Abstract
Background: Racial and ethnic groups in the USA differ in the prevalence of posttraumatic stress disorder (PTSD). Recent research however has not observed consistent racial/ethnic differences in posttraumatic stress in the early aftermath of trauma, suggesting that such differences in chronic PTSD rates may be related to differences in recovery over time.
Methods: As part of the multisite, longitudinal AURORA study, we investigated racial/ethnic differences in PTSD and related outcomes within 3 months after trauma. Participants (n = 930) were recruited from emergency departments across the USA and provided periodic (2 weeks, 8 weeks, and 3 months after trauma) self-report assessments of PTSD, depression, dissociation, anxiety, and resilience. Linear models were completed to investigate racial/ethnic differences in posttraumatic dysfunction with subsequent follow-up models assessing potential effects of prior life stressors.
Results: Racial/ethnic groups did not differ in symptoms over time; however, Black participants showed reduced posttraumatic depression and anxiety symptoms overall compared to Hispanic participants and White participants. Racial/ethnic differences were not attenuated after accounting for differences in sociodemographic factors. However, racial/ethnic differences in depression and anxiety were no longer significant after accounting for greater prior trauma exposure and childhood emotional abuse in White participants.
Conclusions: The present findings suggest prior differences in previous trauma exposure partially mediate the observed racial/ethnic differences in posttraumatic depression and anxiety symptoms following a recent trauma. Our findings further demonstrate that racial/ethnic groups show similar rates of symptom recovery over time. Future work utilizing longer time-scale data is needed to elucidate potential racial/ethnic differences in long-term symptom trajectories.
Introduction
Psychiatric illness prevalence within the United States, particularly trauma and stress-related disorders, varies by racial and ethnic groups. While racial and ethnic categories are not true biological divisions in humans, individuals are racialized into these groups by virtue of their societal systems which in turn affects mental health. For example, Black individuals typically show lower rates of internalizing disorders such as posttraumatic stress disorder (PTSD), anxiety, and depression compared to White individuals (Breslau et al., 2006; Kessler et al., 2005). Although the prior work highlights race-related differences in the prevalence of posttraumatic dysfunction, limited work to date has investigated racial/ethnic differences in symptoms that present in the early aftermath of trauma. Recent research demonstrates peritraumatic responses to traumatic events may be indicative of later chronic dysfunction or may map onto other discernable trajectories of trauma recovery/deterioration (Bonanno & Mancini, 2012; Galatzer-Levy et al., 2013; Shalev et al., 2019). There is a paucity of research on potential racial/ethnic variability in peritraumatic responses or the trajectories of trauma symptoms in first several months after trauma which may impact the generalizability or accuracy of predictive models of susceptibility to posttraumatic disorders. The purpose of the present analysis is to characterize potential racial/ethnic differences in the trajectories of trauma-related disorder symptoms in the early aftermath of trauma.
Prior epidemiological data suggests that White individuals report greater exposure to any traumatic event and childhood physical abuse compared to Black or Hispanic individuals (Roberts, Gilman, Breslau, Breslau, & Koenen, 2011). Exposure to prior traumatic events is a major predictor of subsequent PTSD development following a later trauma and thus may be related to greater rates of PTSD in White individuals (Gould et al., 2021). However, global epidemiological data highlights that the type of prior traumatic event (such as violence victimization) also influences subsequent PTSD development (Kessler et al., 2018; Liu et al., 2017). Importantly, Black and Hispanic individuals generally experience more childhood adversities, community violence exposure, and exposure to other environmental inequities that impact health (Maguire-Jack, Lanier, & Lombardi, 2019; Sheats et al., 2018; Slopen et al., 2016; Williams & Collins, 2001; Williams, Mohammed, Leavell, & Collins, 2010). Further, Black individuals often have less wealth and lower income compared to White individuals and higher income may afford access to systems that can attenuate the consequences of traumatic events (e.g., healthcare access) and buffer against the financial and social consequences of trauma (Cook, Trinh, Li, Hou, & Progovac, 2017; Herring & Henderson, 2016; Yearby, 2018). As discussed, these types of traumatic experiences are also associated with high conditional risk of PTSD after experiencing a subsequent trauma (Powers, Fani, Cross, Ressler, & Bradley, 2016; Yehuda, Halligan, & Grossman, 2001). Thus, the on-average greater disadvantage experienced by minority group individuals may contribute to greater posttraumatic dysfunction. However, racial/ethnic minority groups generally report a lower prevalence of PTSD (Breslau et al., 2006; Kessler et al., 2005), and thus non-White individuals may in fact show reduced severity of posttraumatic dysfunction in the early aftermath of trauma compared to white individuals. Limited work to date, however, has investigated racial/ethnic differences in posttraumatic symptoms in the early aftermath of trauma.
There is some ambiguity as to whether greater resilience to posttraumatic dysfunction may be present in non-White individuals in the aftermath of trauma (Muralidharan, Austern, Hack, & Vogt, 2016). Some exposures more often experienced by Black and Latinx individuals (e.g., chronic neighborhood disadvantage) are not captured well within the DSM-5 conceptualization of trauma and may be related to lower reports of PTSD-related symptoms. However, a component of commonly reported lower PTSD prevalence rates may be due to underreporting of symptoms in epidemiological surveys or lower healthcare availability or utilization in minority racial groups that impacts survey participation (Cook et al., 2017; Miranda, McGuire, Williams, & Wang, 2008). These may partially explain why some prior research has observed higher rates of undiagnosed PTSD in disadvantaged Black individuals (Davis, Ressler, Schwartz, Stephens, & Bradley, 2008; Parto, Evans, & Zonderman, 2011). In addition, a recent report demonstrated that racial discrimination experienced by Black individuals was a risk factor for future PTSD symptom development after trauma (Bird et al., 2021). Thus, race-related stressors may also exacerbate racial/ethnic differences in early PTSD symptoms.
Early prior research from the AURORA study, a multisite longitudinal study of posttraumatic outcomes (McLean et al., 2019), have identified factors associated with the expression of PTSD and depression symptoms in the early aftermath of trauma such as peritraumatic distress and dissociation, or neurophysiological responses (Harnett et al., 2021; Joormann et al., 2020; Kessler et al., 2020; Steuber et al., 2021). Interestingly, the early AURORA work did not identify robust racial/ethnic differences in posttraumatic symptoms within the first two to eight weeks after trauma. We note however that the prior work did not investigate racial/ethnic variation in posttraumatic stress in further time points (e.g., 3-months after trauma exposure) or potential relationships with structural inequities and prior trauma exposure. Given the dissociation between racial/ethnic variability in posttraumatic stress in the early versus long-term aftermath of trauma, it may be that differences in symptom expression over time start to emerge in later time points (e.g., 3-months posttrauma); however, potential differences in symptom expression have not been examined as of yet. Thus, potential racial/ethnic differences in early trauma outcomes remains unclear. Characterizing potential racial/ethnic differences in posttraumatic syndromes over the first several months after trauma is necessary for the development of precision medicine approaches to identify individuals susceptible to long-term posttraumatic dysfunction.
Therefore, to investigate racial/ethnic differences in posttraumatic symptoms in the first three months after a traumatic event, we analyzed data from the AURORA study. We first compared 2-week, 8-week, and 3-month indices of posttraumatic dysfunction (i.e., PTSD, depression, anxiety, or dissociation symptoms) between White, Black, and Hispanic groups. Based on prior literature, we hypothesized that Black and Hispanic individuals would show lower symptoms of posttraumatic dysfunction over time compared to the White individuals. We then examined if controlling for demographic cofactors (e.g., income and employment) contributed to observed racial differences in posttraumatic symptoms. Finally, we completed follow-up analyses investigating the effect of childhood trauma and other prior traumatic events on observed racial differences in posttraumatic symptoms. The present findings provide insight into the impact of race/ethnic-related differences in pretraumatic stressors on traumatic stress reactions in the aftermath of trauma.
Materials and Methods
Participants
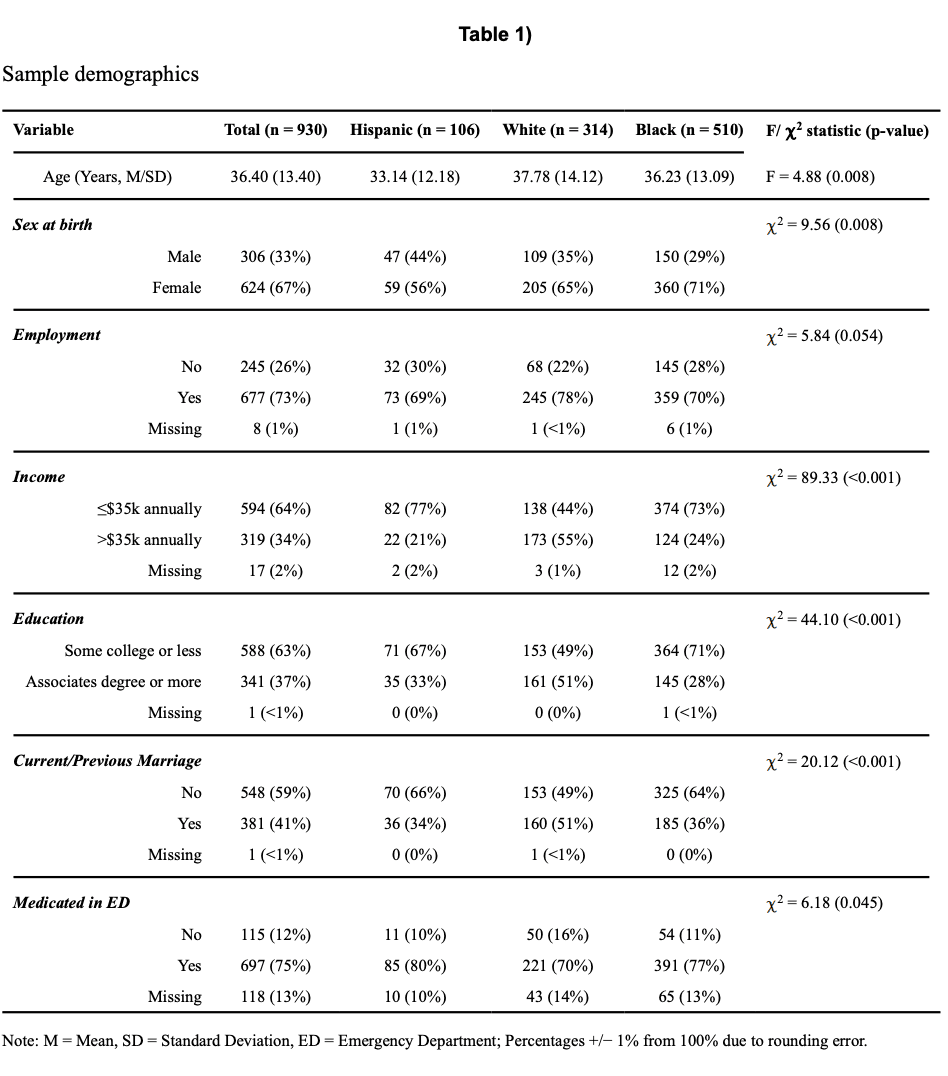
Data from the present analyses were obtained as part of the Freeze 2 psychometric data release of the AURORA Study, a multisite longitudinal study of adverse neuropsychiatric sequelae. Details of the larger AURORA project are described elsewhere (McLean et al., 2019). Briefly, trauma-exposed participants were recruited from Emergency Departments (EDs, n = 29) from across the United States. Trauma was defined as a medical accident requiring admission to the ED, and participants who experienced events such as a motor vehicle collision, high fall (>10 feet), physical assault, sexual assault, or mass casualty incidents were automatically included in the study. Other trauma exposures were also qualifying if: a) the individual responded to a screener question that they experienced the exposure as involving actual or threatened serious injury, sexual violence, or death, either by direct exposure, witnessing, or learning about the trauma and b) the research assistant agreed that the exposure was a plausible qualifying event. Trauma was a necessary inclusion criterion for the present study, and no participants without trauma were included. The psychometric data included 1,618 participants recruited between 09/25/2017 and 06/31/2019, however the present analyses were focused on racial/ethnic differences in the posttraumatic outcomes. Thus, we excluded participants who did not have data on posttraumatic dysfunction (i.e., PTSD, depression, anxiety, dissociation, or resilience symptoms) across all timepoints (n = 645). Participants self-reported their race/ethnicity and were coded into four categories of “Hispanic” (“Hispanic”; n = 106),” “non-Hispanic White (“White”; n = 314),” “non-Hispanic Black (“Black”; n = 510),” and “non-Hispanic other-race (“Other”; n = 43).” For the present analyses, we also excluded participants from the “other” racial category due to small sample size that may impact statistical analyses. In total, 930 participants had completed assessments of all measures of posttraumatic dysfunction at the three timepoints and were included in the present analyses (Table 1). A breakdown of the broad class of trauma-types experienced by each group are presented in Table S1. Note, there were no significant differences in the racial/ethnic make-up of the included versus excluded sample [χ2 (2) = 2.34, p = 0.31]. All participants gave written informed consent as approved by each study site’s Institutional Review Board.
Demographic and psychometric data collection
Participant demographic data were collected after admission to the ED which included participant marital status, income, education level, employment, and medication administered within the ED (see Table S2 for medication and Table S3 for full demographic category breakdowns). After discharge, participants’ posttraumatic symptoms were assessed at 2-weeks, 8-weeks, and 3-months after trauma exposure (described below). The 2-week assessment queried participant symptoms in the past 14 days while the 8-week and 3-month assessments queried participant symptoms in the past 30 days. Participants also completed retrospective reports within the ED (past 30 days prior to the trauma) of posttraumatic dysfunction symptoms.
Measures of posttraumatic dysfunction
Participants’ posttraumatic dysfunction was assessed in terms of PTSD, depression, anxiety, and dissociation symptoms. PTSD symptoms were assessed using the PTSD Checklist for DSM-5 (PCL-5) (Weathers, Litz, et al., 2013), a 20-item self-report questionnaire on symptom expression and severity. Depression symptoms were assessed using the Patient-Reported Outcomes Measurement Information System (PROMIS) Depression instrument from the PROMIS short form 8b (Pilkonis et al., 2011). T-scores were derived from total responses to eight items scored on a Likert scale from 1 (never) to 5 (always). Anxiety symptoms were assessed using four items from the PROMIS Anxiety Bank (Pilkonis et al., 2011). Participants rated how often they felt anxious, worried about things, had trouble relaxing, or felt tense on a scale of 1 (none of the time) to 5 (all or almost all of the time) and the responses were summed to create a total anxiety score. Dissociation was assessed using a modified version of the Brief Dissociative Experiences Survey (Bernstein Carlson & Putnam, 1993). Participants were asked to rate how often they felt that people, objects, or the world around them seemed unreal and how often they felt they were looking through a fog so that people and things seemed unclear on a scale from 1 (none of the time) to 5 (all or almost all of the time). The sum of the two questions was used as an index of dissociation severity. As a contrast to the measures of posttraumatic symptoms, we also assessed participants’ psychological resilience using the Connor Davidson Resilience Scale (CD-RISC) (Connor & Davidson, 2003).
Prior trauma exposure
Prior trauma was assessed using the Life Events Checklist version 5 (LEC-5) (Weathers, Blake, et al., 2013). The checklist assessed prior exposure to traumatic events such as natural disasters, accidents, assaults, etc. that: a) happened directly to the participant, b) were witnessed by the participant, c) the participant learned happened to someone close to them, or d) the participant was exposed to details of it due to their occupation. The LEC-5 was administered during the 8-week assessment. Responses to all questions were summed to derive a prior trauma index. We also indexed childhood trauma via 11 items from the Childhood Trauma Questionnaire – Short Form (CTQ) (Bernstein et al., 2003). Participants were asked to rate how often they experienced maltreatment across five domains (emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect) from a scale of 0 (never true) to 4 (very often true). The CTQ was administered during the 2-week assessment.
Statistical analyses
Statistical analyses were completed using a combination of IBM SPSS Statistics version 24 (Armonk, NY) and the JASP statistical package (https://jasp-stats.org/). Chi-square and univariate analysis of variance (ANOVA) models were completed to assess differences in demographic factors between the racial/ethnic groups. Our initial research questions were focused on racial/ethnic group differences in different posttraumatic outcomes over time. We completed sets of linear mixed-effects models with unstructured covariance matrices to investigate race-related differences in posttraumatic dysfunction measures across the five domains assessed (i.e., PTSD, depression, dissociation, anxiety, and resilience). In Model set A, time (3 levels) and racial/ethnic group (3 levels) were included as fixed factors to assess main effects of racial/ethnic group and differences over time for each measure of posttraumatic dysfunction (five models total). In Model set B, covariates for age, employment status, income, education, marital status, and medication usage during recruitment from the ED were included to determine if race/ethnic differences were observed above and beyond base demographic factors. Demographic data were dummy-coded for inclusion as covariates in linear mixed-effects models (marital status: married vs not; income: <= $35,000 vs > $35,000; education: completed high-school or less, completed greater than high-school; employment: employed vs not; ED medication: yes vs no). Income was dummy-coded based on the median response. We completed separate univariate ANOVAs on assessments completed in the ED to determine if racial/ethnic differences in posttraumatic dysfunction were potentially driven by pre-trauma symptoms. We then repeated Model set A controlling for pre-trauma symptoms and this analysis is reported in the supplement. We next sought to determine if other potential pre-trauma factors may be related to the observed race-related differences in posttraumatic depression and anxiety severity. We focused on prior lifetime and childhood trauma given prior work has demonstrated these factors are major risk factors for subsequent PTSD. The prior trauma index derived from LEC-5 was used in an ANOVA with racial group as the between-subjects factor. To investigate racial/ethnic differences in childhood trauma, subscale scores for the five domains of the CTQ assessing emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect were entered in a multivariate analysis of variance (MANOVA) with a between-subjects factor for racial group. Prior trauma types that differed significantly between the racial/ethnic groups were included in a final linear model as covariates (Model set C). Bonferroni corrections were applied to the linear models based on our a priori interest in the time by racial group interactions and main effects of racial group (2 contrasts per model, 10 total comparisons) and effects were considered statistically significant at an adjusted p = 0.005 (0.05/10) per model set.
Results
Race-related differences in participant characteristics
ANOVA and Chi-squared tests were completed to assess racial/ethnic differences in the demographic factors (Table 1). Significant differences in age and proportions of sex at birth categories were observed between the racial/ethnic groups. No statistically significant difference was observed in employment status for the three groups. Racial/ethnic groups differed in income status, education, marriage status, and ED medication use. Black and Hispanic groups had a greater proportion of participants who were low income, had less than an associate’s degree or equivalent, and were not currently or previously married. Medication usage in the ED was generally higher for Hispanic participants.
Race-related differences in posttraumatic outcomes
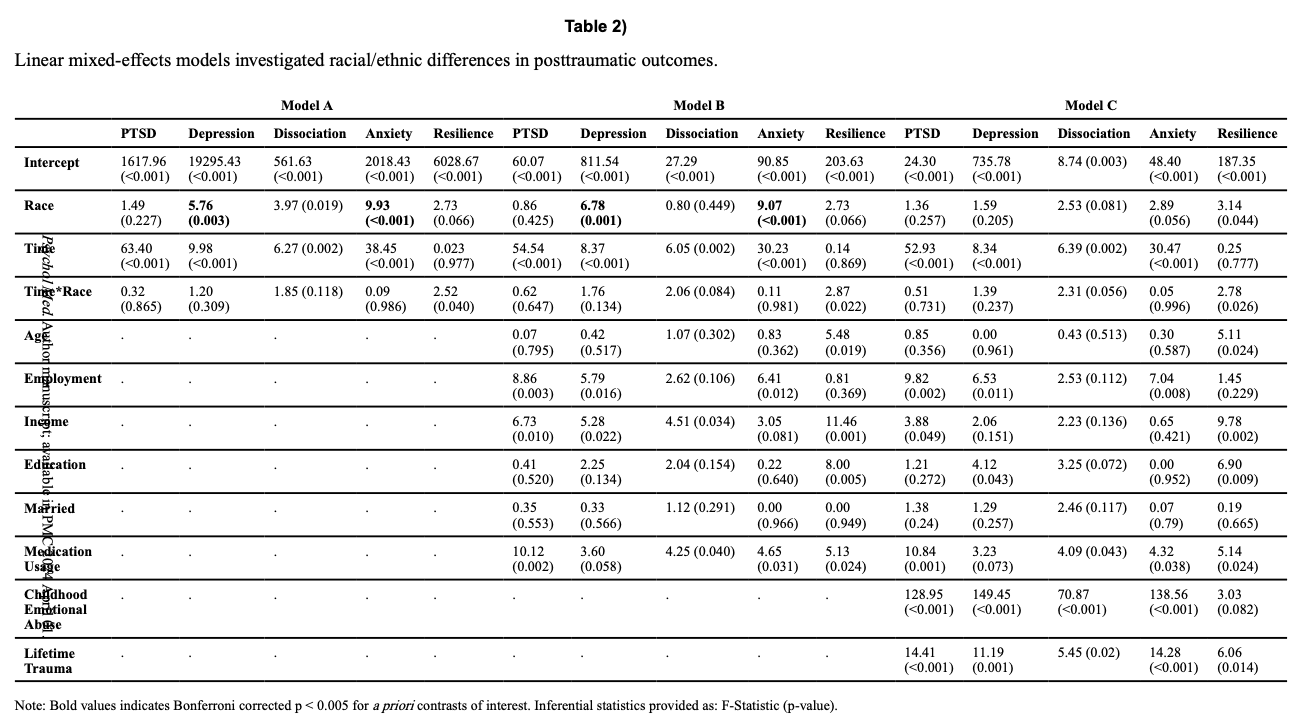
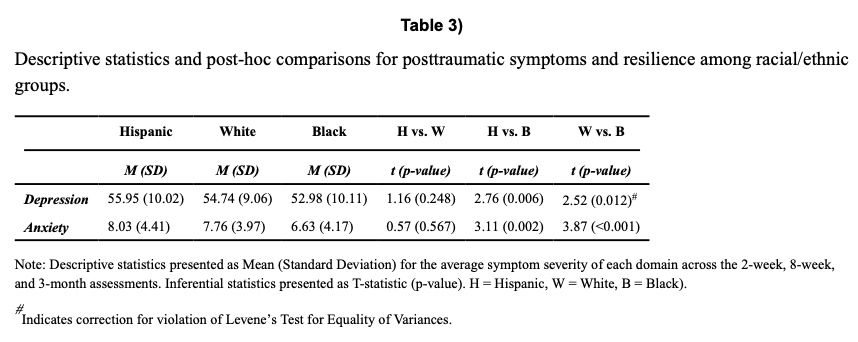
Linear mixed-effects models were completed to assess racial/ethnic differences in PTSD, depression, anxiety, dissociation, and resilience scores with and without inclusion of covariates (Table 2). We observed significant main effects of racial/ethnic group on depression and anxiety scores that persisted when accounting for differences in demographic factors. Post-hoc comparisons revealed that Black participants showed lower overall posttraumatic depression and anxiety severity compared to Hispanic and White participants (Table 3). For completeness, exploratory post-hoc comparisons between groups of each measure at each timepoint are presented in the supplement (Table S4). Taken together, these findings demonstrate that the general severity of post-trauma depression and anxiety are lower in recently trauma-exposed Black individuals, and these differences do not appear to be driven by differences in general demographic factors.
We completed follow-up exploratory analyses to investigate if racial/ethnic differences in posttraumatic dysfunction existed prior to ED admission via the retrospective reports. We observed significant main effects of race/ethnicity on depression, dissociation, and anxiety symptoms (Table S5). When the original linear mixed-effects models also included retrospective reports of posttraumatic dysfunction in the ED, we observed significant main effects of race on anxiety symptoms (Table S6; p = 0.028). These findings suggest some aspect of the observed racial/ethnic differences in posttraumatic dysfunction were driven by pre-trauma factors.
Previous trauma exposure and childhood trauma as potential factors
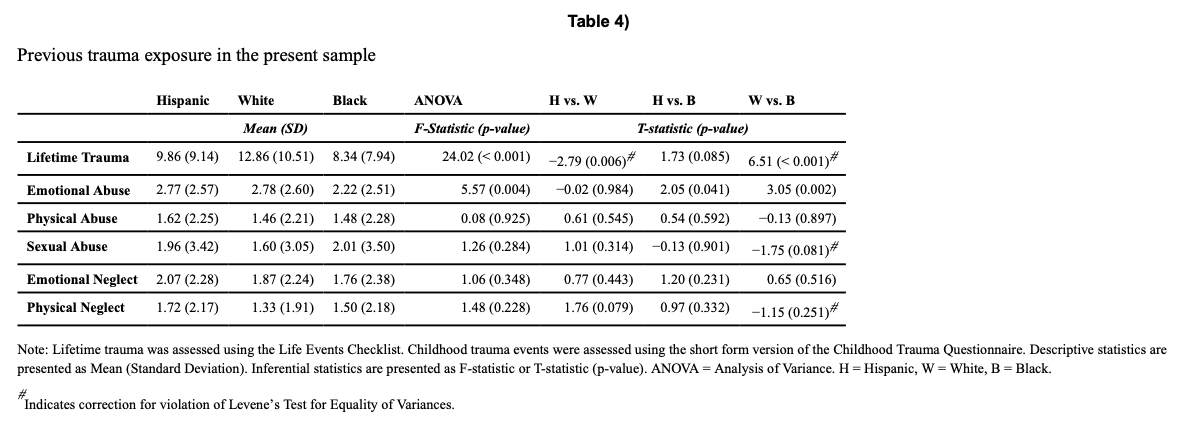
We next investigated racial/ethnic differences in lifetime and childhood trauma as potential pre-trauma factors influencing posttraumatic stress symptoms. We observed a significant main effect of racial group on prior trauma such that White participants endorsed a greater number of traumatic events compared to Hispanic and Black participants (Table 4). Further, we observed a significant omnibus effect of racial group [F(10,1776) = 3.97, p < 0.001, Wilk’s λ= 0.96]. Follow-up univariate ANOVAs revealed race-related differences were specific to emotional abuse, such that White participants reported more emotional abuse compared to Black participants. Of note, prior trauma and childhood emotional abuse were significantly, but weakly, correlated (r = 0.20, p < 0.001).
Given these findings, we repeated the original linear mixed effects models to account for differences in prior trauma and childhood emotional abuse. When accounting for prior trauma and emotional abuse, racial/ethnic group was no longer associated with posttraumatic depression severity or posttraumatic anxiety (Table 2). Taken together, these findings suggest race-related differences in posttraumatic depression and anxiety are partially due to differences in prior reported trauma exposure.
Discussion
Despite evidence of racial/ethnic differences in the chronic and long-term effects of trauma, there are limited data on racial/ethnic differences in posttraumatic outcomes in the early aftermath of trauma. Within the present analyses of a large sample of Hispanic, White, and Black trauma victims, we observed significantly lower posttraumatic depression and anxiety symptoms among Black individuals compared to Hispanic and White individuals. Racial/ethnic differences in depression and anxiety were not attenuated when controlling for differences in socioeconomic indicators or emergency department medication use. However, racial/ethnic differences in posttraumatic symptoms were attenuated when considering differences in prior trauma exposure and childhood emotional neglect. Together, the present findings illustrate that previous exposure to traumatic stress mediates, in part, racial/ethnic differences in depression and anxiety severity in the early aftermath of trauma exposure.
Contrary to our hypotheses, racial/ethnic groups in the present study did not differ in trajectories of recovery from posttraumatic dysfunction over time. Instead, Black individuals displayed – on average – lower severity of depression and anxiety symptoms than Hispanic and White individuals. Prior epidemiological findings suggest that Black and Hispanic individuals have lower occurrence of more chronic disorders such as PTSD and depression (Kessler et al., 2005); however, earlier analyses utilizing data from the AURORA study did not observe racial/ethnic differences in the immediate (i.e., 2-8 weeks) post-trauma phase (Joormann et al., 2020; Kessler et al., 2020). Thus, we initially suspected that racial/ethnic groups would show differing trajectories in symptom severity over time that may explain the discordance between prior research on peri- and- chronic posttrauma outcomes. The lack of a significant time by racial/ethnic group interaction may suggest that differences in recovery trajectory occur at a longer timescale than what was captured in the current analysis (i.e., beyond 3-months). An alternative hypothesis is that posttraumatic dysfunction trajectories are not different between groups, but that differences in the assessment of prevalence rates of chronic dysfunction across racial/groups partially reflects structural inequities. For example, racial/ethnic minority individuals with high symptoms may not be included in these assessments due to confounding factors (e.g., lack of resources) that limit participation. Further analyses within the growing longitudinal AURORA dataset may be able to disentangle posttraumatic trajectories on larger timescales and assess potential attrition related confounds contributing to racial/ethnic differences in posttraumatic outcomes.
Importantly, racial/ethnic differences in posttraumatic depression and anxiety were largely accounted for by differences in prior trauma and childhood emotional abuse. These findings are consistent, in part, with prior work showing that lifetime trauma load is a significant predictor of later PTSD development (Breslau, Chilcoat, Kessler, & Davis, 1999; Kolassa et al., 2010). Further, childhood trauma and adverse childhood experiences are also associated with a range of adult mental health outcomes (McLaughlin et al., 2017; Powers et al., 2016; Schilling, Aseltine, & Gore, 2007). Thus, our data provide support for the model that previous trauma exposures contribute to greater posttraumatic dysfunction after a recent trauma. Somewhat counterintuitively, however, the greater rates of previous trauma were observed in WA participants compared to Hispanic and Black participants. These differences are relatively surprising particularly given the greater amounts of structural adversity (e.g., lower income and education levels) endorsed by Black and Hispanic groups in the present sample.
The disconnect between the present assessment of previous trauma and posttraumatic symptoms and previously observed racial differences in traumatic stress leads to several potentially interesting hypotheses. On the one hand, it should be considered that the current findings may reflect racial/ethnic differences in how individuals from minority groups consider or contextualize events as abuse. Racial/ethnic groups globally and within the US differ in the use and perception of behaviors typically regarded as abusive (e.g., corporal punishment) (Lansford et al., 2015; Taylor, Hamvas, & Paris, 2011). The normalizing of such behaviors may contribute to a hesitancy or inability to consider the events as abusive. As an example, a prior report found that racial/ethnic minority young adults report greater emotional abuse (Brown, Fite, Stone, Richey, & Bortolato, 2018). Further, racial/ethnic minority youth were less able to identify internal feelings as were those with more reported experiences of emotional neglect. These results may suggest that childhood maltreatment contributes to difficulty contextualizing abusive behaviors. Thus, one speculative hypothesis is that the relatively older adults in the present sample are not endorsing events as abusive. On the other hand, the present findings may reflect unique aspects of racialized experiences for White, Black, and Hispanic individuals. Contemporary models of threat and deprivation (McLaughlin, Sheridan, & Lambert, 2014) conceptualize traumatic stressors and abuse as “threats” that are more directly related to the development and expression of posttraumatic symptoms (McLaughlin et al., 2017). Conversely, structural inequalities such as poverty may reflect “deprivation” and this may have greater impacts on future cognitive functioning (Busso, McLaughlin, & Sheridan, 2017). Although cognitive performances were not assessed here, our data may partially support this model in that White individuals experienced more “threat” and minority individuals experienced more “deprivation” and – accordingly – White individuals showed more posttraumatic depression and anxiety symptoms. The relative contributions of such threat-deprivation models to posttraumatic symptoms in the early aftermath of trauma are still relatively unknown and may be one approach to understanding racial/ethnic differences in posttraumatic dysfunction. Speculatively, both of the proposed mechanisms may be relevant to the present results, however it is not possible to disentangle the contributions in the current analyses. Nevertheless, the current findings highlight the need to consider pre-trauma factors that may contribute to race-related differences in peri-and-post-traumatic responses.
Socioeconomic factors such as education and income did not modulate racial/ethnic differences in posttraumatic depression and anxiety. Prior work suggests socioeconomic factors such as education and income moderate the severity of depression and anxiety symptoms and race-related differences in these factors may contribute to racial/ethnic differences in mental health (Chen et al., 2019; Everson, Maty, Lynch, & Kaplan, 2002). Though not the main focus of the present report, we note that income, education, and employment were uniquely associated with PTSD, depression, and anxiety symptoms as well as resilience after trauma exposure. Together, our findings suggest these factors do play a role in posttraumatic responses but do not account for racial/ethnic differences in the early aftermath of trauma.
Several limitations should be noted for the present study. Although our sample is among the largest of longitudinal studies assessing posttraumatic dysfunction immediately following trauma, we were limited in defining racial/ethnic classification to one of three groups. Racial/ethnic variation within the United States is considerably high, and each identity likely has its own stressors that may add nuance to the present results. Future work will be needed to provide more granularity to the present findings. In addition, due to modeling constraints, we only included individuals with complete data on all outcome psychometrics through 3-months after trauma. It is possible that there may be attrition-related interactions with race/ethnicity that we are not able to disentangle here that are relevant for characterizing racial/ethnic differences in posttraumatic outcomes. Another important note is that data were only available for up to three months after the traumatic event. Although we did not observe any differences in changes over time, it is possible that some groups may show significant trajectory changes for periods beyond three months after the traumatic event. It will be necessary to investigate longitudinal changes, ideally leveraging large-scale databases such as the ever-growing AURORA study. However, other datasets from large-scale studies such as the All of Us Research Program (“The ‘All of Us’ Research Program,” 2019), Psychiatric Genomics Consortia (Cichon et al., 2009; Logue et al., 2015), and the Adolescent Brain and Cognitive Development study (Volkow et al., 2018), may also shine important light on the impact of racial/ethnic differences in chronic posttraumatic dysfunction and early childhood pretraumatic factors.
Further, we note that while our approach indexed prior trauma exposure, it is unclear if there were racial/ethnic differences in frequency of specific traumatic events. The LEC-5 was not designed to assess frequency of specific events and although we included a second measure – the CTQ – to improve our index of prior trauma exposure additional research on potential differences in event frequency are needed. Further disentanglement of trauma frequency or proximity to trauma may improve efforts for clarifying individual vulnerability to posttraumatic dysfunction (Weis, Webb, Stevens, Larson, & deRoon-Cassini, 2021). A final limitation is that we did not consider other potentially protective factors in race-related differences of posttraumatic dysfunction. Prior work has highlighted that group differences in behaviors such as religious service attendance may partially explain lower reported mental illness prevalence in Black groups (Reese, Thorpe, Bell, Bowie, & La Veist, 2012). Future work may thus benefit from a consideration of potentially protective factors for race-related differences in posttraumatic dysfunction in the early aftermath of trauma.
In conclusion, the present study demonstrates race-related differences in posttraumatic depression and anxiety are partially driven by racial/ethnic differences in pretraumatic exposures to different life stressors. In particular, White participants’ greater exposure to traumatic events and childhood emotional neglect appeared to potentiate depression and anxiety symptoms after a recent trauma. These findings shed important light on pretraumatic risk factors for posttraumatic dysfunction and provide better understanding of race/ethnicity-related differences in the early aftermath of trauma.
Supplementary Material
Supplement
NIHMS1795430-supplement-Supplement.docx (44.5KB, docx)