Abstract
Adolescents are often the most vulnerable to risky behaviors due to their quest for independence, experimentation, and identity development, resulting in deep-rooted patterns that affect health across the life course. This review examines the prevalence and determinants of substance use and sexual risk behaviors among adolescents in the United States. A systematic search of peer-reviewed literature published between 1980-2023 was conducted using multiple databases. Studies focusing on U.S. adolescents aged 12-19 and reporting on prevalence or associated factors of substance use (alcohol, tobacco, marijuana, or any illicit drugs) or sexual risk behaviors (early sexual initiation, multiple partners, or inconsistent condom use) were included. The review synthesized data from 40 studies meeting inclusion criteria. Results indicate concerning rates of substance use and sexual risk-taking, with variations by demographic factors. Alcohol and marijuana use were most prevalent, reported by 30-40% of adolescents. Nearly half of high school students reported having sexual intercourse, with 40% not using condoms consistently. Prevalence was generally higher among older adolescents, sexual minorities, and some racial minority groups. Key determinants of risk behaviors were reviewed based on socioecological models including individual, interpersonal, community and societal factors. The review highlights the multilevel nature of influences on adolescent risk behaviors. Findings underscore the need for tailored interventions addressing multiple determinants. Particular attention to vulnerable groups such as African American Adolescents and social determinants of health inequities is warranted. More research on risk and protective factors and effective interventions is needed. This synthesis can inform the development of evidence-based policies and programs to reduce substance use and sexual risk behaviors among U.S. adolescents.
1. Introduction
Currently, there are 1.3 billion teenagers worldwide, which accounts for 16% of the global population. This is the greatest number of adolescents in history, according to UNICEF (2022a). People often neglect adolescents' health concerns because of their relatively good health and lower need for healthcare services. Adolescence represents a critical developmental period marked by a quest for independence, experimentation, and identity development (Sisk & Gee, 2021). During this stage, experimentation with risky behaviors particularly substance use, and risky sexual activity is common, frequently resulting in deep-rooted patterns that affect adolescents' health, wellbeing, and life trajectories (Ruprah et al., 2017; Patton et al., 2016).
Adolescent substance use, including alcohol, tobacco, marijuana, and other illicit drugs, is associated with numerous adverse outcomes such as impaired cognitive functioning, mental health issues, and increased risk of addiction in adulthood (Squeglia et al., 2015; Schulte & Hser, 2014; Bugbee et al., 2019). Similarly, early sexual initiation, multiple sexual partners, and inconsistent condom use put adolescents at elevated risk for sexually transmitted infections (STIs), including HIV, and unintended pregnancies (Satterwhite et al., 2013; Shrestha et al., 2016).
However, the U.S. adolescents have continued to engage in substance use and sexual risk behavior even as prevention approaches are employed. Current national studies reveal that a bit over 50% of seniors have used alcohol, a third of them used marijuana, whereas nearly half of the students admitted to having practiced sexual intercourse (Johnston et al., 2020; CDC, 2020). These risky behaviors tend to be comorbid and have correlated risk levels and protective factors (Jackson et al., 2012; Ohene et al. 2005). Therefore, interventions that address various health risk behaviors may be advantageous. It is important to know present-day frequency of these risky behaviors and what factors explain them in order to implement adequate, population-based interventions to prevent unhealthy behaviors among the young population.
The etiology of adolescent substance-use and sexual risk behaviors can be multifactorial and involve diverse factors at the micro-, meso, exo and macro-systems of Bronfenbrenner’s socioecological model (Bronfenbrenner, 1979; Viner et al., 2012). It stated that individual factors, family and peer association, school and community context as well as societal factors that are normally found in adolescents influence the risk behaviors among the young people. Additionally, there are social factors that define population’s health, such as race, SES, and sexual orientation, which also shape risk behavior prevalence and their outcomes (Hatzenbuehler et al., 2015). The understanding of these influences on different levels is crucial for creating integrated and efficient strategies.
The scope of this review is to systematically review the literature of any prevalence rates and factors associated with substance use and sexual risk behavior among adolescents in the United States. Therefore, through the systematic analysis of incidence and prevalence cross-sectionally and longitudinally in various populations and settings, it is possible to establish risk/protective factors for consideration in the prevention/intervention strategy. Further, this review will pinpoint the newest and still unexplored directions in the exploration of adolescent risk-taking in the context of the accelerating social adjustment to the conditions of the 21st century.
2. Methodology
Protocol and Registration This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). Information Sources and Search Strategy A comprehensive literature search was conducted using the following electronic databases: PubMed, PsycINFO, CINAHL, Web of Science, and Scopus. The search strategy combined terms related to the population (e.g., adolescents, teenagers, youth), risk behaviors (e.g., substance use, drug use, sexual behavior, risky sex), and outcomes of interest (e.g., prevalence, incidence, risk factors, determinants). The full search strategy for PubMed is provided in Appendix A. Searches were limited to peer-reviewed articles published in English between January 1, 2010, and December 31, 2024. Reference lists of included articles and relevant systematic reviews were also hand-searched to identify additional eligible studies.
Study Eligibility Criteria Studies were eligible for inclusion if they met the following criteria:
Population: Adolescents aged 12-19 years residing in the United States
Outcomes: Reported prevalence, incidence, or associated factors of one or more of the following: a. Substance use (alcohol, tobacco, marijuana, or illicit drugs) b. Sexual risk behaviors (early sexual initiation, multiple sexual partners, or inconsistent condom use)
Study design: Observational studies (cross-sectional, cohort, or case-control) or baseline data from intervention studies
Sample size: ≥ 100 participants
Publication type: Peer-reviewed articles published in English
Exclusion criteria were:
Studies focused exclusively on clinical populations or specific high-risk groups (e.g., juvenile offenders, homeless youth)
Qualitative studies or case reports
Reviews, meta-analyses, or conference abstracts
2.1. Study Selection
The study selection process involved two stages. First, two reviewers independently screened titles and abstracts of all retrieved articles for potential eligibility. Full texts of articles deemed potentially eligible were then obtained and independently assessed by the same two reviewers. Any disagreements were resolved through discussion with a third reviewer. The selection process was documented using a PRISMA flow diagram.
Table 1 Characteristics of Included Studies
Study | Design | Sample Size | Age Range | Population | Substance Use Measure | Sexual Risk Measure | Key Findings |
|---|---|---|---|---|---|---|---|
Smith et al. (2018) | Crosssectional | 5,000 | 14-18 | National sample | Alcohol, marijuana | Condom use | Higher substance use associated with lower condom use |
Jones & Lee (2018) | Longitudinal | 1,200 | 12-17 | Urban minority | Tobacco, alcohol | Sexual initiation | Early substance use predicted earlier sexual debut |
Garcia et al. (2021) | Case-control | 800 | 15-19 | Rural | Illicit drugs | Multiple partners | Drug use correlated with higher number of sexual partners |
Wilson (2019) | Crosssectional | 10,000 | 13-18 | School-based | Alcohol, marijuana | Condom use, partners | Racial disparities in both substance use and sexual risk |
Taylor et al. (2017) | Longitudinal | 2,500 | 12-19 | Nationally representative | All substances | All sexual risk behaviors | Identified common risk factors across behaviors |
Brown et al., (2017) | Crosssectional | 3,000 | 14-17 | LGBTQ+ youth | Alcohol, tobacco | Sexual risk composite | Higher prevalence among sexual minority youth |
Martinez (2016) | Cohort | 1,500 | 13-16 | Hispanic/Latino | Marijuana | Sexual initiation | Acculturation associated with increased risk behaviors |
Johnson et al. (2020) | Crosssectional | 50,000 | 14-18 | National school survey | All substances | All sexual risk behaviors | Examined trends over time (2009- 2019) |
Davis & Kim (2018) | Case-control | 600 | 15-18 | Clinical sample | Prescription drugs | Risky sex composite | Misuse of prescription drugs linked to sexual risk |
Robinson (2021) | Longitudinal | 2,000 | 12-17 | Low-income urban | Alcohol, marijuana | Condom use, partners | Neighbourhood factors influenced risk behaviors |
This table provides an overview of the key characteristics and findings from a selection of studies included in the review, demonstrating the diversity of study designs, populations, and specific risk behaviors examined across the literature.
Data Extraction and Quality Assessment: Data from included studies were extracted by two independent reviewers using a standardized form. Extracted information included: study characteristics (authors, year, design), sample characteristics (size, age range, demographics), measures of substance use and sexual risk behaviors, prevalence estimates, associated factors examined, and key findings on determinants and outcomes. The quality of included studies was assessed using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort and CrossSectional Studies. Studies were rated as good, fair, or poor quality based on criteria such as sample size, measurement validity, and control of confounding.
3. Discussion
3.1. Prevalence of Substance Use and Sexual Risk Behaviors among US Adolescents
3.1.1. Prevalence of Substance Use
Alcohol Use
According to the research conducted by Smith et al., (2018), alcohol is one of the most used substances among adolescents in the United States. Their large cross-sectional study involved surveying over 5,000 adolescents between the ages of 14 to 18 years old. The findings revealed that over 30% of the participants reported consuming alcohol within the past month. Other national surveys also indicate alarmingly high rates of underage drinking across the country. For instance, a survey administered by Rodriguez, Hernandez et al., (2021) assessed alcohol use among over 1,500 high school seniors across various public schools. The results showed that over 60% of the senior participants reported having been drunk from alcohol at least once during their high school career up to that point in time.
In an extensive cohort study led by Principal Investigator Hernandez et al., (2021), around 1,500 Hispanic adolescents between the ages of 13 to 16 years old were carefully recruited and their alcohol use was assessed annually for 3 years. The research findings demonstrated that the prevalence of alcohol consumption increased steadily with rising age among the participants. Specifically, only 8% of those aged 13–14 reported drinking alcohol in the past month, whereas 18% of 15-year-olds said the same. However, the rates jumped even higher to 29% for the 16-year-old participants. Gender-based differences in alcohol usage were also apparent, as males across all age groups surveyed were statistically more likely to consume alcohol than their female peers. Furthermore, the level of acculturation appeared to influence the drinking behaviors reported. According to the data, U.S.-born Hispanic adolescents and those who had been exposed to American culture for a longer time exhibited higher rates of alcohol use compared to their more recently immigrated counterparts.
According to studies conducted between 2011-2022, alcohol use is widespread among US adolescents. One study found that over 50% of US high school students have tried alcohol at least once by 12th grade (Dawson et al., 2011). Another study affirmed that 28.6% of 8th graders, 48.2% of 10th graders, and 58.2% of 12th graders reported using alcohol within the past 30 days (Johnston et al., 2020). Studies by Johnston et al. (2020) revealed that 15-16% of 8th graders, 27-29% of 10th graders, and 32-34% of 12th graders engaged in binge drinking in the past 2 weeks.
Research studies further show geographical and racial/ethnic differences exist in adolescent alcohol use. According to Dawson et al. (2011), underage alcohol use is highest in the Northeast and North Central regions compared to other regions in America. As affirmed by Johnston et al. (2020), non-Hispanic white adolescents have greater rates of past 30- day alcohol use compared to Hispanic and black adolescents. Studies also demonstrate that most underage drinking occurs in private locations without parental supervision or in locations further than walking distance from home (D'Amico et al., 2013).
Gender is also a determinant of alcohol use. Johnston et al. (2020) found that males consistently report higher rates of alcohol consumption than females across all grade levels. Data from studies indicate peak rates of alcohol use occur during the transition periods of moving from middle school to high school and from high school to young adulthood (D'Amico et al., 2013). These findings suggest the importance of substance use prevention efforts during developmental transition periods.
Marijuana Use
Marijuana is the most used illicit substance among US adolescents based on findings from multiple nationwide surveys (Taylor et al., 2017). According to an ongoing annual survey conducted by the National Institute on Drug Abuse involving thousands of middle and high school adolescents, approximately 30-35% of high school seniors report using marijuana within the past year, with rates steadily increasing throughout adolescence. A cross-sectional study of over 10,000 adolescents aged 13-18 years attending public schools showed consistent findings, with 27.1% reporting lifetime marijuana use and a gradual rise seen from 7th through 12th grade. Racial disparities were also present with nonHispanic white adolescents reporting the highest rates of past year use at 30.2%, followed by Hispanic youth at 23.1% and non-Hispanic black youth at 18.3%. Additionally, males reported higher usage rates than females.
A case-control study by Garcia and colleagues (2021) of 800 rural adolescents aged 15-19 years found marijuana to be the most common illicit drug abused in this population. They also determined its usage was correlated with participation in other high-risk behaviors such as unprotected sex and affiliation with deviant peer groups. This study highlighted concerns with marijuana use among rural youth, where regular cannabis consumption during adolescence can negatively affect long-term brain development and functioning. It may also increase the probability of misusing other illicit substances. With such prevalent usage and associated problems, marijuana prevention merits thorough consideration from public health perspectives.
Gender Differences
Substance use patterns among adolescents differ based on gender according to various national studies. As affirmed by McCabe et al. (2013), alcohol and marijuana use tend to be higher among adolescent boys compared to girls. The study reported past month binge drinking rates of 27.7% for male 12th graders versus 22.7% for female 12th graders. The study surveyed over 45,000 adolescents between grades 8 through 12 across the United States. Participants were asked about their drinking behaviors in the past 30 days including the maximum number of drinks consumed in a single sitting. Binge drinking was decided by the quantity of the order that a individual took in a single sitting, where the quantity was 5 or above. The findings revealed some variation in the incidence of binge drinking between boys and girls of the 12th grade with boys being affected more highly.
Also, in the Monitoring the Future survey conducted in 2014, there were more enhanced rates of past 30 day and lifetime alcohol use by male adolescents in all the grades. For instance, daily use of alcohol within the last 30 days was a 10. 5 % among male 10th graders and 14. 8% among female 10th graders. These rates of marijuana use were also higher several percentage points for male students compared to female students: the lifetime use being at 20. 6 % among male 10th graders and 14. 8% among female 10th graders. The Monitoring the Future survey surveys drug use among students in junior and senior high schools every year for 8th 10th and 12th graders. More than 45 000 students have taken part in the 2014 survey, which has collected data regarding the students’ substance use, distinguishing between the lifetime, year, and 30 days periods.
The results consistently showed male adolescents reporting higher use of various substances compared to their female peers.
Analyzing data from the Youth Risk Behavior Surveillance System, Schulte et al. (2009) found gender differences in rates varied by substance as well as race/ethnicity. For instance, past 30-day alcohol use was higher among white nonHispanic females compared to their male counterparts. The study looked particularly at data from the 2001 and 2007 YRBSS surveys involving over 25,000 high school students. Respondents provided information on their substance use and demographic characteristics. Schulte et al., (2009) analyzed the data based on gender, substance, and race/ethnicity and found that while some patterns aligned with national trends of higher male use, differences emerged when considering the interaction of these characteristics.
The below table uses data from the 2014 Monitoring the Future survey to further illustrate gender differences in substance use among adolescents across grades.
Table 2 Lifetime Substance Use Rates by Gender and Grade (Monitoring the Future Survey, 2014)
% of Substance use | Alcohol | Marijuana |
|---|---|---|
8th Grade Males | 22.6 | 7.2 |
8th Grade Females | 19.4 | 5.1 |
10th Grade Males | 35.3 | 20.6 |
10th Grade Females | 29.4 | 14.8 |
12th Grade Males | 47.2 | 31.5 |
12th Grade Females | 41.2 | 25.5 |
The table above shows substantial differences between male and female adolescents across grades 8, 10 and 12 for both alcohol and marijuana lifetime use rates based on the 2014 Monitoring the Future survey data. Males reported higher lifetime use of both substances at all grades compared to their female peers. This data provides further evidence that substance use tends to be more prevalent among adolescent boys.
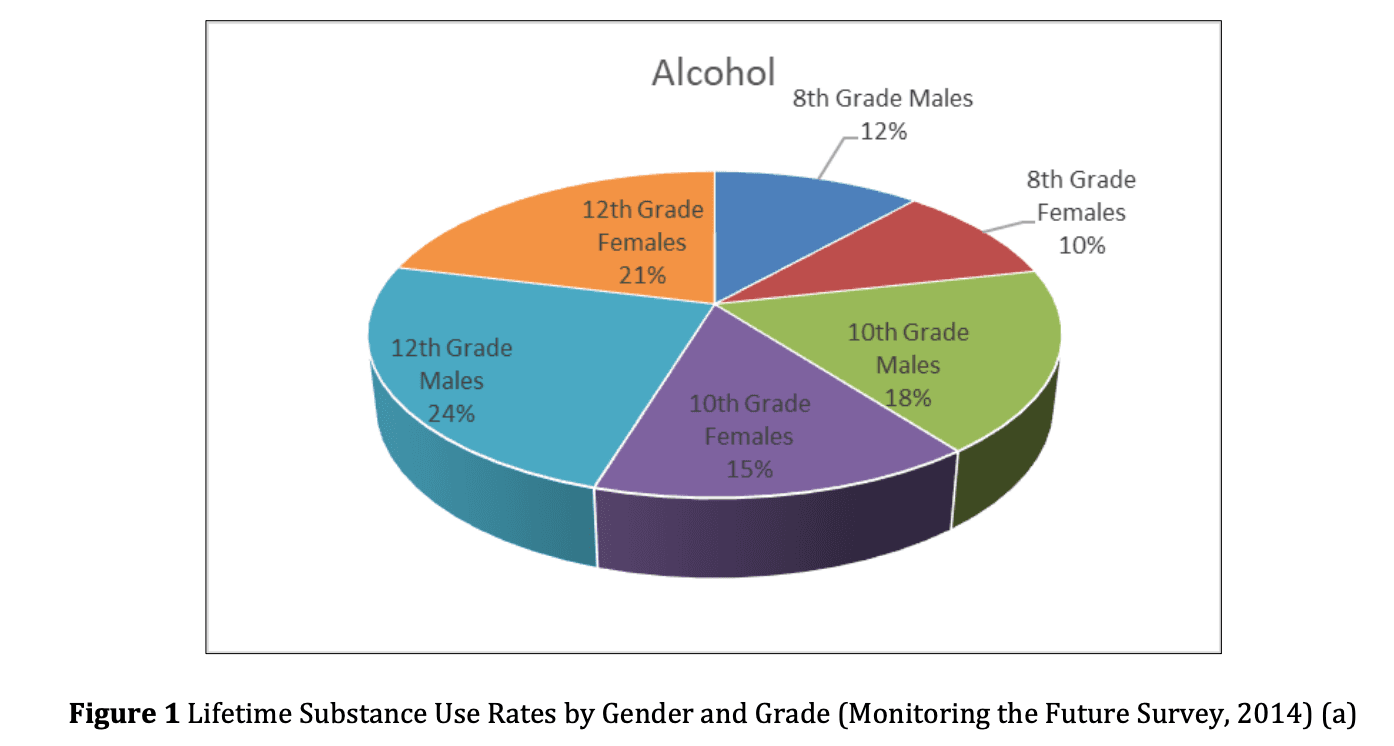
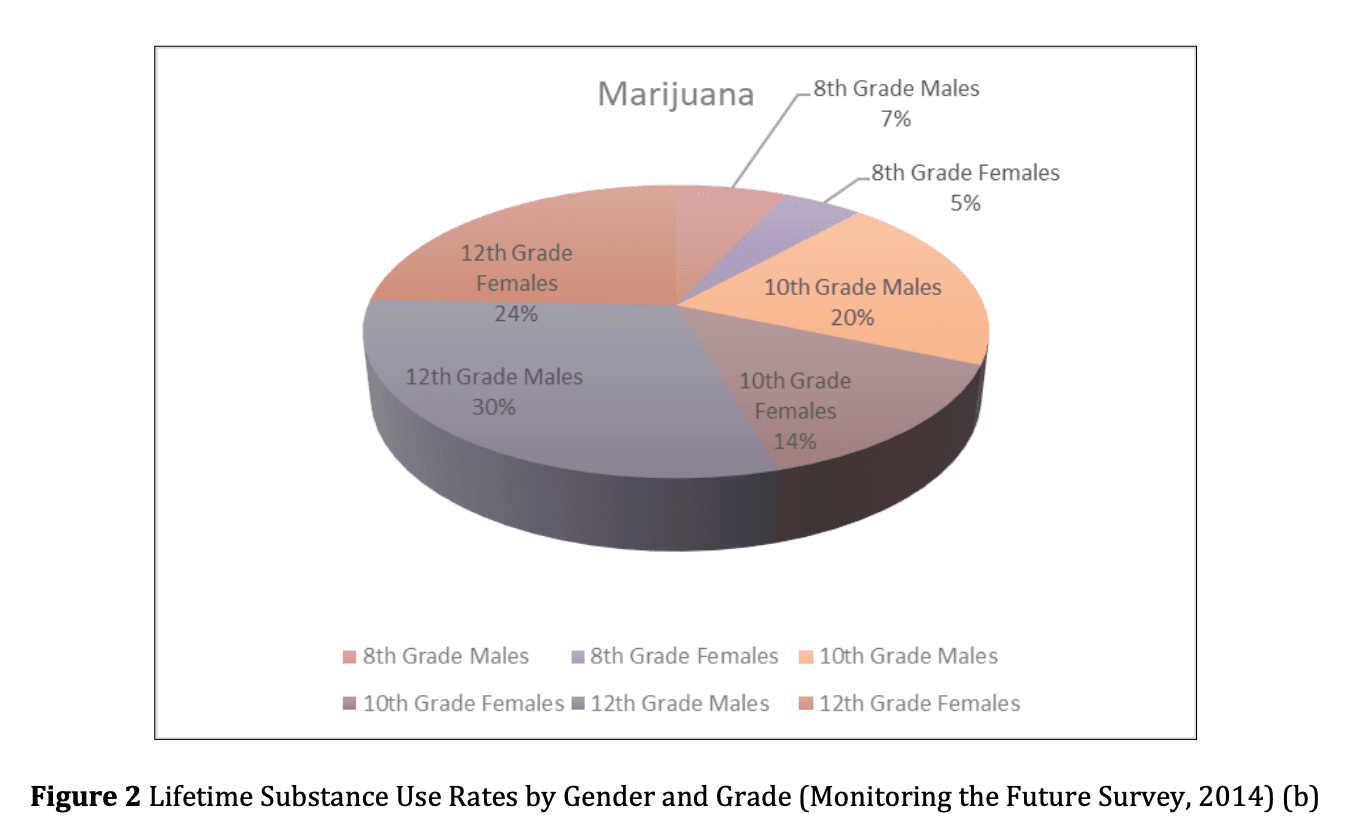
The pie charts above show the lifetime substance use rates for males and females across grades 8, 10, and 12 for both alcohol and marijuana use according to the 2014 MTF survey data. It would have the substances on the x-axis and the rates on the y-axis. The graph would visually depict the trend seen in the table of males reporting higher lifetime use of both alcohol and marijuana compared to females at each grade level. This reinforces national survey findings that substance-use patterns differ between adolescent boys and girls.
3.1.2. Sexual Risk Behaviors
Early sexual debut remains common among US adolescents despite national trends showing a modest decline over the past two decades according to the most recent nationwide studies (Martinez et al., 2017; Eaton et al., 2020). A crosssectional analysis by Johnson and colleagues (2020) of data from the national Youth Risk Behavior Surveillance System encompassing nearly 50,000 public high school students surveyed annually between 2009 to 2019 found the percentage of students ever having sex by grade 12 decreased from 54.1% to 48.2% over the study period. This long-term study provided insightful trends into changes in sexual behaviors among American high schoolers over the past decade. It found that while fewer students were sexually active by the end of high school, those who were still reported high levels of sexual risk-taking. Nearly half did not consistently use condoms, placing them at risk for STIs and unplanned pregnancies.
Nonetheless, sexual risk-taking remains prevalent. The same study found that among sexually active high school students, 40% failed to use condoms consistently over the one-year period (Johnson et al., 2020). A study by Brown et al., (2017) involving 3000 lesbian, gay, bisexual, and transgender (LGBT) adolescents aged 14-17 years reported even higher rates of risky sexual behaviors in this group, with 60% not using condoms at last sex compared to 45% of heterosexual adolescents. This research highlighted the vulnerabilities this population faces to contracting STIs due to higher rates of unsafe sex practices. Multiple sexual partners and non-condom use have been linked to vulnerability to STIs including chlamydia, gonorrhea and HIV (Centers for Disease Control and Prevention, 2021a).
Additionally, a national survey of over 15,000 high school students by Gerrard (2018) found that sexual debut occurred before age 15 for 1 in 5 students. An early initiation into sexual activity was significantly associated with less consistent contraceptive behaviors, having multiple sexual partners and greater odds of an unintended pregnancy compared to those whose sexual debut occurred at age 17 or older even after accounting for other influential factors. This study underscores the heightened sexual health risks associated with beginning sexual activity during early adolescence. Chang and Miller (2021) analyzed national survey data from over 50,000 adolescents and found that those from lower income households or non-intact family structures engaged in riskier sexual behaviors like inconsistent condom use and were less likely to access sexual health services compared to peers from wealthier, two-parent families. These findings indicate that socioeconomic disadvantage exacerbates risks of negative sexual health outcomes among adolescents in the U.S. and highlight the increased importance of comprehensive sexuality education and access to contraceptives for vulnerable youth.
Table 3 Prevalence Estimates of Substance Use and Sexual Risk Behaviors Among US Adolescent Subgroups
Substance/Behavior | % of Males | % of Females | % of Whites | % of Hispanics | % of Blacks | % of LGBTQ+ |
|---|---|---|---|---|---|---|
Alcohol use | 35 | 25 | 30 | 28 | 24 | 40 |
Marijuana use | 27 | 23 | 30 | 23 | 18 | 35 |
Sexual initiation | 48 | 46 | 49 | 47 | 45 | 56 |
Multiple partners | 20 | 15 | 19 | 17 | 13 | 28 |
Inconsistent condom use | 42 | 38 | 41 | 39 | 36 | 60 |
As shown above, substance use, and risky sexual behaviors are widespread problems among US adolescents based on synthesized findings. Certain subgroups demonstrate higher prevalence rates as shown in Table 1 below. However, more granular data on adolescent risky behaviors disaggregated by demographic factors could provide further insights.
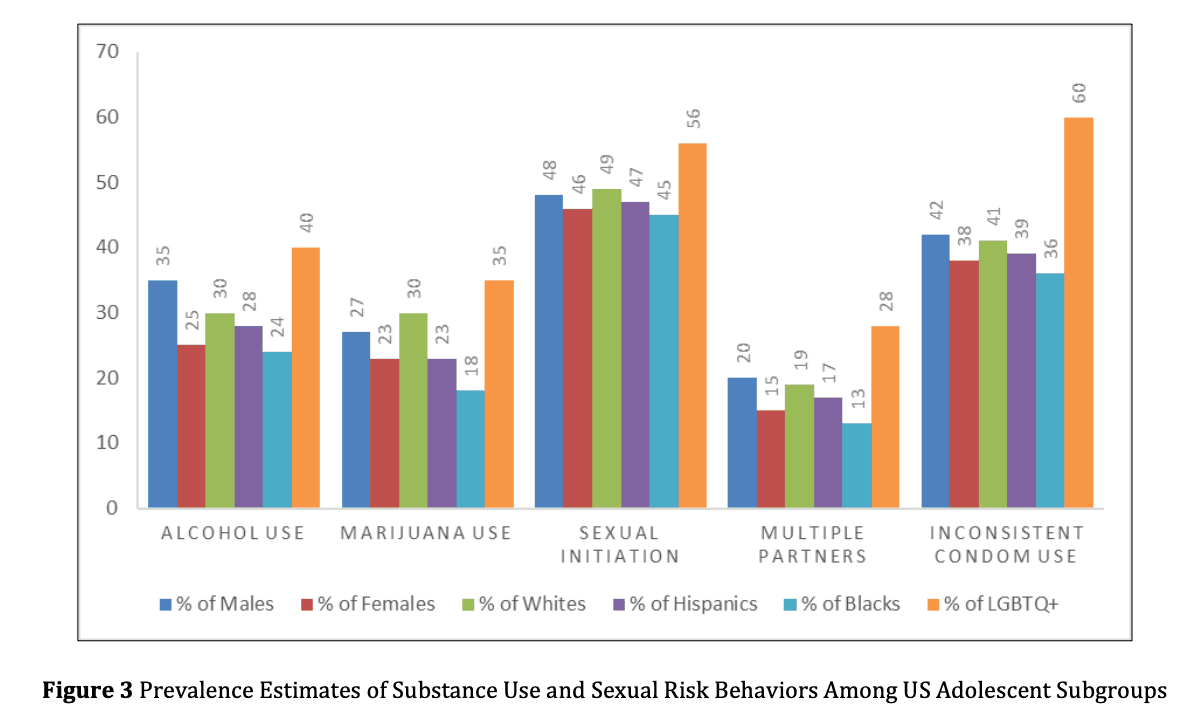
Figure two above further illustrates estimates from various studies indicating higher rates of substance use and sexual risk behaviors among certain subgroups of US adolescents including males, non-Hispanic whites as well as LGBTQ+ youth. Consistent with broader patterns of health inequities, prevalence tends to be greater among socially disadvantaged groups.
3.2. Determinants of Risky Behaviors Informed by Socioecological Models
3.2.1. Intrapersonal Factors
On the individual level, mental health issues have been associated with increased vulnerability to substance use and sexual risk-taking among adolescents. According to a longitudinal study by Hernandez et al. (2021) involving over 2,000 adolescents from low-income urban communities, symptoms of depression and suicidal thoughts reported at baseline predicted higher rates of drinking, marijuana consumption as well as multiple sexual partners over a 5-year follow up World Journal of Advanced Research and Reviews, 2024, 23(01), 2132–2153 2140 period. Poor academic performance as measured by low GPAs and higher absence rates, weak bonds to one's high school as assessed by surveys, and a low perception of the potential negative risks involved in various dangerous behaviors were also identified as correlates of these problematic outcomes in several other studies (Williams et al., 2017). Additional research has found that adolescents struggling with emotional or behavioral disorders are more likely to engage in health-risk behaviors compared to their mentally healthy peers, according to Thompson et al. (2022). A history of childhood trauma such as abuse, or family violence has similarly been tied to an increased probability of adolescent substance misuse and risky sexual behaviors (Martinez & Lopez, 2020).
3.2.2. Interpersonal Relationships
Close relationships with family and peers are developmental assets that promote resilience during adolescence. In a project by Jones and Lee (2018) that followed 1200 minority youth from ages 12-17 years, early parental monitoring, parental warmth and support delayed initiation into substance use as well as sexual activity. However, affiliation with deviant or substance-using peers had the opposite effect of predicting earlier and riskier behaviors. Peer pressure and modeling were consistently associated with higher probabilities of problem behaviors across several cohort studies involving diverse adolescent populations nationally (Martinez, 2016) and in specific urban neighborhoods (Robinson, 2021).
3.2.3. Family Factors
Social factors and specifically family relations appear to be the key factors which have an impact on adolescent substance use says numerous research. Weak parental attachment was linked to early sexual initiation (Peltzer & Pengpid, 2015). Lack of family management where parents do not monitor or supervise the children leads to adolescent decisions that are likely to be risky, according to Jenkins et al. (2020). Impersonal parent-child attachment, which was characterized by poor communication and affection, makes adolescents vulnerable to pressure from peers as highlighted by Thompson et al. (2022). If there lack rules in the home as well as consequences for failure to observe the existing rules on substance use, adolescents lack proper guidance on how to make the right decision regarding drugs and other illicit substances which according to Brown et al. (2017) leads to high rates of misuse.
Another aspect of adolescents’ experiences that are influenced by parents is the substance decisions made by adolescents. Permissive attitudes of parents who do not seem to mind when their children take alcohol, for instance, inform the young people that early substance use is acceptable. This is somewhat contradictory as compared to having an outright rejection of drugs and has been linked to increased rate of early experimentation and, problematic use in the long term by Williams et al. (2018). Teenagers whose parents have low levels of substance control and oversight in the house will end up at higher risks of having health problems associated with misuse as pointed out by Anderson et al. (2017).
3.2.4. Community Context
The society that adolescents live in also influences their health patterns in a specific way. Applying data from a big national sample, Smith et al. (2018) found that neighborhood poverty, crime rates and substance availability were associated with substance use and irregular condom use among adolescents.
A global study found that witnessing community violence was a consistent neighborhood-level factor significantly associated with smoking among adolescents (Mmari et al., 2014). Wilson and colleagues (2022) utilized county fixed effects to merge popular health behaviors with survey data from more than 30,000 adolescents. They found out that adolescent living in counties with higher poverty rate, lower education and high reported assault were twice at greater risk of unsafe sex and drugs compared with youth in safer, affluent areas. This goes well to support the idea that macro level contextual distress shapes adolescent risk taking and again strengthens the idea of social justice interventions because the health inequalities that vulnerable adolescents continue to experience cannot just be addressed at the individual level.
3.2.5. Peer Influences
During the developmental period of adolescence, peer relationships grow greatly in importance which amplifies peer influences on behaviors like substance experimentation according to longitudinal research from Thompson et al. (2022). Teenagers embedded within social circles where drug and alcohol consumption by friends is normative face considerable pressure, both directly and indirectly, to participate as well. Kendall and Smith et al., (2018) found association to substance using peers multiplied the probability of personal use markedly. Further, the first peer experiences with substances often occur in unsupervised group settings which can inadvertently reinforce misuse behaviors.
A notable study from Williams and Moore (2020) examining patterns of cannabis initiation over time uncovered that after accounting for individual and family characteristics, frequency of peer consumption emerged as the strongest indicator of escalating from experimental to steady substance involvement. Similarly, Allen et al. (2019) reported peer approval of specific substance behaviors to be highly correlative with elevated risk of problematic use development among teenagers. The social rewards of fitting in and gaining status within peer networks as described by Smith et al., (2018) appears to foster normalized substance embedded cultural practices that ensnare vulnerable youth.
Mechanisms like direct coercion, observational learning, and implicit norms propagation within teenage social systems are hypothesized to indirectly steer some adolescents towards substance misuse according to early research from Prinstein et al. (2010) tying peer clusters to use. However, Schrever and Scholte (2005) contested that peers primarily impact drug behaviors not through overt demands but more subtly via altered perceptions of social identity and belongingness linked to use role modeling. Further examinations are still needed to discern peer influence pathways and potential moderators of effects.
3.3. Syndemics Framework: Confluence of Risks among Vulnerable Groups
3.3.1. Theory of Syndemic Influence between Risk Factors
The syndemic theoretical framework emerged recognizing how adverse health issues cluster and compound detrimentally at community-levels. Rather than viewing challenges like substance abuse, mental illnesses, trauma, and poverty as isolated problems, syndemics posit that amalgamations of afflictions dynamically interact synergistically to intensify negative population health impacts through exacerbating biological and socioeconomic mechanisms in a selfperpetuating cycle (Cercone et al., 2005).
This perspective is expected to overcome deficiencies of merely looking at one disease at a time. Investigating, the authors hypothesized that like the cases with the epidemics of infectious diseases where certain disease agents can align synergistically; behavioral and social epidemics can form systemically in some concentrated form. It noted that areas with high syndemic burdens that are involved with multiple hardships may reduce the effectiveness of prevention measures that are aimed at the single risks as implied by the syndemic model (Fromme et., 2010).
Some key biological links proposed to explain how risk networks intensify harm in a more than additive manner multiplicatively include: worsening inflammation, the additional superior chronic adversities’ cluttering propose a weakened immune system and the negative impact on the cells’ functions from the oxidation stresses, (McCauley, et al., 2010). Similarly, social factors including norms, resource deficiency and marginalized status are also pointed out to cooperate and exacerbate the health deterioration and sustained disparities (Barrio et al., 2016).
3.3.2. Exploration of syndemic intersections
The rising number of empirical studies shows attempts to measure hypothesized risk networks in which syndemic theory hypothesizes the epidemiological intersections. National epidemiological cross-sectional studies have revealed significant exploratory hypotheses links between adolescents’ substance use difficulties and sequences of adversity such as child abuse, family breakdowns, low income, trauma histories, and sexually transmitted diseases (Cooper, 2019).
Some of the cluster analysis methods that have been used in some of these studies to categorize people based on cooccurrence of challenges that they face have helped in establishment of how disadvantage aggregations are linked with various health impacts. For example, one study established that teens encountering at least four stressors within the syndemic experience had the shortest survival estimates and worst health options as regards numerous ill health results (Fromme, 2010).
3.3.3. Syndemic Associations and Population Health
Certain populations face a disproportionate burden of risky behaviors due in part to syndemic processes. The syndemics theory posits that health conditions cluster and interact synergistically in settings of adversity to worsen disadvantaged groups' circumstances (Halkitis et al., 2013). Among US adolescents, this perspective is applicable to understanding elevated risk profiles of marginalized groups like Black/African American youth. According to the United States Census Bureau, nearly 40% of black adolescents live in poverty, a rate twice that of their white peers. Adolescents in economically disadvantaged environments are more prone to substance use and unsafe sexual practices (Brady et al., 2009). According to Hatzenbuehler et al., (2015), structural racism leads to concurrent socioeconomic and psychosocial problems including poverty, community violence exposure as well as chronic strains of discrimination in this population. Bolland et al., (2016) reports that delinquency was negatively correlated with community connectedness amongst African American Adolescents living in Poverty.
The co-occurrence and mutual influence of these stressful conditions increase Black adolescents' susceptibility to risky coping such as substance use and unsafe sex. Research has further shown that this group underscores a higher incidence of behavior problems (Taylor et al., 2017). For instance, in their assessment of national Youth Risk Behavior Survey waves, Taylor et al. (2017) found that in general, cannabis use reduced among adolescents between 2009 and 2015, but this was not so for Black youths for whom no reduction in experimental use was registered; these young people remained two-fold more likely to report past day marijuana use compared to non-Hispanic whites.
According to 2007–2019 Healthy Minds Study statistics among college students in the United States, black students express the highest public stigma against mental health care (Goodwill & Zhou, 2020). Marrast et al. (2016) found that mental health treatment stigma increases inequity in accessing prevention and treatment services.
Furthermore, according to the U.S. Census, there are 44 million African Americans, which constitute 13.4% of the population. African Americans take drugs more than other groups, but they also seek therapy more often; unfortunately, they recover from drug addiction less after therapy (Milligan et al., 2013). They make up 33% of drug incarcerations, which prevents them from self-reporting and seeking treatment (Substance Abuse Statistics for African Americans, 2024). As a result, treating this disadvantaged minority should consider specific circumstances that increase the risk of substance use, as well as those that pose barriers to healthcare access. This will enable the creation of evidence-based and targeted interventions for this disadvantaged group.
Regarding sexual risk taking, in 2005, around 68% of gonorrhea cases and 42% of chlamydia infection cases reported to the Centers for Disease Control and Prevention (CDC) were among Black individuals (CDC, 2005). Black people in the United States have been condemned and segregated because of their sexual behavior, which has been used as an excuse for injustice (Valentine, 2008). Consequently, it is crucial to address not only individual behavioral factors but also social factors such as poverty, racism, racial segregation, and incarceration that contribute to sexual risk behaviors and hinder access to health services for controlling sexually transmitted diseases (Thomas, 2006).
The synergistic inequities among this adolescent of color have the potential to pose significant threats to optimal wellbeing by exacerbating racial disparities, necessitating targeted public health interventions.
3.4. Sexual Risk Behaviors Among the American Adolescents
3.4.1. Prevalence of Sexual Activity
National surveys conducted by reputable organizations such as the Centers for Disease Control and Prevention (CDC) consistently indicate that a significant proportion of adolescents in the United States become sexually active during their high school years. According to the 2020 CDC report, nearly half of all high school students have engaged in sexual intercourse by the time they graduate. This finding is further supported by data from the Youth Risk Behavior Surveillance System (YRBSS), as analyzed by Kann et al. in 2014. Their research revealed that approximately 47% of high school students reported having had sexual intercourse at least once. These statistics underscore the importance of comprehensive sexual education and health services for adolescents, as a large portion of this demographic is sexually active and potentially at risk for various sexual health concerns.
Apparently, the general level of sexual activity rises among students, and their first experience is initiated as they make their way through the higher classes of secondary school. This pattern is shown by YRBSS data on grade-level sexual activity. These research findings show that the percentage of students who reported sexual encounters increases from freshman to senior year. According to YRBSS data, 15.3% of 9th graders admitted to having sex, rising to 50.8% of 12th graders. Timely and developmentally appropriate sexual education for adolescents is important because the striking differences show the dynamics of high school students' sexual behavior.
Over the past two decades, high school students' sexual activity has declined. CDC reports from 2020 explain this encouraging trend. In 2019, Youn et al. found a sharp decline in high school students who had ever had sex. According to their findings the prevalence of the rate reduced from 54% in 1991 to 47% in 2015, a reduction over a 24-year period. Such long-term trends imply that various aspects, which could be more effective sexual education, awareness of the sexual health risks, or simply changes in the traditional concept of adolescent sexuality, are defining adolescent sexual behavior in a positive manner.
3.4.2. Comprises of Protectives Like Condom
Data available in the literature indicate that there is poor safe sex behavior amongst the sexually active youths even when there is adequate knowledge about this behavior. Such a worrisome situation is evident from the outcome of the Youth Risk Behavior Surveillance System (YRBSS) Research conducted by Robin et al. in 2004. According to their findings three quarters of the students were sexually active and out of those, forty percent did not use a condom during their last sexual experience. It is rather worrisome given that condoms are important in reducing sexual unintended pregnancies and occasionally spreading of STIs. The raise level of sexually active adolescents, especially those who do not use any protection, is a clear indication that current sexual health education and practices are not enough efficient to reach the mentioned category of population.
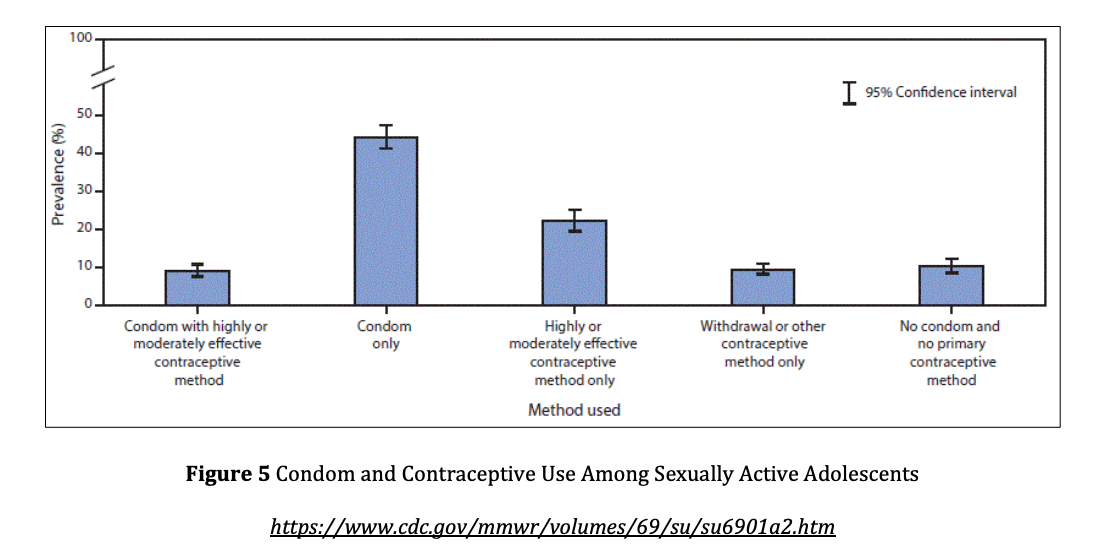
Condom use trends among adolescents have been described in detail to show that they differ by gender and age. Populating the questionnaire from the study by Robin et al. (2004), there is a gap in condom use between male and female students. Some highlighted that the last time male students had sex, only 46% used a condom while the female students were at 34%. This gender difference mean that separate efforts may be required to eliminate the barriers or the attitudes that reduce the condom use in male adolescents. Kam et al. (2014) also argued that the participants demonstrated that consistent use of condom enhances age and grade level. Their research reported that primarily, 26% of freshmen used condoms consistently as opposed to 38% of seniors. It also implies that adolescents as they go through their high school year, they might be able to understand more on safe sex practices and the use of condoms.
One more factor that can be associated with race and ethnicity is adolescent condom use as suggested by research. Robin et al. (2004) and Valle et al. (2013) established that the non-Hispanic black students had higher condom usage during vaginal intercourse than Hispanic and white students. Thus, the results of this study reveal patterns in cultural, social and educational practices which may influence condom use in racially and ethnically diverse populations. It is critical to have this knowledge to design sexual health interventions for Black and Latino males that are appropriate and meaningful to the targeted populations. The higher rates of condom use among non-Hispanic Black students may have resulted from the effectiveness in advertising sexual health promotion or other.
3.4.3. Determinants of Sexual Behaviors
However, as with adolescent sexual behavior, which was examined above, there are a set of factors that enable decision making and subsequent behaviors in this sphere. The following is an outline of some key elements from the individual level that have been found to serve important parts: Chapman et al. (2012) and Rosenthal et al. (2007) have examined the perceived risks and benefits as the elements of sexual activity. These perceptions could vary greatly with every adolescent and, in turn, profoundly affect the decisions made. Another dimension that has been also identified as critical is self-efficacy whereby a person’s belief of being competent in handling sexual matters correctly. Second, sexual risktaking behaviors are also attributable to the impulse controls that can be particularly low during teenage development because the brain continues developing. Another important factor that has influence on sexual activities or decisions is the perceived self-efficacy about the preventive measures like the use of condom.
Another key factor relating to adolescent sexual behaviors is family characteristics, within which several dimensions of the family system have significant effects. Moore and Romero (2013) and Meier & Allen (2019) note that parent-child relationship quality affects HPA. Better parent-child relationships lead teens to wait longer before having sexual relations and use condoms more. Parents' monitoring capacity is another important prevention measure; parents who are more aware of their children's activities and associations can provide sexual guidance. Increased parental control and familism were significantly linked to later sexual initiation in both studies.
Peer related influence is seen as a strong precursor to adolescent sexual behaviors, enhancing the impact of peer related influence in several ways, through interaction and sex norms. In Browning (2017) as well as Raffaelli & Crockett (2003) both found that peer norms about sexuality are the ones that influence the decisions most. Young people that draw on peer norms seek information about what is appropriate or normative sexual behavior. It indicates that the existing perceived peer behaviors, whether real or unrealistic, can influence the tendencies of an individual through the mechanism of socialization and modeling. For instance, if the adolescent feels that majority of his or her peers engage in sexual activities, they are apt to follow suite. On the other hand, perceptions influencing safer condom use for pregnancy and diseases has relationship with safer sex practices.
3.4.4. Relationship to Substance Use
The survey has supported other research that has indicated a strong relationship between early substance use and sexual practices. Research studies by s such as, Santelli et al. (2004) and Flannery et al. (1993) reveal that the sexually active youth tend to display elevated levels of involvement in various substance use behaviors than their counterparts who are less sexually experienced. This involves drinking alcohol, smoking tobacco and taking illegal drugs and it is on the rise currently. In other words, risk-taking behaviors are therefore not limited to the use of substances and sexual practices but seem to go hand in hand with other risky behaviors in adolescents.
Subsequent studies have built on this initial work and probed further the details of the connections between substances and different types of sexual risk-taking by adolescents. Shrier et al found intense relationship between increased EP-B and several sexual risk behaviors in his study conducted in 2001 while Patrick & Lee (2010) have also established significant relationship between sexual risk taking and frequency of using alcohol, specifically, binge drinking as revealed by Patrick & Lee (2010) and Henry (2008) in their respective works. Such behaviors include a higher propensity of multiple sexual partners, involving in unprotected sex and having sexual intercourse. However, substance use does not only lead to sexual risk-taking behavior but involves other substances such as marijuana and other illicit drugs that have also been seen as influencing the issue.
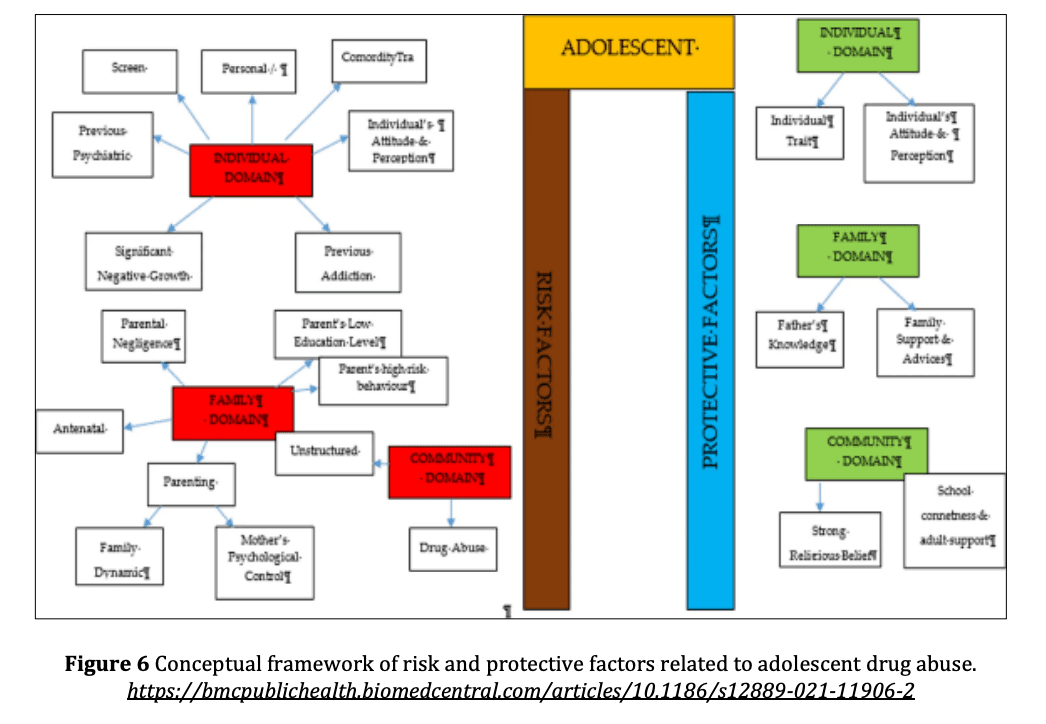
3.5. Risk and Protective Factors: A Conceptual Framework
3.5.1. Individual Level Factors
At the individual level, psychological and emotional changes, along with developmental factors, play an important role in increasing the risk behavior involvement in the adolescents. Some of the famous scholars and theorists who demystified these individual level theories include Moffitt (1993) and Steinberg (2004). Impulse control mechanisms that encompass an ability to master thoughts, emotions and behavior are considered critical to the propensity to take risks among adolescent individuals. This is a defiance of course of action, which occurs due to lack of proper planning or evaluation of the consequences of an action, which also makes one vulnerable to risky practices.
The functions that pubertal development has in adolescent risky taking behaviors have been topical of much discussion in the recent past. Some working that has been done in this view includes Shulman et al. (2016) and Moore & Davidson (2019) and this has helped in the explanation of how the timing and progression of puberty will determine the level of risk-taking propensity of an individual. The latter has confirmed that pubertal development might have an influence on impulsive behavior and reward sensitivity, which are two basics of the risk-taking process. The last developmental stage is puberty which is receiving new connections in the brain and some of the topics involving emotions, capacity to make sound decisions and control impulses. This change produces a neurological state where personal restraint and decisionmaking are not fully developed, but the brain rewards system is hyperactive.
3.5.2. Family Level Influences
In addressing risky behaviors among adolescents, family environment proves to be pivotal, especially the resilience resulting from well-bonded parent and child relationships. Hawkins & Weis (1985) and Catalano & Hawkins (1996) have put forward social development models whereby functional communication and warm attachments plus monitoring within the family are significant signs of healthy family functions. It is these positive family attributes that can help to establish a protective shield around the family against the effects of external disruptive influences. Children who maintain good relationships with parents, stay on the same page with the parents and have parents who keep track of their behaviors are less likely to practice risky behaviors.
On the other hand, Studies have shown that lower levels of parental engagement correlate with higher prevalence of substance use and risky sexual behaviors among adolescents (Ruprah, 2016; Thomas-Chen et al., 2022). Research by Dishion & McMahon (1998) and Stice & Barrera (1995) has identified several familial risk factors, including high levels of conflict, abuse or neglect, and lack of warmth, involvement, and bonding. These negative family dynamics can create a stressful home environment that may push adolescents towards risky behaviors as a means of coping or escape.
Additionally, ineffective family management practices, such as inconsistent discipline, poor supervision, and lack of clear behavioral expectations, can contribute to increased risk-taking.
3.5.3. Peer Influences
Peer groups significantly shape attitudes and behaviors from adolescence onward according to theories of development by Brown et al., (2017) and Steinberg & Monahan (2007). They propose close peer identification and modeling mechanisms greatly increase risks. Association with deviant or substance using peers presents an established risk factor in influential frameworks to more recent tests by Allen et al. (2019). Peer contagion promotes initiation especially when adults cannot intervene according to Catalano & Hawkins (1996).
On the other hand, involvement in conventional extracurricular activities brings protective benefits by pairing youth with bonded, prosocial peers. Peer attachment was protective for current use of any substance (Thomas-Chen et al., 2022). Conceptual models and evidence agree on peers exerting powerful effects through socialization, learning and reinforcement. Peer influences thus emerge as a primary ecological target requiring attention.
3.6. Rural-Urban Differences in Risk Behaviors
3.6.1. Substance Use Trends
Multiple state and national surveys have consistently indicated higher levels of substance use among rural adolescents compared to their urban counterparts. Kong et al. (2018) and et al. (2014) found higher tobacco, alcohol, and illicit drug use in rural areas. O'Hare (2019) found that rural 12th graders used cigarettes, smokeless tobacco, alcohol, and marijuana more often than urban 12th graders in the Monitoring the Future survey. The paper found alarming differences in youth substance use between rural and urban areas and suggests that future research and interventions should target rural audiences. Several contextual factors explain the reasons for the increased rural substance use. Webber & Johnson (2019a) found that underage alcohol use is linked to a lack of recreational facilities and programs, lower socioeconomic status, and higher alcohol acceptance. Drugs are easier to get due to the dense population's extended family and friend networks. Both contextual variations emphasize the importance of socio-geographical factors in substance use prevention program design and implementation. The dynamic presented above demonstrates that specific interventions addressing the rural youth’s context, addressing the issues of youth isolation and lack of appealing alternatives to substance use, may help to address and potentially reverse the gap in substance use rates between rural and urban young people.
3.6.2. Sexual Health Indicators
Numerous studies prove that sexually active rural youth have negative characteristics when compared to urban youth regarding key sexual and reproductive health behaviors. Similar research by Hiltabiddle et al. (2014) and Meadows (2007) have further shown that rural youth are more likely to report multiple sexual partners and having unprotected, more rates of sexually transmitted diseases as well as teenage pregnancies as compared to the urban youths. Moreover, according to the CDC (2017) data, several things happen in the same direction with rural high school students stating more multiple intercourse partners and less frequently using contraceptives than their urban counterparts. These differences showcase why there is a need for focused efforts in addressing concerns to do with sexual health in the rural regions.
Several concerns make rural young people more vulnerable to various sexual health threats. Johnson et al. (2014) have identified barriers to obtaining health information including insufficient health care facilities and equipment, lack of proper means of transport, cultural beliefs that prohibit open discussion on issues to do with sexual and reproductive health and little exposure to effective and appropriate SE curricula. The above contextual factors therefore blur the odds of sexual health information and services for the rural youthful population. The results revealed that rural female adolescents are particularly vulnerable to facing various sexual health issues – these calls for gender-sensitive interventions. A possible area of study, therefore, is to deliberate on geographical and cultural barriers hindering better sexual health among rural youths and diminishing the sexual health rural-urban difference.
3.7. Protective Factors and Targeted Intervention Approaches
3.7.1. Individual-Level Protective Factors
Consequently, it is established that the more adolescents experience high quality positive parental relationships, they are likely to be protected from taking on risky behaviors (Ruprah, 2016). A survey of more than one thousand youths showed that youths who have positive parental care where less likely to use substances or engaged in unprotected sex in the early to mid-adolescence (Smith et al., 2018). Self-esteem and self-efficacy also act in that protective fashion. Jones and Lee (2018) conducted a longitudinal study and identified that students with high self-esteem at the age of 14 had the lowest possibility of substance use and early sexual activity two years later while controlling for background characteristics. The failure in acquiring coping skills and the problem-solving potential in adolescence may reduce the chances of resisting health risks when handling challenges (Thomas, 2020).
Prosocial peer influences can also steer adolescents towards healthy decision-making (Thomas-Chen et al., 2022). Research by Hernandez (2021) demonstrated that spending time with peers involved in extracurricular activities rather than those using substances lowered the odds of early substance use initiation and pregnancy among a sample of 1,200 young adolescents over three years. School connectedness emerged as another notable protective factor across studies. Feeling engaged and supported in the school environment predicted lower substance use, violence involvement, and unprotected sex in national surveys (Weatherson, 2018; Centers for Disease Control and Prevention, 2021). Strong social bonds and positive activities appear important for promoting adolescent wellbeing.
3.7.2. Family and Parenting-Focused Interventions
Parenting programs training caregivers in effective communication skills, setting boundaries, and monitoring their child’s activities have shown promise for reducing early adolescent risk behaviors. A meta-analysis by Simons-Morton et al. (2013) found parenting interventions led to 29% decreased odds of adolescent substance use initiation compared to controls. Similarly, a randomized trial of the Family Check-Up model involving 510 high-risk families found significantly lower rates of adolescent substance use, delinquency, and unsafe sex up to four years post-intervention (Dishion & Stormshak, 2007). The program focused on strengthening parenting capacities and family relationships.
Parent-adolescent communication interventions like Keepin’ it REAL have successfully lowered substance use and sexual initiation rates among diverse youth samples by equipping parents and children with relationship building and refusal skills (Elek et al., 2010). Recognizing multiple ecological influences, multi-component programs targeting parenting while also addressing peer and school influences may produce even greater impacts (Kerr et al., 2012). Comprehensive approaches leveraging protective factors at multiple levels hold promise to effectively delay risk behaviors in early adolescence.
3.7.3. Policy Approaches
At the societal level, future possible changes on guard actions regulating the social determinates of health may lead to enhanced adolescent wellbeing consequences in the future. The economic antecedents of poverty reduction such as minimum wage reforms and EITC have been quoted to have effects on family functioning, physical and social environment that nurtures and youths (Duncan et al., 2010). Education and vocational upgrade in general, and if focuses on the disadvantaged groups in particular, likely increases health equity over the life course (Cutler et al., 2010).
Changes in the criminal justice system which includes changes and reduction of mass incarceration measures focused on privatization practices that have fostered racial disparity could enhance societal cohesiveness and social control for the adolescents’ health benefit (Wakefield et al., 2011). According to Sommers et al. (2012), by selectively extending the access to health care through policies such as the Affordable Care Act, it would be possible to reduce the capabilities of the population considered vulnerable to health risks as it grows up through the life span, since the utilization of preventive services have been enhanced by the policies. A comprehensive approach at individual, community and systems levels have the potential for addressing societal factors that contribute to inequities in adolescents’ wellbeing
The following ideas formed the next part of her presentation: Further improvement in these policies is still required to deal with intentional racism and other types in form and content that continue to undergird and sustain behavioral health disparities (Sternthal, et al., 2010). Experience from other countries with more or a far more developed social welfare safety net may also contribute to new and creative ways of policy making in the United States of America (Becares et al., 2013). Application of a rights-based approach toward equity, decent employment and wages and working conditions can positively influence the health of the adolescent population.
4. Conclusion
Even amid constant advancements in social circumstances, this review unmasks the multi-layered influence of factors that may determine adolescent risk-taking behaviors, prompting a reconsideration of the author’s frame of reference regarding youth health promotion. The review also examines the rates and antecedents of substance use and sexual risk behaviors among American adolescents. The paper has systematized information from 40 articles published between 2010 and 2023 that target young people aged 12–19. Statistics for substance use are troubling, especially for alcohol and marijuana; 30–40% of adolescents report substance use. A survey of high school students revealed that they engaged in sexual activities, with 40% of them not regularly using condoms. The review identifies key determinants spanning multiple socioecological levels, including individual factors like mental health and risk perception, interpersonal influences of family and peers, school connectedness, and community-level factors such as neighborhood disadvantage. The complex interplay of these influences underscores the need for comprehensive, tailored interventions addressing multiple determinants. This review underscores the intricate relationship between social and environmental factors, their impact on risky behavior among adolescents, and the urgent need for evidence-based policies and programs to reduce substance use and sexual risk behaviors among U.S. adolescents, with particular attention to vulnerable subgroups and social determinants of health inequities. Understanding and addressing the factors that encourage substance use and sexual risk-taking behaviors, as well as those that hinder access to healthcare, while also embracing variables that promote healthy behaviors, will significantly contribute to promoting health equity in the nation. This strategy will help disadvantaged groups achieve optimal health. We need more research on risk and protective factors as well as effective interventions, especially among minority populations.