and young adults who approve of “substance use-as-coping.” A recent qualitative study of young adults who identify as lesbian, gay, transgender, bisexual, and queer (LGBTQ) found that some LGBTQ youth initiated substance use to cope with stressors such as interpersonal and structural discrimination (Felner et al., 2020). Interestingly, in a group of Asian and Pacific Islander college and graduate students, perceived racism was associated with inferior mental health but not substance use; however, no direct test of the stress-coping framework was conducted (Chia-Chen et al., 2014).
A positive association has also been found between self-reported and perceived racism and discrimination among Black Americans (Borrell et al., 2007), U.S.-born Latinos (Otiniano Verissimo, Gee et al., 2014; Otiniano Verissimo, Grella et al., 2014), Asian Americans (Yoo et al., 2010), and African, South East Asian, and Hispanic immigrants (Tran et al., 2010) and substance use. In addition, perceived discrimination among Hispanics during adolescence and early adulthood is associated with initiation of substance use (Rogers et al., 2020). In a study of LGB adults, those who reported sexual orientation, race, and gender discrimination had four times greater odds of reported SUD in the past year than LGB adults who reported no discrimination (McCabe et al., 2010). More recent research by Glass et al. (2020) found racial and ethnic discrimination was associated with increasing severity of alcohol used disorder along both extensive and intensive margins. In other words, the experience of racial and ethnic discrimination and the number of events experienced were both associated with more severe alcohol use disorder.
Although animal studies have not directly tested the relationship between the social stressor of racism and substance use, studies have investigated the role of social stress, social subordination, and positive social interactions. For example, studies have found that chronic subordination and negative social experiences can lead to increased initiation of substance use and self-medicating (Neisewander et al., 2012). In addition, studies of aggressive social interactions (like racism and discrimination) found greater drug use, relapse, and drug-seeking behaviors among rats and mice with “acute and repeated social defeat exposure” (Logrip et al., 2012; Pelloux et al., 2019). Finally, studies have found benefits of positive social interactions can overcome drug craving in animal subjects (Pelloux et al., 2019; Venniro et al., 2018). These findings suggest that negative social interactions and social oppression stemming from racism are risk factors for substance use initiation and misuse, whereas social inclusion may be protective. Heilig et al. (2016) proposed that the neuroscience addiction model could be made more translational to clinical treatment by explicitly incorporating social exclusion into addiction neuroscience.
The stress-coping model also implies that the environmental effects of racial and ethnic discrimination (e.g., greater access to negative coping mechanisms, such as via alcohol and illicit drugs, and limited access to resources that encourage healthy behaviors, such as parks and gyms), make it more likely for minorities to use coping strategies to manage chronic stress through choices that offer immediate relief (such as substance use initiation or abuse). For example, low-income Black neighborhoods tend to have higher concentrations of liquor stores and other alcohol outlets, and this higher concentration has been associated with greater susceptibility of risky alcohol use among Black drinkers (Theall et al., 2011). Animal research on rats and primates has also found that availability of substances affects use (Heilig et al., 2016; Nader and Banks, 2014).
7.4. Institutional racism example: Criminal justice system, racism, and substance use
Of particular importance to this discussion on racial and ethnic discrimination and health is an understanding of the role of institutional racism and its negative effect on health and health behaviors. The United States has the dubious distinction of having the highest imprisonment rate (655 per 100,000) in the world (International Center for Prison Studies, 2018), accompanied by disproportionate representation of incarcerated minorities (Alexander, 2012; Center on Addiction and Substance Use [CASA], 2010), high proportion of incarcerated individuals with SUDs, and little capacity to provide SUD treatment (Alexander, 2012; CASA, 2010; Nowotny, 2015). Minorities have disproportionately greater exposure to the criminal justice system in general and incarceration in particular (Bonczar, 2003; Hinton, 2016; Wildeman and Wang, 2017), resulting in severe health outcomes at the individual, family, and community levels (Lorvick et al., 2018; Wildeman and Wang, 2017). Structural racism has a long history of manifestations via institutional policies, including criminal justice policies (Bailey et al., 2017; Hinton et al., 2018). Relatedly, policy changes in the last four decades, not increases in criminal behavior, have led to the expansion of the carceral state and extensive reach of the criminal justice system in the lives of low-income and marginalized communities (Alexander, 2012; Raphael and Stoll, 2013). Included in these policies is the War on Drugs, which not only treated substance use as a crime instead of an illness, but also targeted drugs used by minorities and widened the net of the criminal justice system, thereby increasing racial disparities in this system (Cox and Cunningham, 2021). These disparities partially stem from government policies that disproportionately target communities of color. For instance, intergovernmental grant programs, together with U.S. Supreme Court decisions authorizing police with extraordinary powers to stop and search residents with minimal to no probable cause, often in the name of drug policy, have contributed to the disproportionate policing and imprisonment of people of color (Alexander, 2012; Benson and Rasmussen, 1996; Blumenson and Nilsen, 1998; Cox and Cunningham, 2021; Holcomb et al., 2018; Russell, 1998; Sandy, 2002; Tieger, 1971).
Given the impact of criminal justice policies on minority communities and their direct and indirect effects on health, it is not possible to discuss racial health disparities without considering the impact of the criminal justice system on the health outcomes of minorities in general and substance use in particular. Moreover, given the indirect negative effects of concentrated incarceration on families and communities, it is necessary to take an intergenerational life course approach to understand how these policies might affect outcomes of certain communities across time and space, including substance use initiation and abuse.
The criminal justice system plays a central role in the lives of marginalized communities of color and is an important component of the racism these communities experience (Kwate and Goodman, 2015). At every level of the criminal justice system, racial disparities and biases are present (Alexander, 2012; Bailey et al., 2017; Cox, 2020; Hinton et al., 2018; Wildeman and Wang, 2017). Criminal justice system contact has been associated with diminished mental health in general (Sugie and Turney, 2017) and increased emotional distress, anxiety, trauma, and posttraumatic stress disorder in particular (Geller et al., 2014; Hirschtick et al., 2020; Jackson et al., 2019). Contact with the criminal justice system has also been associated with mental distress of communities and family members and is a regular occurrence in communities of color (Bor et al., 2018; DeVylder et al., 2018; Lee et al., 2014; Naser and Visher, 2006; Wildeman et al., 2012), which could contribute to intergenerational transmission of substance use and SUDs. Because minorities have disproportionately higher contact with this system, they are also more likely to experience health consequences resulting from the additional stress of being marked with a criminal record, the stigma of incarceration, or having a family member incarcerated (see Cox, 2018). Although drug use is common in the incarcerated population, there is reverse causality in this relationship. That is, drug use can lead to incarceration. Conversely, the negative aforementioned direct psychosocial effects of incarceration and the indirect effects of the mark of a criminal record and incarceration after release can also limit the ability to be a productive, law-abiding citizen, which can contribute to substance use initiation, disorder, and relapse. Although there is scant longitudinal research investigating the effect of incarceration on substance use, Genberg et al. (2015) found that the odds of injection drug use among people who had stopped injecting drugs prior to their incarceration increased after their release. Mowen and Visher (2015) reported that family conflict during incarceration is associated with substance use. To the extent that incarceration places additional strain on family relationships, it is another mechanism through which incarceration can affect drug use. Other research has found social support (e.g., supportive parenting) can protect against chronic stress, such as racism (Gibbons et al., 2010). Animal models have also demonstrated the importance of social engagement and support. For example, in a review by Neisewander et al. (2012), negative social experiences in general, and chronic social subordination in particular, increased vulnerability to drug use and abuse. This means we should expect greater substance use in the incarcerated population in general, with larger effects among racial minorities dealing with the intersectionality of their race and criminal status. Given that stress may differentially promote initiation and relapse of substance use among women (Torres and O’Dell, 2016), this may be especially true for incarcerated women, who are disproportionately racial and ethnic minorities and typically more disadvantaged than men (Cox, 2012).
7.5. Racism and discrimination in SUD treatment
Although there is a dearth of quantitative studies on perceived discrimination or personal experiences of discrimination stemming from the SUD treatment system, evidence of stigma and discrimination of people with SUDs (Tsai et al., 2019) and inequities in SUD treatment access and outcomes has been documented. Studies using data from large SUD treatment systems have revealed that Black and Latino clients wait longer to be admitted to treatment and are less likely to receive the services they need and complete a course of treatment (Guerrero et al., 2013; Marsh et al., 2009; Mennis et al., 2019). In part, these differences are associated with program characteristics such as lack of Medicaid payment acceptance and culturally and linguistically appropriate services (Guerrero et al., 2017). In the criminal justice system, disparities have also been noted wherein incarcerated Blacks and Hispanics with SUD are less likely to receive evidence-based treatment compared to their White counterparts (CASA, 2010). Although more detailed studies of incarcerated populations (e.g., Nowotny, 2015) found no Black–White disparities in utilization of SUD treatment during incarceration, they found that Hispanics were significantly less likely to utilize such treatment and that overall treatment access, especially to evidence-based treatment, was extremely low. However, a study in California documented racial and ethnic disparities in diversion to SUD treatment in lieu of incarceration and noted that Whites are more likely to receive such diversion compared to Blacks and Latinos (Nicosia et al., 2013). Moreover, Whites are more likely to have access to community-based treatment and co-occurring disorder treatment than minorities (Hedden et al., 2021). Due to the overwhelming prevalence of SUDs among incarcerated populations (64.5%; CASA, 2010) and the significant overrepresentation of minorities in incarcerated populations, lack of SUD treatment for incarcerated populations has a further disproportionate impact on racial and ethnic disparities in SUD treatment access. Despite evidence that SUD treatment for incarcerated populations is efficacious and cost-effective (Wakeman and Rich, 2015), stigma related to addiction and prevailing attitudes favoring punishment versus rehabilitation among policy makers contribute to the lack of systemic implementation of SUD treatment and related services in the criminal justice system (CASA, 2010).
Other research on hospitalized patients with SUDs has documented that such patients often experience stigma and discrimination from health care providers and other hospital staff members (Biancarelli et al., 2019; Horner et al., 2019; McNeil et al., 2014; Simon et al., 2019). Prompted by the pressing need to increase service capacity due to the opioid epidemic, a recent qualitative study (Priest et al., 2020) of board-certified or board-eligible addiction physicians from 16 U.S. acute care hospitals sought to identify major barriers and facilitators of development and administration of addiction consultation services. They found that stigma and discrimination of drug users and SUD treatment among hospital health personnel and administrators was a critical barrier to the development and operations of such services.
In summary, racism and discrimination and its various institutional, cultural, and interpersonal forms result in significant threats to well-being. As such, it is critical to consider social factors related to vulnerability to substance use. Emerging data from animal studies provide relevant findings suggesting that factors related to racism and discrimination, such as social subordination and exposure to aggressive social interactions, create vulnerability to substance use. Epidemiological and social science studies have documented the harmful health and other effects of exposure to racism and discrimination. Less is known about how exposure to racism and discrimination interacts with other stressors and adversities to influence substance use vulnerability.
8. Limitations and promising areas for future directions
Although significant scientific progress has taken place in the basic and social sciences regarding the role of stressors, environmentally toxic social contexts, and racism and discrimination in substance use vulnerability, limitations and gaps require further investigation. Next, we highlight some of those limitations and promising areas for future research.
8.1. Increased research focus on community and societal factors that affect social vulnerability to substance use at the individual and community levels of influence
Although substantial gains have been made in recent decades in understanding how stress and development interact to create vulnerability to substance use, research that expands on the study of vulnerabilities is needed. Most approaches to date have focused on mitigating individual-level factors, whereas less has been done to investigate community and societal factors that may interact to directly and indirectly affect youth’s exposure to adversity (Lorenc, 2020). Nor have they included aspects of urban neighborhood context, including overpolicing and environmental pollutants, or experiences driven by low income, such as food insecurity, eviction, overcrowded housing, juvenile justice contact, homelessness, and household stressors of single parents with weak support networks (Wade et al., 2016). Future research that measures a wider range of factors associated with socially toxic environments in childhood is needed to provide a comprehensive understanding of how social determinants of health directly and indirectly influence the association between such exposure and substance abuse. By doing so, the scientific community will produce more sensitive and representative indicators of childhood adversity that more accurately gauge its social distribution in and across populations and communities. This knowledge can lead to the development of more upstream social or community-level policy actions and interventions that address socially toxic environments among children and families, reduce structural risk factors, and strengthen social supports (McEwen and Gregerson, 2019).
8.2. Longitudinal studies of social vulnerability, brain development, and substance use trajectories
As noted in recent national consensus reports (NASEM, 2019a, 2019b, 2020), more longitudinal studies on brain development are needed (Jernigan et al., 2018; Lisdahl et al., 2018). This includes studies assessing if and how alcohol and drug use results in adaptations to the stress response system or exacerbates pre-existing stress dysregulation (Wemm and Sinha, 2019). Data from recent large longitudinal studies, combined with previous work from retrospective analyses of the early life experiences of adults, are providing new opportunities to examine normal brain development and cognitive trajectories from childhood to young adulthood and how these are shaped by biological, psychological, and social and physical environmental factors. An overarching aim is to identify how these factors influence vulnerabilities to SUD. One such initiative is the Adolescent Brain Cognitive Development (ABCD) Study (ABCD Research Consortium, 2020). Funded by multiple institutes at the National Institutes of Health, it is the largest longitudinal study of brain development and child health in the United States. It is currently following the biological and behavioral trajectories of nearly 12,000 children for 10 years beginning at ages 9–10 through adolescence into early adulthood. The study aims to track exposure to substance use and how this may affect developing brain structure and function in terms of mental health and cognitive abilities. In addition to brain imaging and biospecimen collection for genetic and epigenetic analyses, the ABCD Study protocol consists of standardized and harmonized assessments of neurocognition, physical and mental health, social and emotional functions, and culture and environment. The ABCD Study will provide an unprecedented opportunity to examine how factors across multiple domains (i.e., biological, behavioral, sociocultural) and levels of influence (i.e., individual, interpersonal, community) interact across developmental stages to affect substance use trajectories among youth (Jernigan et al., 2018; Zucker et al., 2018). The design and methodology of the ABCD Study holds unparalleled promise for advancing science regarding the role of social vulnerability to substance use and related health conditions. This includes sufficient sampling of various racial and ethnic groups to allow detailed analyses and sound psychometric scales for measuring exposure to socially toxic environments, including discrimination and racism; protective, risk, and cultural factors; and numerous biological measures.
The HEALthy Brain and Child Development (HBCD) Study is another ongoing 10-year longitudinal study similar to the ABCD Study but that aims to assess brain development from infancy into preadolescence. Specifically, the HBCD Study will establish a large cohort of pregnant women across various regions of the United States who have been substantially affected by the opioid crisis and follow these women and their children for at least 10 years. Study findings are expected to provide researchers with a greater understanding of normal brain development in childhood and the long-term impacts of prenatal and postnatal opioid, other drug, and environmental exposures (National Institutes of Health, 2020). Data from the ABCD and HBCD studies can be used to inform interventions at all levels of influence that can reduce exposure to toxic environments and mitigate their impacts on substance use vulnerability.
Both studies have an open science model that makes the data freely available through an open access platform to the broad research community. This ensures that the data can be used to answer a broad range of research questions and facilitates collaboration between behavioral and basic scientists to gain a better understanding of the mechanisms involving social factors and their interaction with biology.
8.3. Development and implementation of population-level upstream prevention approaches
The literature on prevention of substance use has largely focused on downstream approaches (i.e., individual, family, and school-level substance use prevention interventions), many of which address social factors that contribute to substance use vulnerability. However, akin to the public health parable and case study presented earlier, population-level strategies are needed to address upstream root and fundamental causes that create conditions of adversity and social vulnerability (NASEM, 2017). A recently published report by NASEM (2019a) supports our call for upstream approaches to improving child health and advancing health equity in children that can substantially lead to the reduction of socially toxic childhood environments. The report’s recommendations include support from policy makers at the federal, state, local, and tribal levels and philanthropic organizations to (1) develop interventions that are culturally sensitive and tailored to meet the needs of vulnerable children, including those living in chronic poverty and from immigrant backgrounds; (2) reform the content of prenatal, postpartum, and pediatric care to ensure ongoing access to quality health care; (3) have public housing authorities increase the supply of high-quality affordable housing available to families, especially those with young children; and (4) expand access to comprehensive, high-quality, and affordable ECE programs across multiple settings to all eligible children, prioritizing those from vulnerable and underserved populations (NASEM, 2019a).
Without population-level strategies that address root causes, we will forever be swimming against the tide of impacts underlying social vulnerability. Agent-based modeling has recently been applied in public health (Tracy et al., 2018) and holds promise for increased understanding of population-level health outcomes, such as substance use. Although not free of limitations, this approach could be useful “for visualizing, analyzing, and informing complex dynamic systems” (Tracy et al., 2018, p. 78), such as substance use vulnerability, at the population level and modeling potential benefits of interventions under varied scenarios. Agent-based models have proven useful, for example, in assessing disease endpoints at the population level, risk behaviors, and policy impacts and in social epidemiological research and studies on the mechanisms through which upstream social factors contribute to health and disparities (Tracy et al., 2018).
8.4. Advancement of theoretical models and methods in animal models and human research on upstream social factors
Venniro and colleagues (2018) aptly identified a current limitation of current neuroscience research stemming from not incorporating volitional social factors, which play a critical role in human addiction—thereby limiting translation of animal research to prevention and treatment in humans. Future neuroscientific studies may consider how to incorporate volitional social factors that mimic real-world interactions in communities and how these social factors influence neurobiological mechanisms of substance use, addiction, craving, and relapse.
In addition, a neurobiological model of racism and discrimination suggests that ongoing experiences of discrimination result in impaired function of the HPA axis and prefrontal cortex, similar to impairments seen in cases of chronic stress and heightened prolonged stress reactivity, which may ultimately lead to an increased risk of negative mental health outcomes (Berger and Sarnyai, 2015). For this reason, it is imperative to consider discrimination as an acute or chronic psychosocial stressor, and more effort should be directed toward the development of a useful neurobiological framework for understanding its damaging effects on physical and mental health (Busse et al., 2017). Moreover, research is needed to understand how the type of social exclusion generated by racism and discrimination affects neurobiology and substance use.
Similarly, research is needed on how racism and discrimination act across all levels of influence associated with individual, environmental, and structural determinants of substance use and SUDs (individual, interpersonal, community, and societal). And interventions at all these levels need to be developed and tested to identify efficacious strategies to reduce exposure and mitigate impacts of racism and discrimination on health, including substance use.
8.5. Improving treatment availability, access, and outcomes
We have stressed the role of social determinants of health in exposure to factors that increase vulnerability to substance use and called for research on upstream factors and upstream interventions at the population level. However, as in the public health parable and case study presented, there is also a need to advance scientific understanding that leads to more efficacious approaches for those already affected by SUD. Although SUD treatment could be improved in many ways, the most immediate is to test and implement strategies that enable expansion of the SUD treatment capacity and reach with efficacious approaches. This includes access to efficacious treatment in the community, in the criminal justice system, and for all population groups. Treatment itself can be an important aspect of prevention, because parental SUDs are a major risk factor for children.
8.6. Summary
This review provided evidence that socially based stressors play a critical role in creating vulnerability to substance use and as such, deserve greater empirical attention to further our understanding of how they get under the skin. We focused attention on the role of stressors, particularly early and ongoing exposure to socially toxic childhood environments, and racism and discrimination as foundational social factors in the psychobiological cascade that creates vulnerability to substance use and its consequences. Using a top-down approach, we brought attention to some known yet often unexplored relationships between vulnerability to substance use and SUDs and understudied inequities and their potential differential effects across minority populations. Finally, research gaps and promising areas of research, practice, and policy focused on ameliorating social vulnerabilities associated with substance use and SUD across the lifespan were presented. These future efforts can take the form of enhanced interdisciplinary approaches that consider biological and social factors that interact across multiple levels to influence vulnerability to substance use at the individual and population levels.