Abstract
This study was designed to examine the prospective relations of perceived racial discrimination with allostatic load (AL), along with a possible buffer of the association. A sample of 331 African Americans in the rural South provided assessments of perceived discrimination from ages 16 to 18 years. When youths were 18, caregivers reported parental emotional support, and youths assessed peer emotional support. AL and potential confounder variables were assessed when youths were 20. Latent Growth Mixture Modeling identified two perceived discrimination classes: high and stable and low and increasing. Adolescents in the high and stable class evinced heightened AL even with confounder variables controlled. The racial discrimination to AL link was not significant for young adults who received high emotional support.
Studies have consistently documented racial disparities across numerous health outcomes, even among young people. Compared with members of other racial groups, African Americans experience aging-related chronic diseases earlier in life, at greater severity, and with more serious disease-related consequences (Schuster et al., 2012). According to life course and developmental perspectives, disproportionate disease risk among African Americans can be traced to systematic disadvantage and social inequities, starting at conception and continuing throughout childhood and adolescence (Priest et al., 2012). This is particularly true for African American youths growing up in the rural South. The socioeconomic risk factors that characterize this region include chronic, endemic poverty; lack of public transportation; limited occupational and educational opportunities; frequent housing adjustments in response to economic pressures; changes in employment status; interpersonal and institutional racism; difficulty in accessing medical care; and marginalization by healthcare providers (Hartley, 2004).
The health risk inequities that African Americans experience undoubtedly arise from more than class disadvantage. Psychosocial stressors that disproportionately impact African Americans have been proposed as a mechanism that increases their vulnerability to poor health. Consistent with this reasoning, an emerging line of research has focused on racial discrimination, a qualitatively unique source of psychosocial stress that African Americans face (Mays, Cochran, & Barnes, 2007; Pascoe & Smart Richman, 2009). Racial discrimination includes routine experiences with disrespect and treatment connoting that one is inferior or unintelligent; it continues to be pervasive in African Americans’ lives (Williams & Mohammed, 2009). Such experiences can be overtly racially motivated, or they can include more subtle instances of demeaning treatment in which intentions are less obvious. A hypothesis that has been proposed in the health disparities literature, but has yet to be examined empirically, is that exposure to racial discrimination during childhood and adolescence will have negative effects on the functioning of biological stress-regulatory systems and, ultimately, on health (Geronimus, Hicken, Keene, & Bound, 2006; Shonkoff, Boyce, & McEwen, 2009). The first purpose of this study was to address this issue by testing the hypothesis that high levels of perceived discrimination across adolescence will be associated with higher levels of wear and tear on biological systems, termed allostatic load (AL; McEwen & Stellar, 1993).
Perceived Discrimination and Allostatic Load
Recent theory and research suggest that coping with cumulative stressors elicits a cascade of biological responses that may be functional in the short term, but over time “weather” or damage the systems that regulate the body’s stress response. As the concept of allostasis emphasizes, the body achieves stability during stress through changes in multiple, interconnected systems. When these systems are repeatedly perturbed by stress, a biological toll, with potential implications for long-term health status, may be exacted. Some researchers consider AL to be a marker of this presumptive toll of chronic physiological stress. Often, AL is operationalized as a composite reflecting various mediators and outcomes of the stress response, including the sympathetic adrenomedullary system, the hypothalamic-pituitary-adrenal (HPA) axis, lipid metabolism, indices of inflammation, and immune functioning. Although specific components of AL vary somewhat among studies, researchers nevertheless have assessed the ways in which physiological systems as a whole are affected by socioeconomic, behavioral, social, and emotional factors (Kubzansky, Kawachi, & Sparrow, 1999). AL composites predict the onset of chronic diseases including hypertension, cardiac disease, diabetes, stroke, and all-cause mortality (Karlamangla, Singer, & Seeman, 2006).
Support for the first study hypothesis can be found in studies with African American adults. This research has demonstrated that exposure to racial discrimination is associated with a range of biological markers of stress, including neuroendocrine risk markers for poor birth outcomes (Hilmert et al., 2013), glucocorticoids (Mays et al., 2007), proinflammatory cytokines, and other markers of inflammation (Cooper, Mills, Bardwell, Ziegler, & Dimsdale, 2009). A recent study found that exposure to racial discrimination was associated with C-reactive protein (CRP), a measure of systemic inflammation, among African American adults (Lewis, Aiello, Leurgans, Kelly, & Barnes, 2010). Together, these studies support the importance of understanding the biological effects of exposure to racial discrimination during adolescence, a developmental stage during which youths may be particularly sensitive to race-related stressors.
Adolescence, Perceived Discrimination, and Allostatic Load
Adolescence is a critical developmental period in the life course that is characterized by numerous social, physical, and psychological changes. It is a time when youths began assigning greater value to their status within peer social networks and reduce their involvement with the family (Spear, 2000). This is also a stage during which African American youths are continuing to explore their racial identity (Spencer, 2006). Through this developmental process, youths come to understand the importance of their racial group membership to their thought processes, perceptions, feelings, and behavior. A complexity added to this normative process is the increase in minority youths’ contention with perceived racial discrimination, which may negatively influence developmental paths. Theoretical work suggests the importance of considering discrimination as a prominent environmental characteristic for minority youths that may place them at risk for negative outcomes (Swanson, Cunningham, & Spencer, 2003). The distress occasioned by demeaning messages inherent in discriminatory experiences during this developmental stage can exact a toll on physical and mental health (Williams & Mohammed, 2009). Thoits (1991) maintained that stressors threatening the central parts of an individual’s identity are likely to exert particularly pernicious influences. Thus, we expect that racial discrimination, a stressor that threatens both social standing and personal identity, will be particularly salient across adolescence. The challenges associated with low socioeconomic status (SES) and exposure to racial discrimination, coupled with the developmental nature of adolescence, is hypothesized to contribute to heightened levels of AL.
Emotional Support, Perceived Discrimination, and Allostatic Load
The present research also focused on buffering effects. Studies of adolescents have identified several buffering effects, defined as factors that reduce the impact of adverse experiences (Chen & Miller, 2012). For example, measures of family emotional support and of problem-solving skills have been shown to reduce the effect of life stress on outcomes such as adjustment, academic achievement, and drug use (Luthar, 2006). Evidence from several recent articles also suggests that parental emotional support may be a particularly influential source of buffering children’s and adolescents’ physiological stress reactions, capable of offsetting some of the risky hormonal, metabolic, inflammatory, and cardiovascular profiles that tend to develop following exposure to childhood adversity (Brody et al., 2013; Chen, Miller, Kobor, & Cole, 2011). Other recent research indicates that access to peer emotional support during adolescence has buffering properties that extend to physiological stress responses (Adams, Santo, & Bukowski, 2012). Exposure to life stress without peer support resulted in elevated physiologic stress responses, whereas having peer support attenuated the link. Together, these results support the proposition that access to family and peer support during adolescence has beneficial effects on the functioning of biological stress-regulatory systems and, ultimately, on health. It is thus plausible to predict that emotional support from parents and peers has a buffering effect for adolescents’ stressors, reducing the impact of perceived discrimination on AL.
Methodological Contributions
This study was also designed to address two methodological issues. First, we ruled out several alternative explanations for the hypothesized contribution of perceived discrimination to AL by statistically controlling for demographic and biobehavioral confounders. Few, if any, studies to date have included these controls. The demographic confounder was cumulative SES risk, because it has been found to be associated with AL levels among both African American and Caucasian adolescents (Brody et al., 2013). The biobehavioral confounders were perceived life stress, depressive symptoms, and unhealthy behaviors. Perceived discrimination is associated with depressive symptoms during adolescence (Brody et al., 2006), and both depression and AL reflect neurobehavioral adjustments to stress (Karlamangla et al., 2006). Similarly, perceived racial discrimination is associated with perceived life stress among rural African American adolescents (Brody et al., 2012), rendering attributions about the unique contribution of discrimination to AL somewhat ambiguous if more general life stress is not statistically controlled. Finally, perceived discrimination has been linked to indicators of unhealthy behaviors, including poor diet, lack of sleep and exercise, and the use of alcohol and other drugs (Pascoe & Smart Richman, 2009). Self-medication theories suggest that individuals coping with discrimination may use alcohol and other drugs and choose poor-quality foods for short-term relief from stress (see Sinha, 2008).
A review of previous longitudinal studies of adolescent-perceived discrimination among rural (Brody et al., 2011; Brody et al., 2006; Simons, Chen, Stewart, & Brody, 2003; Simons et al., 2006) and urban (Greene, Way, & Pahl, 2006) African American youths indicates a considerable amount of heterogeneity in both levels of perceived discrimination and its change across time. Thus, an additional methodological contribution of this study was to determine whether perceived discrimination is best characterized by multiple, distinct trajectories. Recent statistical advances allow empirical analysis of the underlying data heterogeneity, which would otherwise be treated as error (Del Boca, Darkes, Greenbaum, & Goldman, 2004). Latent Growth Mixture Modeling (LGMM) has emerged as a strong methodology for the study of homogenous trajectories in a larger heterogeneous sample. Tests using LGMM can determine whether a population is composed of a mixture of discrete classes of individuals with differing growth profiles. Based on the heterogeneity observed in other studies with rural and urban African American adolescents, we expected that a single continuous distribution would be unlikely to represent fully adolescents’ experiences with discrimination. Instead, we hypothesized that a multiple trajectory model would better fit the data. Specifically, we hypothesized that perceived discrimination would be characterized by more than one class across the ages of 16 to 18 years, and that youths who perceived more discrimination would evince higher AL at age 20 years. Both of these perspectives are based on the concept that more frequent perception of discrimination, a salient stressor in the lives of African American adolescents and adults, would result in more frequent activations of biological responses to stress, leading to wear and tear on bodily systems and higher AL. This hypothesis was derived from allostasis theory (Goodman, McEwen, Huang, Dolan, & Adler, 2005) and the weathering hypothesis (Geronimus et al., 2006), both of which propose that chronic exposure to high levels of salient stressors and the challenges they present forecast high AL.
Method
Sample
We tested our hypotheses using data from the Strong African American Families Healthy Adolescent Project. African American primary caregivers and a target youth selected from each family participated in annual data collections; youths’ mean age was 11.2 years at the first assessment and 20.2 years at the last assessment. Of the youths in the sample, 53% were female. At baseline, 78% of the caregivers had completed high school or earned a general equivalency diploma. The families resided in nine rural counties in Georgia, in small towns and communities in which poverty rates are among the highest in the nation and unemployment rates are above the national average (Proctor & Dalaker, 2003). At the first assessment, the primary caregivers in the sample worked an average of 39.4 hours per week; nevertheless, 46.3% lived below the federal poverty standards with a median family income per month of $1,655. At the last assessment, the proportion was 49.1% with a median income of $1,169. The increase in the proportion of families living in poverty and the decrease in family income over time may have resulted from the economic recession that was occurring during 2010. Overall, the families can be characterized as working poor.
At the first assessment, 667 families were selected randomly from lists of fifth-grade students that schools provided (see Brody et al., 2013, for a full description). From a sample of 561 at the age 18 data collection (a retention rate of 84%), 500 emerging adults were selected randomly to participate in the assessment of AL. Costs associated with the assessment of AL necessitated the drawing of a subsample. From the subsample, 398 participated in the collection of AL data at age 20. The current study thus was based upon the 331 participants (114 men and 190 women) who agreed to participate in the assessment of AL at age 20 and had provided data on all study measures from ages 16 to 20. At the beginning of the current study when the youths were age 16, 50.4% of them lived in single-mother-headed households; 27.3% lived with their biological mothers and fathers; 13.0% lived with their biological mothers and stepfathers; 5.2% lived with grandparents; and 4.2% lived with other guardians. Comparisons with participants who did not provide AL or complete all study measures did not reveal any significant differences on any variables. To further assess attrition bias, we used Heckman’s (1979) two-step procedure to estimate sample selection bias. The inverse Mills ratio was not significant, and including this parameter in our models did not change the findings.
Procedures
Perceived discrimination was measured when the youths were 16, 17, and 18 years of age. Protective parent and peer relationships were assessed when the target youths were 18, and AL and the control variables were measured when the target youths were 20 years of age. All data were collected in participants’ homes using a standardized protocol. One home visit that lasted approximately 2 hours was conducted by two African American field researchers at each wave of data collection. Interviews were conducted privately, with no other family members present or able to overhear the conversation. Informed consent was obtained at each data collection wave. Participants were told that the purpose of the study was to identify the predictors of health and well-being among rural African American adolescents. They were compensated $100 at each wave of data collection. At each wave, primary caregivers consented to minor youths’ participation in the study, and minor youths assented to their own participation. Youths age 18 and older consented to their own participation.
Measures
Allostatic load
The protocol for measuring AL when youths were 20 years of age was based on procedures developed for field studies involving children and adolescents (Evans, 2003). Resting blood pressure was monitored with Dinamap Pro 100 (Critikon; Tampa, FL) while the youth sat reading quietly. Three readings were taken every 2 minutes, and the average of the last two readings was used as the resting index. This procedure yields highly reliable indices of chronic resting blood pressure (Kamarck et al., 1992). Overnight urine samples were collected for assays of catecholamines and cortisol. Beginning on the evening of data collection, all urine that a youth voided from 8 p.m. to 8 a.m. was stored on ice in a container with metabisulfite as a preservative. Total volume was recorded, and four 10-ml samples were randomly extracted and deep frozen at −80° C until assays were completed. The pH of two of these samples was adjusted to 3 to inhibit oxidation of catecholamines. The frozen urine was delivered to the Emory University Hospital medical laboratory in Atlanta, Georgia, for assaying. Total unbound cortisol was assayed with a radioimmune assay. Epinephrine and norepinephrine were assayed with high-pressure liquid chromatography with electrochemical detection. Creatinine was assayed to control for differences in body size and incomplete urine voiding. CRP, a biological marker of systemic inflammation, was assayed from a blood sample. After blood was drawn into serum separator tubes by certified phlebotomists, it was frozen and delivered to the Psychiatric Genetics Lab at the University of Iowa for assaying. Phlebotomists went to each participant’s home to draw the blood. Serum levels of CRP were determined using a Duo Set Kit (DY1707; R&D Systems, Minneapolis, MN) according to the manufacturer’s directions. A normal concentration of CRP in healthy human serum is usually lower than 10 mg/L. No participants had CRP levels outside the normal range. Because CRP is characterized by a skewed distribution (skewness = 1.90, kurtosis = 2.94), we applied a log transformation to normalize the readings (skewness = 0.91, kurtosis = −0.31 after the transformation).
AL was calculated by summing the standardized scores of seven indicators: overnight cortisol, epinephrine, and norepinephrine; resting diastolic and systolic blood pressure; CRP; and body mass index (BMI; weight in kilograms divided by the square of height in meters). Prior studies of AL in adults (Karlamangla et al., 2006), children (Evans, 2003), and adolescents (Brody et al., 2013) used similar metrics, combining multiple physiological indicators of risk into a total AL index.
Perceived discrimination
Participants responded to nine items from a version of the Schedule of Racist Events (SRE; Landrine & Klonoff, 1996) revised for use with adolescents (Brody et al., 2006). Items in the revised SRE assessed the frequency during the previous year, ranging from 0 (never happened) to 2 (happened a lot), with which the respondent perceived specific discriminatory events such as racially based slurs and insults, disrespectful treatment from community members, physical threats, and false accusations from business employees or law enforcement officials. Responses were summed to form the perceived discrimination scale, ranging from 0 to 18. Coefficient alpha for the scale was .87 at age 16, .88 at age 17, and .89 at age 18. Means and standard deviations were M = 3.62, SD = 3.53 at age 16; M = 5.05, SD = 4.44 at age 17; and M = 5.52, SD = 4.59 at age 18.
Emotional support
The measure of emotional support included assessment of parent and peer support. Each youth’s primary caregiver responded to the 11-item Family Support Inventory (Wills, Blechman, & McNamara, 1996) at the age 18 data collection. Caregivers reported their instrumental and emotional support on a scale ranging from 1 (not at all true) to 5 (very true). Example items include, “If my child talks to me I have suggestions about how to handle problems,” and “If my child needs help with school or work, she/he can ask me about it.” Cronbach’s alpha for the scale was .94. Peer support was measured using a 4-item subscale from the Carver Support Scale (Carver, Scheier, & Weintraub, 1989). Youths reported on the amount of support their peers provided to them in dealing with problems; example items include, “I get emotional support from my peers,” and “I get sympathy and understanding from my peers.” The response set for these items ranged from 1 (not at all true) to 5 (very true). Cronbach’s alpha was .95. These scales were standardized and summed to form a composite measure of protective emotional support. Nunnally’s (1978) reliability coefficient for composite variables was .97.
Confounder variables
To account for variables that could provide plausible rival explanations, all analyses controlled for cumulative socioeconomic risk, perceived stress, depressive symptoms, and unhealthy behavior at the age 20 data collection. Cumulative socioeconomic risk was defined as the sum of six socioeconomic risk indicators: family poverty as assessed using United States government criteria (an income-to-needs ratio ≤ 1.5), primary caregiver noncompletion of high school or an equivalent, primary caregiver unemployment, single-parent family structure, family receipt of Temporary Assistance for Needy Families, and income rated by the primary caregiver as less than adequate to meet all needs. Perceived stress was measured using six items from the Life Stress subscale from the MacArthur Reactive Responding Scale (Taylor & Seeman, 1999). Example items include, “I often feel overwhelmed by all that I have to do” and “I often don’t feel on top of all that needs to be done.” The response set ranged from 1 (strongly agree) to 5 (strongly disagree). Scores were reverse coded and summed to form a measure of perceived life stress, with high scores representing high levels of stress. Cronbach’s alpha was .65. Depressive symptoms at age 20 were assessed with the 20-item Center for Epidemiologic Studies Depression scale (CES-D; Radloff, 1977), a self-rated measure of symptoms occurring during the previous week. The response set ranged from 0 (rarely or none of the time, less than 1 day) to 3 (most of the time, 6–7 days). This scale has been well validated and widely used to measure depression in community samples. Cronbach’s alpha was .84. In this sample, 32.6% of the participants scored at or above the cutoff score of 16, indicating clinically significant levels of depressive symptoms. Unhealthy behavior was indexed using items from the Youth Risk Behavior Survey (YRBS; Youth Risk Behavior Surveillance System, 2009). This scale has been used in several national, ethnically diverse surveys and has shown good validity and reliability. Participants reported how often during the past 7 days they consumed fruit, vegetables, 100% fruit juices, and milk. The response set ranged from 0 (none) to 7 (4 or more times a day). Exercise was measured with a single item: “During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” The response set ranged from 0 (0 days) to 7 (7 days). The nutrition and exercise items were reverse coded so that higher numbers indicated unhealthier behaviors. Several items indexed substance use. Respondents reported the number of days during the past month on which they had smoked cigarettes, had a drink of alcohol, or had 5 or more drinks of alcohol within a couple of hours. The response set for all three items ranged from 0 (0 days) to 7; for smoking and drinking, 7 was labeled (every day), whereas for having 5 drinks, it was labeled (20 or more days). Respondents also reported the number of occasions during the past month on which they used marijuana, ranging from 0 (0 times) to 6 (40 or more times). The indicators were standardized and averaged to form the composite unhealthy behavior measure. Reliability for this measure was .94.
Plan of Analysis
The data analyses were composed of three steps. First, we executed a univariate latent single-class growth model (LGM) to facilitate model specification for the execution of an LGMM. Second, LGMM was executed to identify discrete classes of adolescents with qualitatively different perceptions of discrimination across adolescence. Third, qualitatively different classes of perceived discrimination were used in linear regression analyses, along with protective emotional support, to test the stress-buffering hypothesis. Descriptions of each of these analytic steps follow.
When three waves of data are available, LGM uses these data points to determine a within-individual change in a construct (e.g., perceived discrimination; Singer & Willett, 2003). Applied to this study, LGM fits an ordinary least squares (OLS) regression line to the three data points for perceived discrimination for each adolescent. The regression lines described the growth or change in perceived discrimination for each adolescent across the course of the study. The intercept for each adolescent represents his or her level of perceived discrimination at the starting point, age 16. The slope of each line indicates the rate at which perceived discrimination changed across the three waves of data collection. The LGM calculates the mean and variances for the intercept of perceived discrimination (value at age 16) as well as the mean for the slope of perceived discrimination (values across ages 16, 17, and 18). If the intercept and slope evince significant variation, an LGMM will be executed to identify discrete classes of perceived discrimination.
LGMM determines whether the population under study is composed of a mixture of discrete classes of individuals with differing profiles of growth (i.e., different intercepts and slopes of perceived discrimination). Based on the heterogeneity observed in our previous studies of perceived discrimination among rural African American children, preadolescents, and adolescents, we hypothesized that a single continuous distribution would be unlikely to represent fully individuals’ perceptions of racial discrimination. Instead, we hypothesized that a multiple trajectory model would better fit the data. To do this, comparisons of model fit among 1-to-3 class LGMMs were evaluated. Comparisons of model fit assessed relative fit with conventional indices, including Bayesian (BIC), entropy values, and the Lo-Mendell-Rubin adjusted likelihood ratio (adjusted LRT; Lo, Mendell, & Rubin, 2001). We sought a model with lower entropy values for the criterion indices.
As a test of the primary study hypotheses, three linear regression models were executed. The first model was designed to examine the association between perceived racial discrimination classes across ages 16 to 18 and AL at age 20. The second model included the confounders to rule out their contributions to any prospective associations between perceived discrimination classes and AL that the first model might reveal. The third model was executed to estimate the main effect of protective emotional support and the hypothesized interaction of perceived racial discrimination classes with protective emotional support in forecasting AL at age 20. All interaction analyses were executed based on the conventions that Aiken and West (1991) prescribed, whereby the risk variable is first mean centered and interactions are calculated as the product of the centered variable and other study variables.
Results
Descriptive Associations
Table 1 presents the correlations, means, and standard deviations for AL, perceived discrimination, emotional support, and the confounder variables. Significant, positive associations emerged among classes of perceived discrimination, AL, depressive symptoms, and perceived stress. High and stable levels of perceived discrimination across adolescence forecast heightened AL, elevated levels of depressive symptoms, and heightened perceived stress at age 20. Receipt of emotional support was associated with low levels of depressive symptoms and perceived stress. AL was not associated with any of the confounder variables. Table 2 presents the correlation matrix, means, and standard deviations for the measures that constitute AL at age 20. Cortisol was positively associated with epinephrine and norepinephrine, and it was negatively associated with CRP. Thus, stress hormones from the sympathetic nervous system and HPA axis were correlated, with higher levels of cortisol associated with lower levels of CRP, which is an indicator of systematic inflammation and immune function. Epinephrine, but not norepinephrine, levels were negatively associated with BMI and CRP. Diastolic, but not systolic, blood pressure was positively associated with BMI and CRP.
Table 1
Correlations Among Study Variables
Study Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
1. Allostatic load | -- | |||||||
2. Discrimination class a | .113 | -- | ||||||
3. Emotional support | −.036 | .004 | -- | |||||
4. Gender (male = 1) | .046 | −.033 | −.183 ** | -- | ||||
5. Depression | −.030 | .178 ** | −.157 ** | −.098 | -- | |||
6. Perceived stress | .032 | .191 ** | −.153 ** | −.004 | .510 ** | -- | ||
7. SES-related risk | .088 | −.068 | −.019 | −.018 | .002 | .065 | -- | |
8. Unhealthy behaviors | −.058 | .025 | −.127 * | .137 * | −.195 ** | .151 ** | .001 | -- |
Mean | −0.065 | 0.215 | 0.000 | 0.430 | 13.378 | 14.961 | 2.644 | −0.006 |
SD | 3.438 | 0.411 | 0.742 | 0.495 | 8.050 | 4.042 | 1.597 | 0.604 |
Note. N = 331. SES = socioeconomic status.aHigh and stable = 1, low and increasing = 0.*p ≤ .05, two-tailed.**p ≤ .01, two-tailed.
Table 2
Correlations Among Indicators of the Allostatic Load Index
Study Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
1. Allostatic load | -- | |||||||
2. Cortisol | .366 ** | -- | ||||||
3. Epinephrine | .339 ** | .140 * | -- | |||||
4. Norepinephrine | .481 ** | .341 ** | .353 ** | -- | ||||
5. Diastolic BP | .641 ** | −.039 | −.007 | .014 | -- | |||
6. Systolic BP | .605 ** | .048 | .068 | .005 | .664 ** | -- | ||
7. BMI | .586 ** | −.061 | −.134 * | .075 | .325 ** | .201 ** | -- | |
8. Log of CRP | .458 | −.125 * | −.157 ** | −.067 | .229 ** | .079 | .592 ** | -- |
Mean | −0.065 | 5.491 | 8.253 | 38.095 | 74.147 | 114.073 | 28.350 | 0.695 |
SD | 3.438 | 3.646 | 12.426 | 32.952 | 9.606 | 11.914 | 8.270 | 0.685 |
Note. N = 331. BP = blood pressure. BMI = body mass index. CRP = C-reactive protein.*p ≤ .05, two-tailed.**p ≤ .01, two-tailed.
Latent Growth Modeling of Perceived Discrimination
Using LGM, we tested the hypothesis that adolescents’ perceptions of discrimination would increase over time; the results supported the hypothesis. The slope parameter was positive and significantly different from zero (mean = .784, p < .0001), indicating the average slope increased between ages 16 and 18 at a rate of .784 points every year. More importantly, the analysis indicated significant variation in the intercept (variance = 10.39, p < .0001) and the slope (variance = 2.171, p < .001), suggesting robust individual differences in trajectories of perceived racial discrimination. Given these findings, an LGMM was executed to identify different classes of trajectories across adolescence of perceived racial discrimination.
Latent Growth Mixture Modeling of Perceived Discrimination
The fit statistics for the 1-to-3 class LGMM solutions are summarized in Table 3. As depicted in Table 3, the analysis showed that, although the 3-class model evinced the lowest BIC statistics, entropy indicated that the 2-class model fit the data better than did the 3-class model. In addition, the Adjusted LRT also suggested the 2-class model fit the data significantly better than did the 1 and 3 class models. The 2-class model was therefore chosen to characterize discrete trajectories of perceived racial discrimination across adolescence among rural African Americans. Figure 1 depicts the average trajectories for each class of perceived discrimination. The majority of participants (78.5%) were assigned to a class with a relatively low intercept at age 16 that increased significantly from ages 16 to 18. The intercept of perceived discrimination was approximately 2. We refer to this class as low and increasing. The second group, which comprised 21.5% of the study sample, evinced a high and stable level of perceived discrimination across adolescence. This group had a much higher intercept of perceived discrimination at age 16; the starting point for this group was 8, nearly 4 times higher than for the first group. We refer to this class as high and stable.
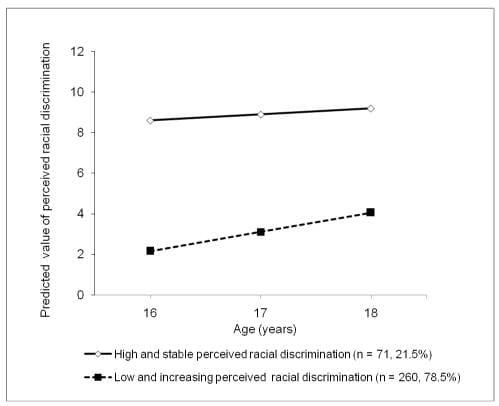
Figure 1
The estimated mean scores for each class of perceived racial discrimination.
Table 3
Results for Model Selection
Lo-Mendell-Rubin Adjusted Likelihood Ratio Test | Proportion of Individuals in Class | |||||||
Likelihood | BIC | Entropy | 2 Log Likelihood | p | 1 | 2 | 3 | |
One class | −3467.68 | 6983.99 | -- | -- | -- | 1.00 | ||
Two class | −3427.23 | 6921.34 | .81 | 76.69 | .01 | .21 | .79 | |
Three class | −3409.87 | 6904.85 | .77 | 33.93 | .37 | .16 | .18 | .66 |
Note. BIC = Bayesian index.
Tests of the Study Hypotheses
The regression models that address the study questions are presented in Table 4. Adolescents in the low and increasing class of perceived discrimination were assigned a 0; those in the high and increasing class were assigned a 1. Model 1 in Table 4 tested the study hypothesis that high and stable levels of perceived discrimination across adolescence would forecast AL at age 20. This hypothesis was supported [b = 0.923, 95% CI (0.027, 1.819), p < .05]. The analysis presented in Model 2, Table 4 adds confounder variables to the analysis depicted in Model 1, Table 4. As hypothesized, with the confounder variables controlled, perceptions of high and stable levels of discrimination forecast higher AL levels at age 20 [b = 1.088, 95% CI (0.177, 1.999), p < .05].
Table 4
Regression Models of the Results of Perceived Racial Discrimination and Emotional Support Using Allostatic Load at Age 20 Years as the Outcome
Allostatic load at age 20 years | |||
Model 1 | Model 2 | Model 3 | |
b [95% CI] | b [95% CI] | b [95% CI] | |
Main effect | |||
Racial discrimination | .923 *
[.027, 1.819] | 1.088 *
[.177, 1.999] | 1.115 *
[.218, 2.012] |
Moderator | |||
Emotional support | .229 [−.183, .641] | ||
Two-way interaction | |||
Racial discrimination × Emotional support | −1.446 **
[−2.322, −.569] | ||
Control variables | |||
Gender (male = 1) | .425 [−.321, 1.171] | .433 [−.317, 1.184] | |
Depression | −.276 [−.701, .150] | −.392 [−.818, .034] | |
Perceived stress | .112 [−.321, .545] | .149 [−.279, .577] | |
SES-related risk | .208 [−.021, .437] | .237 *
[.011, .464] | |
Unhealthy behavior | −.483 [−1.099, .132] | −.526 [−1.137, .085] | |
Constant | −.246 **
[−.661, .169] | −1.014 **
[−1.833, −.194] | −1.097 **
[−1.909, −.286] |
Note. N = 331. b = unstandardized beta. CI = confidence interval. SES = socioeconomic status.*p ≤ .05, two-tailed.**p ≤ .01, two-tailed.To address the hypothesized buffering effects of emotional support, Model 3 in Table 4 added the multiplicative interaction term by multiplying the perceived discrimination variable by emotional support as a predictor of AL at age 20. The analysis revealed the hypothesized interaction [b = −1.446, 95% CI (−2.322, −0.569), p < .001], which is illustrated in Figure 2. In Figure 2, high protective emotional support is defined as 1 standard deviation above the sample mean (+1 SD), and low protective support is defined as 1 standard deviation below the sample mean (−1 SD). As hypothesized, the highest levels of AL at age 20 emerged among young adults who perceived high and stable levels of discrimination across adolescence and received low levels of protective emotional support. Conversely, young adults who also perceived high and increasing levels of discrimination across adolescence but received high levels of protective support evinced very low AL levels that were indistinguishable from those of 20-year-olds who perceived relatively low levels of discrimination across adolescence.
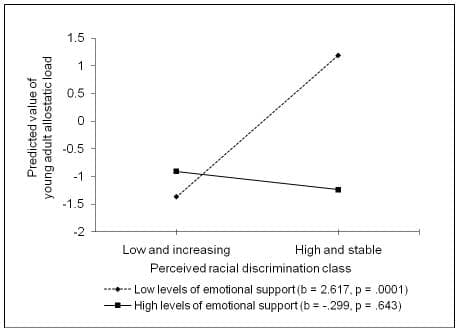
Figure 2
The effect of perceived racial discrimination on young adults’ allostatic load by level of emotional support. The lines represent the regression lines for different levels of emotional support (low: 1 SD below the mean; high: 1 SD above the mean). Numbers in parentheses refer to simple slopes.
Although allostasis theory (McEwen & Stellar, 1993) prescribes a focus on the effects of stress across multiple physiological systems, we repeated the analysis in Model 3, Table 3 for each component of AL to determine, for heuristic purposes, which of the components the perceived discrimination class × emotional support interaction forecast. These analyses are presented in Table 5; all of them include controls for the confounders that were included in the analyses presented in Model 3, Table 3. These confounders were not included in Table 5 due to space considerations. A main effect for perceived discrimination emerged for BMI, with greater perceptions of discrimination forecasting higher BMI. Significant interaction effects emerged for resting diastolic [b = −4.62, 95% CI (−8.34, −0.896), p < .05] and systolic [b = −4.74, 95% CI (−8.57, −0.918), p < .05] blood pressure. A trend for cortisol approached significance [b = −0.864, 95% CI (−1.85, −0.126), p < .10]. For these indicators, high levels of emotional support buffered exposure to high and stable levels of perceived discrimination across adolescence.
Table 5
Regression Models of the Results of Perceived Racial Discrimination and Emotional Support Using Allostatic Load Index at Age 20 Years as the Outcome
Perceived discrimination | Emotional support | Perceived discrimination × Emotional support | |
b [95% CI] | b [95% CI] | b [95% CI] | |
Cortisol | |||
Model 1 | −.242 [−1.209, .724] | ||
Model 2 | −.236 [−1.197, .724] | .437 †
[−.011, .884] | −.850 †
[−1.800, .100] |
Epinephrine | |||
Model 1 | 1.476 [−1.804, 4.755] | ||
Model 2 | 1.550 [−1.722, 4.822] | .236 [−1.288, 1.761] | −2.258 [−5.495, .978] |
Norepinephrine | |||
Model 1 | 2.837 [−5.990, 11.664] | ||
Model 2 | 2.778 [−6.046, 11.602] | 1.655 [−2.457, 5.766] | −1.033 [−9.761, 7.695] |
BP-systolic | |||
Model 1 | 2.336 [−.634, 5.306] | ||
Model 2 | 2.527 †
[−.386, 5.441] | −.093 [−1.458, 1.273] | −4.710 **
[−7.593, −1.827] |
BP-diastolic | |||
Model 1 | .859 [−1.729, 3.446] | ||
Model 2 | 1.041 [−1.486, 3.568] | −.028 [−1.212, 1.156] | −4.591 **
[−7.091, −2.090] |
BMI | |||
Model 1 | 4.367 **
[2.247, 6.487] | ||
Model 2 | 4.365 **
[2.248, 6.482] | .548 [−.444, 1.540] | −.927 [−3.022, 1.169] |
CRP | |||
Model 1 | .097 [−.076, .270] | ||
Model 2 | .099 [−.075, .272] | −.005 [−.086, .076] | −.027 [−.198, .145] |
Note: Gender, depression, perceived stress, socioeconomic status-related risk, and unhealthy behavior are controlled in all analyses. Model 1 includes confounder variables and perceived discrimination as predictors. Model 2 includes confounder variables, perceived discrimination, emotional support, and the interaction of perceived discrimination and emotional support as predictors.N = 331. b = unstandardized beta. CI = confidence interval. BP = blood pressure. BMI = body mass index. CRP = C-reactive protein.†p ≤ .10, two-tailed.**p ≤ .01, two-tailed.
Discussion
During their high school years, African American adolescents experience emotional and social challenges while developing independence, a sense of self, and racial identity. Adolescence is also a time when African American youths become keenly aware of their relative treatment by others and are particularly cognizant of targeted rejection (Stevenson, 2004). Against this developmental backdrop, we examined longitudinally the possibility that perceived discrimination would forecast AL levels during young adulthood, at age 20. The results indicated that (a) perceived racial discrimination was associated positively with AL; (b) the association between perceived discrimination and AL retained its significance when confounder variables were controlled in the data analysis; and (c) the association between perceived discrimination and AL was ameliorated when adolescents received high levels of emotional support. The findings are consistent with suggestions that perceived discrimination can be a chronic social-environmental stressor that, for some, may have a negative impact over time on physiological systems and, ultimately, on health (Mays et al., 2007; Pascoe & Smart Richman, 2009; Williams & Mohammed, 2009). To the best of our knowledge, this is the first study to present data on prospective associations between perceived racial discrimination and AL and on the benefits of emotional support in buffering this process.
These findings are consistent with the premise that poor health and health disparities during adulthood may be associated with experiences earlier in life, particularly for African Americans living in the rural South who grow up with substantial race-related stressors (Pascoe & Smart Richman, 2009). The present findings are also consistent with theoretical propositions that, despite exposure to high levels of perceived discrimination and other race-related stressors, many African American young adults do not develop high AL. Stress buffering processes such as receipt of emotional support may account for those individual differences. Other protective processes that serve as resilience resources may also buffer associations between perceived discrimination and AL; these should be considered in future research. Studies of racial socialization strategies and messages, racial identity, and coping strategies that emphasize cultural pride predict protective effects on psychosocial outcomes when African American youths encounter racial discrimination and other stressors (Gaylord-Harden, Burrow, & Cunningham, 2012). Currently, it is not known whether these protective processes will have similar protective-stabilizing effects on AL and other outcomes implicated in health disparities. The emergence of such effects would demonstrate that the protective effects of racial socialization and racial identity operate to promote both psychosocial and physical health outcomes. To determine whether the findings obtained concerning perceived discrimination × emotional support operated for all, or just some, of the indicators of AL, we executed analyses separately for each of the 7 AL indicators. The hypothesized interaction was significant for the 2 indicators of blood pressure; a trend for cortisol approached significance (p < .10). For each of these interactions, high and stable levels of perceived discrimination across adolescence forecast elevated levels of each indicator for young adults who received low, but not high, levels of emotional support. The importance of these findings becomes evident when they are placed in the context of the health disparities literature. African Americans have the highest prevalence of uncontrolled hypertension among all racial and ethnic groups in the United States (Xu, Kochanek, Murphy, & Tejada-Vera, 2010). The results suggest that exposure to race-related stressors may be associated with the origins of this health disparity, particularly for youths who do not receive the benefits of emotional support.
The research literature has shown perceived racial discrimination to be correlated with the confounder variables; therefore, we controlled them in the data analyses. These variables might be expected to serve as mediators linking perceived discrimination with AL. The data presented in Table 1 reveal that perceived discrimination was associated with the confounder variables of depressive symptoms and perceived stress. Table 1 also shows, however, that AL was not correlated with any of the confounder variables; this precludes any of them from serving as mediators. At present, the mechanisms for a perceived discrimination gradient in AL remain relatively unexplored. Psychological characteristics, coping strategies, and emotion regulation indicators could be posited as mediators. From a myriad of options that merit exploration, we suggest that future research begin with a focus on the regulation of negative emotions. One consistent consequence of perceived discrimination is the development and expression of elevated levels of anger and hostility (Brody et al., 2006), which have been shown to influence physiological functioning across several systems. For example, hostility has been associated with amplified blood pressure reactions to stress (Fredrickson et al., 2000), elevated fasting glucose (Shen, Countryman, Spiro, & Niaura, 2008), and heightened plasma lipid levels (Weidner, Sexton, McLellarn, Connor, & Matarazzo, 1987). Elevated levels of anger forecast CRP levels in adolescents (Brody et al., 2013). Whether anger and hostility mediate the association of perceived discrimination with AL remains an open question, but they remain prime candidates for this role.
In accordance with its definition, AL has been operationalized in past research as the extent of dysregulation aggregated across markers of a variety of allostatic systems (Karlamangla et al., 2006). Health risks associated with AL are hypothesized to result not only from changes in one system but also from modest changes occurring in multiple systems. Researchers have assumed that the components comprising AL all operate similarly as risk factors in response to cumulative or stage-specific stressors. One indicator of AL in this study that is included in most formulations of AL is cortisol level because, if not regulated by countervailing biological processes, it contributes to various physical illnesses (e.g., diabetes, cardiovascular disease, and some cancers; Chung et al., 2009). Conversely, cortisol production in response to challenging circumstances is essential to health through its widespread effects on the body, including not only enhancement of glucogenesis and attention but also inhibition of the immune system and inflammatory processes (Sapolsky, Romero, & Munck, 2000). This raises an interesting question concerning cortisol’s function as a risk or protective factor in formulations of AL. Indeed, in the present study, we found an inverse relation between overnight cortisol levels and CRP, a measure of systemic inflammation. These results imply that higher cortisol levels were serving a protective function with respect to systemic inflammation, suggesting that the designation of cortisol as a risk factor in AL for 20-year-old African Americans is not unambiguous. This finding indicates that, at the very least, more attention should be given to the measurement of AL in persons of different ages.
Several limitations of this study should be addressed in future research. First, the discrimination measure assessed interpersonal discrimination only, rather than structured or institutional discrimination; thus, it provided a limited assessment of the range of discriminatory experiences that adolescents in the rural South encounter. Williams and Williams-Morris (2000) called for more systematic research characterizing the multiple dimensions of racism (e.g., residential segregation). Similarly, Sue et al. (2007) described a taxonomy of racial micro-aggressions that included micro-assaults, micro-insults, and micro-invalidations. Future research should employ more detailed, multidimensional assessments of chronic and daily discrimination in probing the association between racial discrimination and AL.
Second, involvement with community resources beyond the family could also buffer the association between perceived discrimination and AL. Involvement with faith-based institutions not only provides social support but also promotes spiritually centered coping (Constantine, Donnelly, & Myers, 2002). Natural mentors from the community also promote connectedness and provide validation that contribute to a sense of efficacy (Utsey, Bolden, Lanier, & Williams, 2007).
Third, because AL was measured only once, the findings do not provide evidence for a causal pathway from perceived discrimination to AL. To remedy this limitation, future studies should examine the possibility that perception of high and stable levels of discrimination forecast change in AL. This would require longitudinal data with multiple assessments of both perceived discrimination and AL.
Finally, the lack of associations between the confounder measures and AL raise some questions. We assumed that unhealthy behaviors would be correlated with perceived discrimination, as a coping strategy, and with AL. To determine if some relations were masked, correlations were run between each indicator of the unhealthy behavior measure and each indicator of AL. These correlations are available from the first author. One significant correlation emerged, between high self-reported exercise levels and low CRP levels. Although this is an interesting finding that merits further exploration, it suggests that the measurement of unhealthy behaviors needs to be improved in future efforts. The use of technologies such as pedometers for exercise and blood-based assays of nutrients for quality of food intake would provide a more rigorous test of this association.
These cautions notwithstanding, the present study is among the first to show a positive, prospective association between perceived discrimination and AL. It also highlights the benefits of supportive relationships in ameliorating this association and underscores the importance of supportive relationships in keeping stress from “getting under the skin.”