Abstract
What accounts for variation across racial and ethnic groups in drug use and harms related to substance use? While explanatory mechanisms for racial and ethnic disparities include differential access to and use of health services, a myriad of other factors, including racism and historical trauma, contribute to drug-related disparities. Furthermore, the addiction scientific workforce, like the full biomedical research enterprise, lacks diversity. This deficit undercuts U.S. scientific leadership and is a major challenge for the field. To address these entrenched problems, the National Institute on Drug Abuse (NIDA) is prioritizing research on health disparities and supporting multiple efforts to enhance scientific workforce diversity. Studies on substance use trends and emerging threats must measure disparities and track progress in reducing disparities, but also acknowledge the limitations of race and ethnicity-based data. Researchers must take the bold step of proposing studies that elucidate causal mechanisms which have the potential to be ameliorated by novel policies and practices. Critically, the impact of racism on all aspects of the substance use trajectory must be assessed to better tailor prevention, harm reduction, treatment, and recovery-support interventions to the specific circumstances of those who need them. Particular attention should be given to people who are incarcerated, who are experiencing homelessness, and who have a history of adverse childhood experiences. Training the next generation of the addiction science workforce needs to address structural barriers to participation with partnerships between funders, such as NIDA, and grantee organizations.
Highlights
NIDA is prioritizing research on health disparities and supporting efforts to enhance scientific workforce diversity.
Studies on substance use trends and emerging threats must measure disparities and track changes
Acknowledging and addressing the limitations of race and ethnicity-based data is needed.
Studies are required that elucidate causal mechanisms which might be ameliorated by novel policies and practices.
Training the next generation of the addiction science workforce needs to address structural barriers to participation.
1. Introduction
Variation in rates of substance use and outcomes such as overdose, infectious diseases, and justice system involvement, are notable across race and ethnic groups (e.g., see Fig. 1, Han et al., 2022; Furr-Holden et al., 2018; Kiang et al., 2021). While these differences are frequently described in the research literature, the likely origins and meaning of group differences are rarely discussed and sometimes interpreted deterministically when, in fact, “race” and “ethnicity” are inherently social constructs. Furthermore, in the United States, definitions of race and ethnic groups, which are typically based on definitions from the White House Office of Management and Budget (2022), vary over time in ways that impact interpretation of findings.
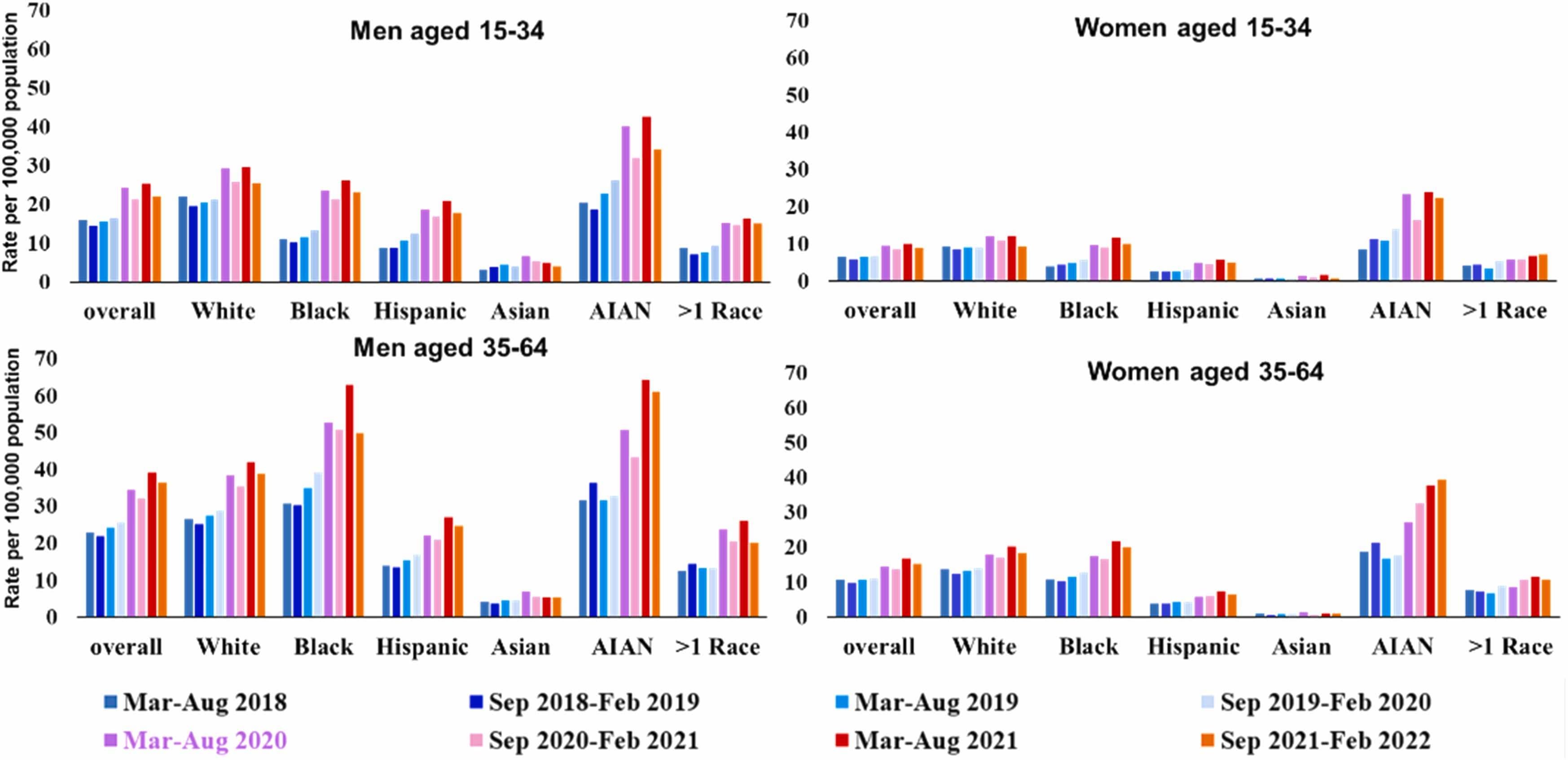
Fig. 1. Age-adjusted overdose death rates in the U.S. according to sex, age-group, and racial and ethnic identity before and during the COVID-19 pandemic (from Han et al., 2022).
Tracking data on rates according to race and ethnicity remains critical because inequities are a threat to overall population health (Cogburn, 2019) and point to areas of high need for treatment and prevention services. Yet, as these data are collected and shared, a challenging question remains: What are effective prevention and treatment interventions to reduce disparities? Answering this question requires an understanding of underlying causes and malleable factors that drive or sustain disparities.
Multiple explanatory mechanisms have been proposed, including differential access to and use of health services. Racism, historical trauma, and other stress theories (including the impact of social determinants of health such as poverty, unemployment, and unstable housing) have all been examined as mechanisms to account for the disparities in substance-related morbidity and mortality (Yearby et al., 2022). Prominent factors addressed in research studies include multi-generational impacts of trauma, unfair housing and lending practices, ongoing experiences of racism and discrimination, as well as traumatic exposure to racially motivated violence either personally or in the media or online.
In particular, communities of color have been disproportionately harmed by decades of inequitable application of punitive and carceral responses to drug possession and use (Mitchell and Caudy, 2015), and the effects of these disparities in criminal policy responses to drug use are significant (National Academies of Sciences, 2019). The disruption and trauma inflicted on historically marginalized communities and families by inequitable drug enforcement also contributes to the social conditions that can lead to increased drug use and other unfavorable outcomes. For instance, disproportionate felony convictions and incarceration can increase difficulties for historically marginalized people in finding housing and employment, separation of children from their parents, and prohibition of people in some places from voting. Thus, disparities in justice systems may exacerbate substance-related harms both directly and indirectly. Responding to these major social and health concerns is a scientific imperative.
2. Scientific responses
In June of 2020, NIDA Director Nora Volkow established the NIDA Racial Equity Initiative to broadly address racial inequity in addiction science, including the workplace at NIDA itself, the scientific workforce supported by NIDA funding, and NIDA’s research portfolio (Volkow, 2021). This work is consistent with the National Institutes of Health (NIH) goal of improving “the NIH culture and structure for equity, inclusion, and excellence” (National Institutes of Health, 2022a), and is consistent with the NIH UNITE initiative, which was developed to explore “understanding barriers; developing robust health disparities/equity research; improving its [NIH] internal culture; being transparent and accountable; and changing the extramural ecosystem so that diversity, equity, and inclusion are reflected in funded research and the biomedical workforce” (Collins et al., 2021).
2.1. Enhancing racial equity in the scientific workforce
Training the next generation of researchers presents both challenges and opportunities. As highlighted in recent examination of trends in training across biomedical fields, the number of persons entering academic careers in biomedicine may be declining (National Institutes of Health, 2023a). A key concern is the relatively low pay for training positions, particularly post-doctoral positions. Relatively low salaries for highly educated and trained persons has been identified as a major contributor to declining participation in post-doctoral positions. These salary concerns may be particularly acute for underrepresented groups in science where family incomes may not support the extended low-salary training that is typical in biomedical science (National Institutes of Health, 2023a).
NIH training grants set the standard for trainee salaries, but they have not kept up with inflation and may not be sufficient to allow persons who lack other sources of income or support to pursue careers in biomedical science. While the need for increased support from NIH continues to be emphasized, such increases to individuals may result in a decrease in the overall number who can be supported if overall funding is not also increased. We also note that grants, such as individual and institutional training grants (i.e., “F” and “T” grants) are assistance mechanisms and can be supplemented with non-federal funds. In fact, multiple institutions have increased their support for pre- and post-doctoral trainees well beyond the NIH stipends (Castiglione, 2023, Langin, 2023). Such additional support would be welcomed by all but may be particularly important to persons from disadvantaged backgrounds.
Specific programs to support workforce development extend well beyond the broad T and F grant programs. For example, programs specifically supported by NIDA include NIDA’s Diversity Scholars Network, the NIDA Summer Research Internship Program, the Loan Repayment Program, Diversity Supplement Awards, and a funding opportunity published in 2022 called “Research Opportunities for New and ‘At-Risk’ Investigators to Promote Workforce Diversity” (Avila et al., 2022, National Institute on Drug Abuse, 2023b, National Institutes of Health, 2022b). In addition, multiple broad NIH efforts are designed to enhance workforce diversity (National Institutes of Health, 2023b).
Continued focus on researcher demographics is crucial for NIH to determine the impact of efforts to enhance racial and ethnic diversity in the scientific workforce. Earlier this year, the NIH Office of Extramural Research published an analysis examining trends in funding for Research Project Grants by demographic characteristics from 2010 to 2022 (Lauer and Bernard, 2023). While progress is demonstrated, absolute numbers of Black and Hispanic applicants remain very low, and the narrowing White-Black gap in funding from 2010 to 2021 backslid between 2021 and 2022 (see Fig. 2). Such analyses will be regularly required to assess if novel, more concentrated approaches to improving racial equity in the workforce result in more meaningful change. Monitoring similar data for the addiction workforce supported by NIDA grants is an important goal to help identify areas that may be improving or may need additional attention.
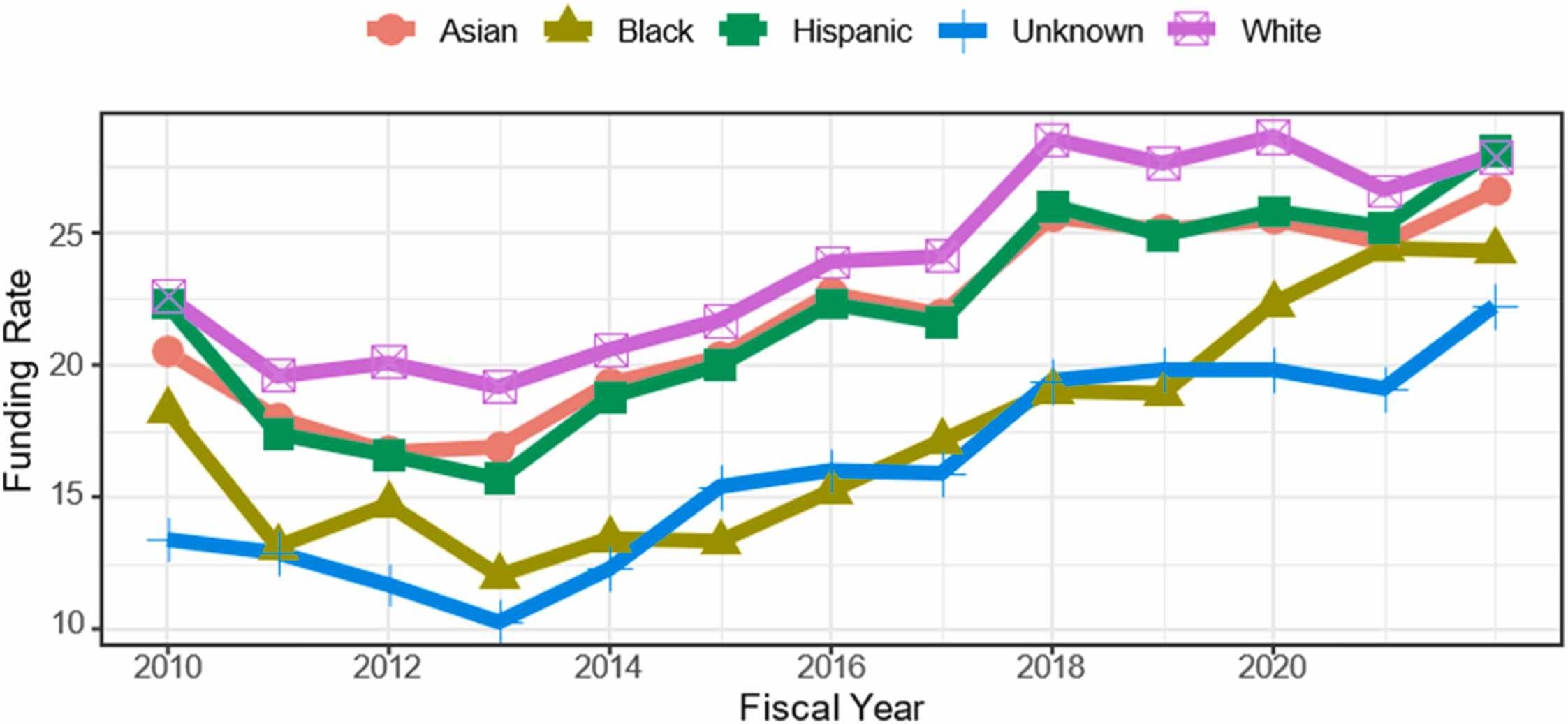
Fig. 2. Funding rates for Type 1 R01-equivalent grants submitted to the National Institutes of Health from 2010 to 2022, according to the race and ethnicity of the principal investigator (from Lauer and Bernard, 2023).
2.2. Enhancing racial equity in NIDA-supported science
New areas of research on racial and ethnic health disparities continue to be promoted and supported by NIDA. Toward the goal of enhancing NIDA research in this area, the Racial Equity Initiative conducted iterative listening sessions and held a scientific meeting in 2021 entitled “Enhancing Health Disparities Research Related to Substance Use and Addiction: Research Gaps and Opportunities” (National Institute on Drug Abuse, 2021). A coordinated suite of funding opportunities was subsequently released to encourage research addressing the gaps identified, including community-engaged research, neurocognitive mechanisms of structural racism, reducing disparities at the intersection of HIV and substance use, and enhancement of addiction research at minority-serving institutions (National Institute on Drug Abuse, 2023a).
As in many areas of health research, addiction research often collects information about participant race and ethnicity, but outcomes for the identified subgroups are not always analyzed. Nor are participant race and ethnicity typically assessed within the full context of social determinants of health or with a strong consideration of race as a social construct. Addressing these gaps may be enhanced with community-engaged research, which is a critical tool to ensure that the perspectives of communities are integrated at the stage of research design and to ensure researchers are addressing the most pressing research questions with the greatest capacity to meaningfully improve health outcomes (Webb Hooper et al., 2022).
Integration of community perspectives is also critical for leveraging resiliency factors to tailor interventions to communities of color. For example, neurodevelopmental impacts of poverty can be mitigated through targeted prevention programs aimed at disadvantaged youth and their families, such as the Strong African American Families prevention intervention studied in Georgia (Brody et al., 2017). Further, while rates of drug use and overdose may be particularly high among American Indian individuals, a growing body of research focuses on the unique strengths of American Indian communities to enhance connection to salutary traditions that are protective against substance use disorders (Barlow et al., 2013, Walls et al., 2016, Barlow et al., 2015). Building on resiliency factors also helps to avoid the discouragement of focusing solely on a nearly endless parade of negative associations.
As previously described, criminalizing drug use has profoundly impacted communities of color. Research on best interventions for substance use disorders in carceral settings that takes into account race and ethnicity may help ameliorate health disparities around drug use and addiction. NIDA has long supported research in justice settings, including landmark studies such as Inciardi and colleagues’ treatment outcome work (Inciardi et al., 1997) and work to enhance integration of public health and public safety actions (Chandler et al., 2009). More recently, the Justice Community Opioid Innovation Network, has launched a coordinated set of research projects aiming to improve evidence-based care across justice settings including prison, jail, drug court, probation, parole, and community re-entry (Ducharme et al., 2021).
3. Conclusions and call to action
Scientific research must provide opportunities both to continue to track emerging shifts in rates of drug use and drug-related harms across multiple racial and ethnic subgroups and to elucidate causal mechanisms. Critically, the impact of racism on all aspects of the substance use trajectory must be assessed to better tailor the prevention, harm reduction, treatment, and recovery-support interventions to the specific circumstances of those who need them.
Research on the social, historical, and contextual factors that influence health is a growing focus for the entire National Institutes of Health (Bernard et al., 2021, Tabak and Collins, 2011). Widening the lens beyond biology and health care access reveals just how impactful these factors can be and is illuminating potential new ways to improve health and reduce health disparities. For example, a longitudinal study capturing the beginning of income supports for American Indian families documented improved mental health outcomes for the children of those families that continued to manifest even 20 years later, along with reduced risky or illegal behaviors, increased physical health, and improved financial functioning (Copeland et al., 2022). Income supports during the COVID-19 pandemic may offer another natural experiment to measure the health effects of reduced financial insecurity (Weissman et al., 2023).
In addition to the new research solicited by the NIDA Racial Equity Initiative, large, ongoing research projects are poised to address questions around experiences of racism and its impact on health outcomes, along with other insights, to guide development of policies and interventions to reduce health disparities. The ABCD Study and the new HEALthy Brain and Child Development Study, which together are assembling large-scale datasets on brain development spanning the prenatal period through age twenty, are expected to enable researchers to study the complex web of influences that leads to disparities in substance use and addiction outcomes (Volkow et al., 2020, Volkow et al., 2018).
Additional research is needed to maintain an accurate understanding of the landscapes of drug use and addiction outcomes and their intersections with race and ethnicity. Epidemiological data on people who are incarcerated, who are experiencing homelessness, and who are absent from school (i.e., excluded from school-based surveys) are urgently needed to fill gaps in our surveillance systems. Collection of data on contextual factors must also inform these and other clinical studies to best account for variable outcomes, elucidate the multifactorial pathways that lead to health disparities, and ultimately inform the implementation of effective solutions (Jordan et al., 2020).
Multiple approaches to addressing workforce diversity are underway at NIDA and NIH. Partnerships and extension of these programs in academic centers is essential for their success. For instance, as described above, NIH support for trainees may not be adequate to allow persons of limited means to engage in a research career. With NIH grants as a foundation, grantee organizations could offer additional support to assure equitable access to scientific training.
Communities of color in the United States have experienced iterative harms, from the assaults on health and safety associated with colonization, slavery, and genocide, through lynching, segregation, redlining, and mass incarceration (Comas-Díaz et al., 2019, Gameon and Skewes, 2021, Gone et al., 2019, Skewes and Blume, 2019). These profound influences cannot be ignored in the consideration of how to best address the clear health disparities that accompany the current U.S. drug crisis, as well as the entrenched lack of diversity in the biomedical research workforce.
Contributions
The manuscript was conceptualized by all authors, drafted by Compton, Einstein, Wargo, and edited for important content by all authors.
Disclaimers
The opinions in this perspective are those of the authors and do not necessarily represent the official opinions of the National Institute on Drug Abuse, the National Institutes of Health, or the U.S. Department of Health and Human Services.
Declaration of Competing Interest
Unrelated to the submitted work, Compton reports ownership of stock in General Electric Co., 3 M Co., and Pfizer Inc. Other authors have no conflicts to disclose.