Abstract
PTSD is characterized by difficulties in accurately evaluating the threat value of sensory stimuli. While the role of canonical fear and threat neural circuitry in this ability has been well studied, recent lines of evidence suggest a need to include more emphasis on sensory processing in the conceptualization of PTSD symptomology. Specifically, studies have demonstrated a strong association between variability in sensory processing regions and the severity of PTSD symptoms. In this review, we summarize recent findings that underscore the importance of sensory processing in PTSD, in addition to the structural and functional characteristics of associated sensory brain regions. First, we discuss the link between PTSD and various behavioral aspects of sensory processing. This is followed by a discussion of recent findings that link PTSD to variability in the structure of both gray and white matter in sensory brain regions. We then delve into how brain activity (measured with task-based and spontaneous functional imaging) in sensory regions informs our understanding of PTSD symptomology.
Introduction
Dysfunction in distinguishing between threatening vs non-threatening stimuli is a central theme in both the symptoms and our mechanistic understanding of Post-traumatic Stress Disorder (PTSD). Evaluating potentially trauma-relevant stimuli depends upon the ability to detect and perceive sensory inputs. This detection and perception involves a balance between internally and externally driven sensory information and its perceived threat to the individual [1]. Trauma exposure and subsequent development of PTSD involves an interplay between circuits for the sensorial experience and emotional appraisal of stimuli. Yet, while the contribution of threat circuitry is well appreciated, integrating sensory processing into neurobiological models of the disorder has received much less focus.
Recent work suggests that sensory circuits may be highly relevant to our understanding of risk vs. resilience following trauma exposure [2], as well as in distinguishing phenomenological presentations of PTSD such as ‘intrusion’ symptoms (e.g. – flashbacks) [3]. Intrusive symptoms and flashbacks incorporate an explicit memory component with a strong sensorial component (e.g., vividly “seeing” the trauma occur again) that elicits intense physiological reactions [1,3]. These symptoms can further become more frequent when the trauma memory is overgeneralized to non-trauma related contexts. Thus, understanding the role of sensory processing in PTSD is of crucial importance for ameliorating the sensory disturbances prevalent in the disorder.
A question that is crucial to this understanding is how variability in sensory processing, as well as the structural and functional characteristics of sensory brain regions, is linked to overall PTSD severity. Importantly, there is a fundamental need to distinguish between the variability in these features that result from PTSD itself versus those that represent risk factors for the later development of PTSD. Such an understanding has great potential to aid not only in PTSD intervention [1,4], but also has potential implications for sensory processing dysfunction in a variety of psychiatric disorders [4,5]. In the current review, we discuss recent developments in the important role of sensory processing and PTSD. We highlight recent findings showing altered sensory processing linked to PTSD and recent evidence of structural and functional brain variability associated with PTSD. We also discuss some of the latest developments in therapies for PTSD based on knowledge of sensory processing in PTSD.
Altered sensory processing and PTSD
PTSD has been linked to various deficits in sensory processing [4,6–9]. Sensory modulation, the act of increasing or decreasing activity in sensory cortex in response to stimuli, may underlie alterations to processing in specific sensory modalities including vision [6,7,10], audition [11,12], somatosensory function [13,14], and olfaction [15,16]. In PTSD, deficits in sensory modulation may cause the over/under-responsivity of sensory cortex in the presence of stimuli and may lead to symptoms such as hyperarousal states [8] or dissociative phenotypes in the form of hypo-reactivity to triggering stimuli [4]. The work done in this area has demonstrated that PTSD is associated with deficits in the processing of both emotional and non-emotional sensory stimuli [6–8].
It is well known that PTSD causes deficits in the ability to appropriately process the emotional dimensions of sensory stimuli. Other work has shown that PTSD is associated with alterations in individuals’ ability to evaluate both pleasant and aversive emotional visual stimuli [10]. Shalev and colleagues found that discrimination between neutral stimuli was impaired after those stimuli had been associated with an aversive visual stimulus [7]. Other work by Marlatte and colleagues has shown that PTSD is associated with non-emotional visual processes such as imaging spatially coherent scenes and spatial navigation through complex environments [6]. Recent work has also found evidence of sensory processing dysfunction associated with trauma early in life. For example, children exposed to continuous traumatic stress have altered sensory modulation patterns and subsequent deficits in general sensory processing independent of emotional context [8]. Still, the neurobiological underpinnings of these deficits are not fully understood.
Recent studies of brain structure and function have led to new understanding of potential mechanisms for sensory processing deficits associated with PTSD. For example, the aforementioned work by Marlatte and colleagues, identified structural features that were directly associated with PTSD-related dysfunction in non-emotional sensory processing [6]. Notably, they found that spatial processing and integration was related to white matter fiber density in tracts connecting core memory regions (e.g. – hippocampus and thalamus) with higher-order visual regions like the precuneus. Other recent work has identified potential functional mechanisms for sensory processing deficits in PTSD. Work in combat veterans shows that sensory processing dysfunction in PTSD may be related to altered synchronization of alpha activity, brain activity measured from EEG in the 8–12 Hz range, that may be involved in regulating sensory inhibition [9]. The oscillations in the alpha range are particularly important due to their observed role in gating bottom-up input between sensory cortex and frontal regions. Evidence from this work suggests that dysfunctions in the regulation of alpha connectivity in PTSD, may lead to an inability to inhibit sensory cortex, which may underlie the overactivation of sensory representation during the re-experiencing of trauma.
While these findings provide potential insight into the mechanistic underpinnings of sensory processing dysfunction in PTSD, a great deal remains yet to be understood. The fact that PTSD is associated with deficits in the sensory processing of both emotional and non-emotional stimuli raises several interesting possibilities. First, these findings may indicate the presence of a universal predisposition that may exist well before trauma exposure. In other words, it may be that individuals with pre-existing alterations in sensory processing may be more susceptible to developing PTSD-related sensory dysfunction. However, it should be noted that traits like sensory processing sensitivity (SPS) have been associated with neural patterns that are distinct from those associated with hyperarousal in PTSD [4]. If this is indeed the case, it raises the question of whether there is a causal role of trauma exposure in combination with some regions involved in fear circuitry (e.g. - PFC, amygdala, hippocampus, etc.) that explain sensory hyperarousal in PTSD [17]. One way to further uncover knowledge in this area is to examine how variability in key brain features relate to PTSD symptomology. The next sections describe these associations in more detail, focusing specifically on the relationship between PTSD and the features of brain structure, brain activity, and functional connectivity.
Neural structure of sensory cortex in PTSD
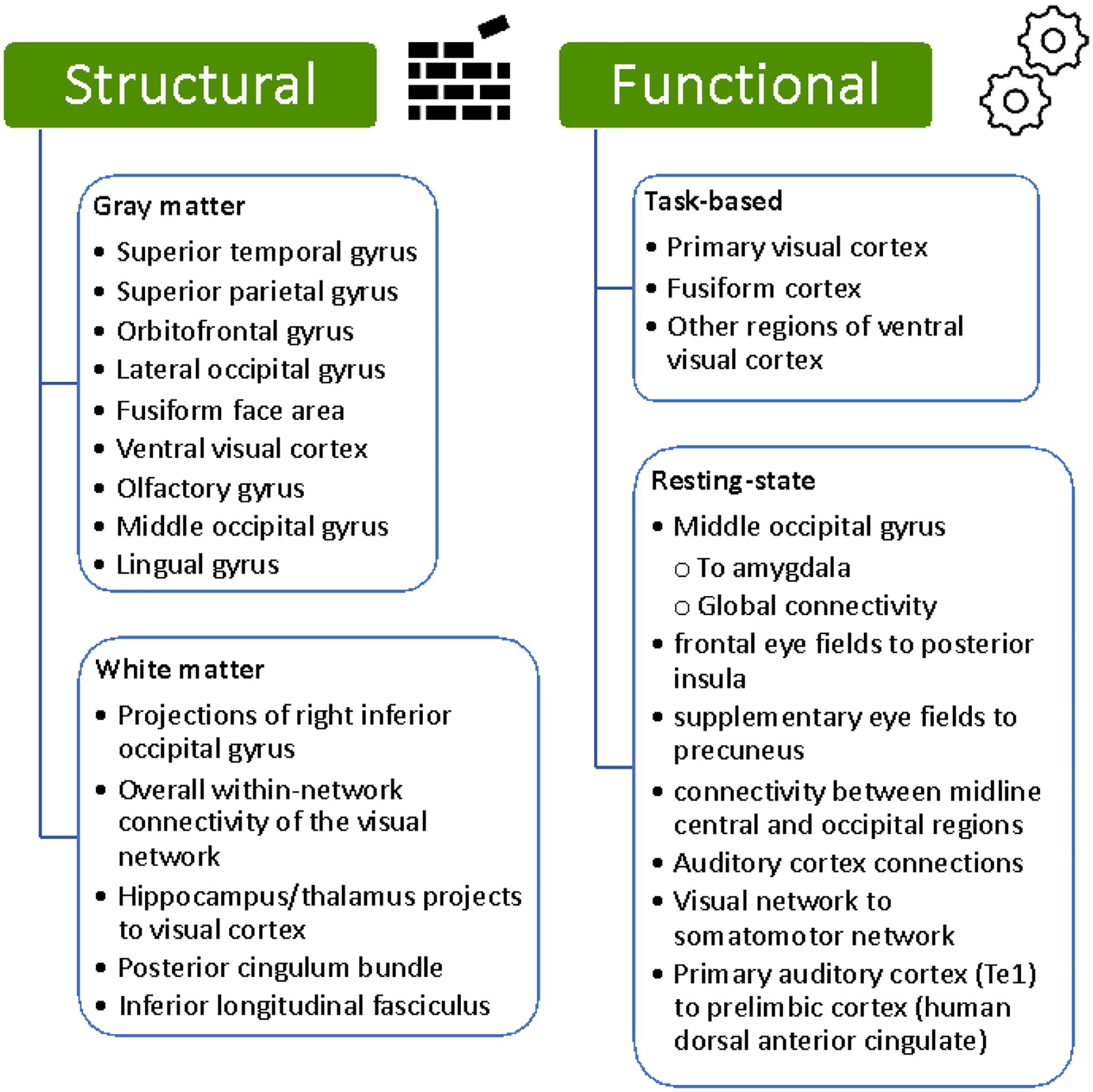
An increasing amount of evidence demonstrates an association between PTSD and the structural features of sensory cortex. Work in animals has previously linked changes in cortical structure to severe psychological stress [18]. Evidence has also been uncovered from human studies. For example, mega-analysis performed by Wang and colleagues showed that greater severity of intrusive memories was associated with lower gray matter volume (GMV) in temporal, parietal, and occipital regions [19]. These regions included the superior temporal gyrus, which helps integrate audiovisual information from emotional stimuli [20], the superior parietal gyrus (SPG) involved in dorsal visual processing stream for spatial and movement information [21] and bilateral orbitofrontal gyrus (OFG), involved in guiding sensory attention and integrating inputs from sensory and limbic structures [22]. Other studies have found decreased average cortical thickness in visual cortex associated with PTSD, with cortical thickness in the lateral occipital gyrus being lower in individuals with PTSD compared to controls [23].
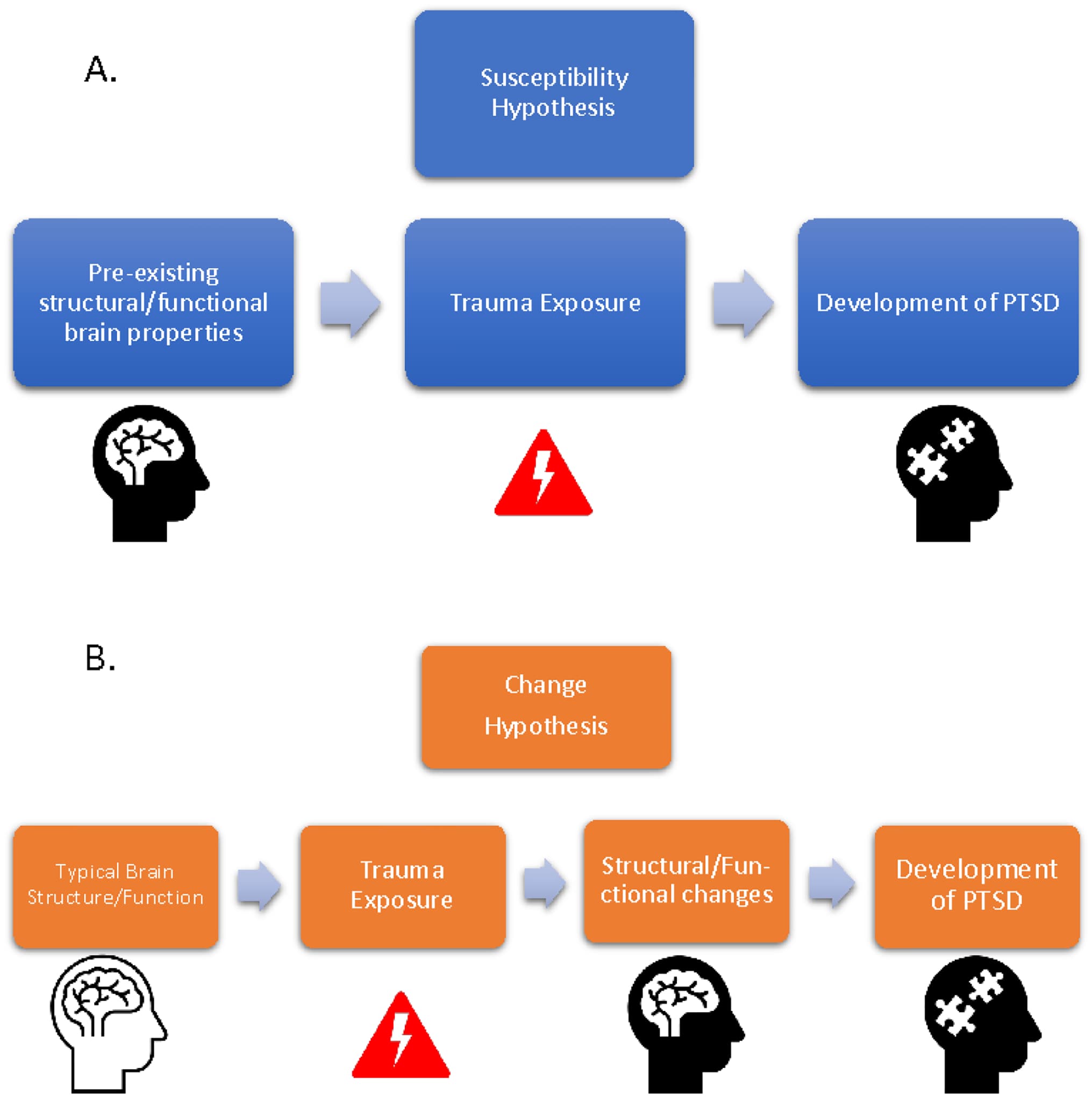
Although patient-control comparisons of cortical structure between PTSD patients and non-trauma exposed individuals are important, insight can also be gained from examining how variability in cortical structure among PTSD patients leads to differential symptomology. This helps address the major question of whether the structural properties of sensory cortex associated with PTSD represent pre-trauma susceptibility vs. changes acquired in response to and following trauma exposure (Fig. 1). For example, PTSD patients with greater avoidance behaviors show greater cortical thickness in middle/lateral occipital cortex [24]. Other investigations have probed the timing of structural changes in sensory cortex in earlier phases immediately preceding the development of PTSD symptomology. For example, some insight has been gained from studying individuals with Acute Stress Disorder (ASD) [25]. ASD is characterized by PTSD-like symptomology in the immediate aftermath (up to the first month) of exposure to trauma and serves as a predictor of the later development of full-fledged PTSD. Individuals with ASD show lower GMV in temporal and occipital regions that is associated with PTSD symptom severity and symptom clusters 4 weeks later. Work from members of our own group shows significant associations between acute posttraumatic symptoms and the structure of gray and white matter in visual regions including fusiform face area, and other regions in the ventral stream [26]. Variability in these structures exhibited a curvilinear relationship with acute posttraumatic stress severity and the change in PTSD symptom severity from 1 to 12 months. Together, these findings demonstrate the importance of continued investigation of sensory cortical variability in relation to the chronological development of PTSD symptomology.
Several other studies have also identified alterations to the integrity of white matter tracts that connect sensory cortex to the rest of the brain [6,27–29]. Connections for the right inferior occipital gyrus show a more central role (i.e. - nodal centrality) in PTSD patients as well as increased overall within-network connectivity in the visual network. Additionally, recent work has shown a relationship between PTSD and white matter integrity in pathways connecting the hippocampus and thalamus with later visual regions like the precuneus [6]. Increased fractional anisotropy has also been observed in PTSD patients in the posterior cingulum bundle [27], a pathway connecting visual areas to the medial temporal lobe. However, other connections linking the temporal lobe with occipital cortex, like the inferior longitudinal fasciculus, have shown decreased structural integrity [29]. Together, these findings suggest that not all temporo-occipital connections may be altered in the same way with PTSD.
Newer approaches have also begun to emerge for studying the relationship between PTSD and brain structure in sensory cortex. For example, individual network construction based on covariance of gray matter morphology is a method that allows for the evaluation of brain networks based on T1-weighted images alone. Using this method, changes have been observed in regions of sensory networks, including the olfactory gyrus, superior and inferior occipital gyri, and middle occipital gyrus [30]. Other studies have also used gray matter structural networks to identify changes in occipital cortex, specifically in the lingual gyrus, associated with PTSD. The aforementioned work by our own group used similar approaches based on white matter diffusion data to identify variability in the structure of sensory regions that associate with PTSD [26]. The development of additional multimodal and other powerful integrative statistical methods for investigating associations between PTSD and brain structure variability will continue to be an important area for future research.
In addition to measures of cortical thickness/volume and white matter structure, another interesting measure receiving more attention that has been linked to PTSD susceptibility is cortical gyrification - a measure of the folding and patterning of the brain gyri and sulci. Functionally, these patterns of cortical folding enable the efficient wiring of local neuronal connections. In PTSD patients, relative to trauma-exposed controls, cortical gyrification was higher in regions of occipital cortex [31]. This finding suggests that cortical gyrification in occipital cortex may serve as a risk factor for the later development of PTSD following exposure to trauma.
These findings suggest that the link between brain structure and PTSD symptoms may underlie many of the subsequent changes in sensory processing that occur in individuals with PTSD (Fig. 1). However, exactly how these changes in brain morphology translate to changes in behavior remains to be understood. One potential avenue of exploration to provide further clarity is the understanding of brain activity changes following the development of PTSD.
Brain activity and PTSD
Task-based brain activity
Studying brain activity in individuals with post-traumatic stress disorder (PTSD) provides valuable insights into the underlying mechanisms associated with the condition (Fig. 2). For example, individuals with trauma exposure and/or PTSD have shown lower activity in visual cortex when examining positive visual stimuli [32], and reduced activation in secondary visual areas in response to negative visual stimuli [33]. The similarity in modulation for positive and negative stimuli matches work in individuals with anxiety and mood disorders without PTSD, where activity in visual cortex elicited by unpleasant stimuli is not significantly different from when viewing neutral stimuli [34]. This is in contrast to healthy individuals, in whom greater activity in early visual cortex is observed when viewing aversive compared to scrambled visual stimuli [7].
These findings match prior findings that PTSD patients exhibit difficulty with distinguishing between threatening and non-threatening stimuli [33,35]. It is also consistent with other work showing that PTSD symptoms are associated with habituation of activity in visual cortex in response to the repeated presentation of fearful face stimuli [36]). While structures in canonical fear circuitry (i.e. – the amygdala, prefrontal cortex, hippocampus, etc.) show altered patterns of activity in PTSD, the differential modulation of sensory cortex in healthy individuals that becomes less distinguishable with greater trauma exposure and PTSD, further suggests a top-down influence on sensory cortex that is mediated by subcortical and frontal regions [36].
Functional connectivity
Resting-state brain activity has also helped to inform current understanding of the neurobiology of PTSD. For example, PTSD with and without dissociation can be distinguished using the resting activity of somatosensory and motor regions [37]. Functional connectivity, or the correlation in spontaneous brain activity between regions, has also been a useful metric for understanding sensory cortex in PTSD. Notably, many recent studies have similar lines of corroborating evidence for the importance of the middle occipital gyrus (MOG) in PTSD symptomology. For example, PTSD patients show lower connectivity between the MOG and amygdala [38], in addition to altered global patterns of connectivity stemming from MOG [39,40]. This evidence bolsters the importance of not only cortico-limbic connectivity in PTSD, but also cortico-cortical connections that link sensory structures to other cortical regions including posterior cingulate cortex [41] and premotor cortex [42]. Additionally, these findings are supported by recent evidence showing reduced activity in middle occipital cortex when examining positive visual stimuli [32].
Additionally, regions involved in visual processing outside of occipital cortex, such as the frontal eye fields (FEF) and supplementary eye fields (SEF), may be involved in aspects of PTSD. Specifically, recent work suggests that functional connectivity of these areas may be related to the retrieval of trauma memories. Along these lines, Harricharan and colleagues found that PTSD patients show lower connectivity between FEF and posterior insula, SEF and precuneus [43]. These findings suggest that eye movements, or more globally – top-down control over sensory processing in PTSD, may be a potential avenue for the development of future therapies. Furthermore, the current psychotherapy approach of eye movement desensitization and reprocessing (EMDR), which is thought to primarily have efficacy through supporting emotion stabilization during exposure therapy, may also have important effects in sensory networks, which has not yet been explored in detail through a sensory neuroscience lens.
New approaches that build upon the concepts of functional connectivity have also been used to identify changes in sensory processing regions that associate with PTSD [44]. One relatively new method is meta-analytic co-activation modeling (MACM). Although slightly different from pure functional connectivity, MACM is an approach that uses meta-analysis as a means to derive functional connectivity. Using this approach, Pankey and colleagues were able to identify altered patterns of connectivity in visual processing regions that were associated with PTSD [44].
Recent work has shown that resting-state functional connectivity in sensory regions may be a helpful tool in evaluating the effectiveness of novel therapies for PTSD. For example, Zandvakili and colleagues found that after treatment with theta-burst transcranial magnetic stimulation, PTSD patients exhibited increased EEG-based functional connectivity between midline central and occipital regions [45]. In a study of youth with PTSD, functional connectivity in auditory cortex was able to predict individual responses to trauma-focused psychotherapy with up to 76% accuracy [11]. This investigation also saw increased connectivity between regions of the parietal network and the sensorimotor network. Similarly, Korgaonkar and colleagues found that functional connectivity of brain regions in the visual and somatomotor networks was related to better treatment outcomes in PTSD patients who were responsive to trauma-focused psychotherapy treatment [46].
A great deal of focus in studies of functional connectivity and PTSD has been placed on static functional connectivity, or the average functional coupling of activity between brain regions over a given time. However, additional insight has also been gained from the study of dynamic functional connectivity, which probes how functional coupling changes dynamically from moment to moment. For example, Wen and colleagues found that PTSD patients exhibited abnormal patterns of dynamic functional connectivity, specifically within regions of the visual network [47]. In addition to studies of static and dynamic functional connectivity during rest, work in task-based functional connectivity has also identified changes associated with PTSD. In a study of trauma-exposed Black women, performed in conjunction with members of our research group, negative affect symptoms in trauma-exposed individuals were associated with lower functional coupling between occipital cortex and amygdala in task-based functional connectivity [48]. This coupling, observed during a valence-rating task of emotional pictures, points towards the functional relevance of altered functional connectivity observed in PTSD patients.
Animal studies have also suggested the potential importance of functional coupling between sensory cortex and non-sensory brain regions [12,49,50]. For example, Concina and colleagues found that synchronization between primary auditory cortex (Te1) and prelimbic cortex (thought to be somewhat homologous to human dACC) plays an important role in fear discrimination [12]. Notably, the authors found that communication between prefrontal and limbic structures alone was not sufficient for fear discrimination. This finding again highlights the importance of studying cortico-cortical connectivity between sensory and prelimbic structures, in addition to connections between limbic and paralimbic structures, to fully understand their role in fear generalization and discrimination in PTSD. Other work has examined the question of whether functional coupling between sensory and non-sensory regions represents changes vs. susceptibility. For example, in a rat model of PTSD, resilience to trauma was shown to be associated with pre-trauma functional connectivity between limbic structures and regions involved in olfaction, vision, and audition [50]. Together, this work highlights potential targets for manipulating brain activity that may relate to sensory processing dysfunction in PTSD.
Developments in sensory cortex based therapies for PTSD
In addition to investigating functional and structural alterations associated with PTSD, recent work has also shown ways in which sensory cortex can be targeted to help relieve symptoms of PTSD. For example, work using repetitive transcranial magnetic stimulation (rTMS) to target activity in visual cortex has proven to be effective in relieving intrusive memories in PTSD. Herz and colleagues found that treating early visual cortex with inhibitory 1 Hz repetitive rTMS reduced the emotional intensity of intrusive memories [51]. The frequency of intrusions and the explicit visual memories themselves, however, remained intact. The finding that emotional intensity has strong clinical implications, but also contributes to fundamental knowledge about the role of early visual cortex in PTSD symptomology. This finding is consistent with evidence from the perceptual learning literature in which stimulation of early visual cortex inhibits previously learned, perceptual memory of non-emotional visual stimuli [52]. Recent work has also pinned virtual reality as a potential avenue of therapy for PTSD symptoms [53]. Such technology could potentially allow for exposure therapy with sensory stimuli in the absence of threat in a way that diminishes previously learned negative responses to stimuli associated with prior trauma. As more knowledge is uncovered about the relationship between PTSD and sensory brain structure/function, virtual reality could be a useful tool in helping to correct targeted sensory dysfunction after trauma exposure.
Conclusion
Mechanistically, there is an abundance of data in animal models that sensory processing can change, across most sensory systems, at the level of function and structure following sensory-based fear conditioning and trauma exposure [17,18,54,55]. Here, we have attempted to summarize recent studies in humans that demonstrate the presence of such changes/forms of variability associated with PTSD. With these new lines of evidence, it is becoming increasingly clear that sensory regions, their patterns of connectivity, and subsequent ties to sensory behavior may need to be incorporated more centrally into current lines of thinking around PTSD.
Moving forward, there remains a significant call to action in several areas. First, the major question that remains is: what exactly is represented by the variability in sensory systems that is associated with PTSD? While many aspects of sensory neural circuitry appear to vary with PTSD symptomology, a deeper interpretation of the causal nature of these associations must be considered. This need will perhaps be best served through more longitudinal human studies that further separate the characteristics of pre-existing susceptibility, acute responses in the immediate aftermath of trauma, and the long-term changes that occur at later post-trauma time points. Further work is also needed to build upon animal studies that have probed the susceptibility/changes in sensory cortex associated with trauma and PTSD [17,50,56]. Specifically, these efforts should focus on using pre-clinical models to better understand the mechanisms behind sensory cortex-related changes/susceptibility. For example, using more pre-post trauma designs in animal models will help reveal how variability in sensory circuits contributes to vulnerability for the development of sensory processing dysfunction and PTSD symptomatology after trauma exposure. These types of studies could then be followed by genetic/molecular manipulation of these circuits to determine whether susceptibility can be reduced by strengthening/weakening these pathways Additionally, studies that assess variability among PTSD subjects, beyond traditional case-control analyses, will provide important insight into the relationship between sensory processing and PTSD. While direct comparisons between patients and controls have been informative, much can also be learned by examining how varying degrees of symptom severity relate to variation in sensory-processing among PTSD patients. Finally, leveraging this knowledge is crucial for the development of targeted therapies and the enhancement of existing treatment options through a better understanding of their underlying mechanisms of action. As future studies continue to investigate the relationships between PTSD and sensory processing, it will aid the field in not only understanding more about the sensory mechanisms that contribute to the disorder, but also provide key insight into the dynamic relationship between emotion and sensory processing.
Highlights.
Sensory processing may deserve a more central role in our thinking about PTSD.
PTSD is linked to variability in sensory processing and properties of sensory cortex.
PTSD is related to local & global patterns of functional connectivity in sensory cortex.
PTSD is associated with structural gray/white matter differences in sensory cortex.
Sensory variability may represent susceptibility to, or consequences of, PTSD.