Abstract
The recent worldwide surge of warfare and hostilities exposes increasingly large numbers of individuals to traumatic events, placing them at risk of developing posttraumatic stress disorder (PTSD) and challenging both clinicians and service delivery systems. This overview summarizes and updates the core knowledge of the genetic, molecular, and neural circuit features of the neurobiology of PTSD and advances in evidence-based psychotherapy, pharmacotherapy, neuromodulation, and digital treatments. While the complexity of the neurobiology and the biological and clinical heterogeneity of PTSD have challenged clinicians and researchers, there is an emerging consensus concerning the underlying mechanisms and approaches to diagnosis, treatment, and prevention of PTSD. This update addresses PTSD diagnosis, prevalence, course, risk factors, neurobiological mechanisms, current standard of care, and innovations in next-generation treatment and prevention strategies. It provides a comprehensive summary and concludes with areas of research for integrating advances in the neurobiology of the disorder with novel treatment and prevention targets.
Posttraumatic stress disorder (PTSD) is classified in DSM-5 as a trauma and stressor-related disorder. PTSD symptoms occur following traumatic stressor exposure, reflect an underlying neuropathological process, and are shaped by individual, environmental, and cultural factors. Individuals who suffer from PTSD relive distressing reminders of the traumatic event with vivid perceptual proximity and high emotional intensity. They commonly reorganize their lives while trying to contain and mitigate the persistent effects of past traumatic experience. For those traumatized in a war zone, the “war” continues after their return to a safe environment, a phenomenon referred to as failure to update the context and integrate safety signals. Survivors of sexual assault or torture describe difficulties engaging with and trusting others. Those with PTSD experience the world as dangerous, uncontrollable, and unpredictable and expend great effort to avoid being triggered by reminders. They are hypervigilant, scan the environment for danger, are on high alert even in safe environments, and are tense and exhausted. Core PTSD symptom patterns, including nightmares, flashbacks, and startle reactions, are similar across traumatic events, cultures, and historical descriptions dating back several millennia, suggesting a common underlying neurobiology and psychology.
Understanding the mechanisms leading from trauma exposure to PTSD is critical to predicting and preventing the disorder. Chronologically, these include pretrauma vulnerability factors, peritraumatic responses at the time of exposure, and posttraumatic factors that influence chronicity and recovery. Structurally, they include molecular pathways, neurocircuits, and neurocognitive, emotional, interpersonal, and social factors.
Advancing PTSD Classification and Subtyping
There is growing interest in reducing PTSD heterogeneity by identifying biologically and clinically distinct subtypes of the disorder. A subgroup of those with PTSD, for example, experience peritraumatic and posttraumatic dissociative symptoms, including depersonalization, derealization, amnesia for aspects of the trauma, and altered perception of time (1, 2). From data from the World Mental Health Surveys, the prevalence of this dissociative subtype is estimated to be 14.4%.
Similarly, ICD-11 distinguishes PTSD, characterized by the core symptoms of intrusive and distressing reexperiencing of the traumatic event, avoidance of internal and external reminders of the traumatic event, hypervigilance, and enhanced startle reaction to stimuli, from complex PTSD, a severe subtype that is more common following repeated interpersonal trauma, with prominent disturbances of emotion regulation, self-identity, and relational capacities. Other candidate subtypes include PTSD with neurocognitive impairment and PTSD with depression.
Prevalence and Course of PTSD
Trauma exposure is common. Lifetime estimates of trauma exposure in the United States range from 50% to 89%, of which approximately 50% are from assault and 50% from accidents. In an international study of 69,000 adults, 70% reported lifetime exposure to a traumatic event and 30.5% reported being exposed to four or more traumatic events. A majority of trauma survivors do not develop PTSD, experiencing transient initial symptoms and intensification at times (e.g., at “anniversary” dates), but otherwise are functioning well. Traumatic events are therefore better understood as a necessary but not sufficient cause of PTSD. Traumatic events can also trigger other psychiatric disorders, including major depression and substance misuse. In the National Comorbidity Survey Replication (NCS-R), which surveyed a nationally representative sample of 9,282 Americans age 18 years and older, PTSD was assessed among 5,692 participants, using DSM-IV criteria. The lifetime prevalence of PTSD among adult Americans was estimated to be 6.8%, and current past-year PTSD prevalence was estimated at 3.5%. The lifetime prevalence of PTSD was 3.6% among men and 9.7% among women. The 12-month prevalence was 1.8% among men and 5.2% among women.
Among war zone–exposed military personnel, the National Vietnam Veterans Readjustment Study assessed 3,016 American Vietnam veterans and civilian control subjects between 1986 and 1988, using a representative sample of those who served during the Vietnam era. The estimated lifetime prevalence of PTSD among veterans was 30.9% for men and 26.9% for women. Among Vietnam theater veterans, 15.2% of males and 8.1% of females were diagnosed with PTSD at the time the study was conducted, that is, 15–18 years after the war ended. A 25-year follow-up, the National Vietnam Veterans Longitudinal Study, conducted between 2011 and 2013, 40 years after the war, found prevalences of 4.5% for current PTSD, 10.8% for current PTSD plus subthreshold DSM-5 war-zone PTSD, and 17.0% for lifetime war-zone PTSD.
For most people exposed to trauma, symptoms wane during the year that follows trauma exposure. In a study of rape victims, 95% met PTSD symptom criteria within 2 weeks of the rape, and 1, 3, and 6 months after the rape, the rate declined to 63.3%, 45.9%, and 41.7%, respectively. In the same study, 64.7% of nonsexual assault victims met PTSD symptom criteria 1 week after the trauma. Epidemiological data from the National Comorbidity Survey indicate that the median time for PTSD to remit is 36 months for individuals who sought help for any mental health problem (not necessarily for PTSD) and about 64 months for individuals who never sought help for a mental health problem. Approximately one-third of those who initially qualify for PTSD had not recovered and remained with chronic PTSD. A recent review of studies concerning delayed-onset PTSD confirmed that symptom onset is almost never entirely delayed. For example, in one study of Israeli combat veterans, most cases of apparent delayed-onset PTSD involved either exacerbation of chronic subsyndromic symptoms or delayed help seeking in those with PTSD. PTSD symptom severity may fluctuate over time, often in response to life adversities.
Risk Factors for PTSD
Risk factors in PTSD include female gender, age at trauma, race, lower education, childhood abuse, greater severity of trauma exposure, lack of social support, and additional life stress after trauma exposure. Another analysis identified prior trauma, prior psychological adjustment, family history of psychopathology, greater perceived life threat during the trauma, lower posttrauma social support, greater emotional distress during exposure, and greater dissociation during exposure. A large epidemiological study found that exposure to interpersonal violence and having experienced four or more traumatic events increased PTSD risk. A meta-analysis of risk factors for combat-related PTSD identified lower education, non-officer ranks, army service, combat specialization, higher numbers of deployments, longer cumulative duration of deployments, more adverse life events, prior trauma exposure, and prior psychological problems as PTSD risk factors. Related risk factors included higher levels of combat exposure, discharging a weapon, witnessing someone being wounded or killed, and killing enemy combatants, prisoners of war, and civilians.
Genetic Risk Factors for PTSD
The search for single genetic features has been replaced by a polygenic approach and, more recently, by exploring gene-by-environment interactions, epigenetic features, gene expression, protein synthesis, and brain circuits. A twin study of Vietnam veterans estimated that 30% of the variance in the risk for PTSD is genetic. A number of common genetic variants have been associated with PTSD, including polymorphisms in FKBP5, PACAP1, COMT, DRD2, GABA alpha-2 receptor, G protein signaling 2 (RSG2), a single-nucleotide polymorphism in an intergenic region of the fourth chromosome, and an estrogen response element on ADCYAP R1. In addition, the s/s genotype of the serotonin transporter gene interacts with childhood adversity to increase PTSD risk.
A recent genome-wide association study (GWAS) of over 250,000 participants from the Million Veteran Program identified enrichment in tissue-specific gene expression in several cortical and subcortical regions related to PTSD. A 2020 Psychiatric Genomics Consortium GWAS of 32,000 PTSD cases and 100,000 trauma-exposed control subjects found higher heritability in females compared with males. In a GWAS of PTSD conducted in a multiethnic cohort of over 30,000 individuals with PTSD and 170,000 control subjects, Nievergelt et al. identified three significant loci, two in European and one in African-ancestry analyses, with heritability estimates varying by sex, ranging from 5% to 20%. Five genes were associated with PTSD in those with European ancestry (CDHHC14, PARK2 [a Parkinson’s disease gene], KAZN, TMEM51-AS1, and ZNF813), and five distinct genes were identified in those of African ancestry (LINC02335I, MIR5007, TUC338, LINC02571, and HLA-B). Two additional genes, SH3RF3 and PODXL, were identified from 18,222 protein coding genes among those with European but not African ancestry, and suggest a role for the immune system in PTSD.
Neurobiology of PTSD
PTSD consists of a continuation and expansion of trauma-triggered cognitive, emotional, and physiological responses despite trauma termination. Individuals with PTSD fail to extinguish trauma-acquired conditioned fear responses. Supporting a fear acquisition model, studies indicate an association between elevated heart rate shortly after traumatic events and subsequent PTSD, for example, during emergency department admission after injury. Finally, decreased heart rate variability has been robustly associated with PTSD and linked to emotional cognition and emotion regulation. A comprehensive overview of the neurobiology of PTSD was presented recently in the Journal by Ressler.
Fear Conditioning Circuitry
This model proposes that the acquisition and maintenance of PTSD symptoms is related to the acquisition, overconsolidation, and failure of extinction of conditioned fear responses. The traumatic event is the conditioning stimulus (CS), the immediate responses to trauma are unconditioned responses (UCRs), and stimuli (sights, sounds) present during the traumatic event acquire the ability to elicit conditioned responses (CRs). Psychophysiological studies have supported the fear-conditioning model by consistently showing intense physiological responses to trauma reminders.
Fear conditioning and extinction are adaptive learning processes. The neural circuitry that mediates these processes is essential to survival and is conserved across species. It commands the body’s hardwired, involuntary, instantaneous defensive responses to imminent threat. This highly conserved stress response system includes sympathetic and parasympathetic system activation, cardiovascular and respiratory reactions, activation of the hypothalamic-pituitary-adrenal (HPA) axis, defensive fight, flight, and freezing behaviors, and changes in information processing. It is orchestrated by the central nucleus of the amygdala and is modulated by other amygdala nuclei capable of filtering and evaluating threat stimuli, including the basolateral amygdala (BLA), and further by cortical and subcortical structures, such as the hippocampus, insula, and prefrontal structures. Each of these modulatory layers is highly plastic, subject to new learning throughout life. PTSD is thought to involve new learning in these modulatory systems.
During exposure to extreme threat, previously neutral stimuli overlapping in time with threat stimuli are relayed via the thalamus to the basolateral nucleus of the amygdala, which activates the central nucleus of the amygdala to enable defensive responding. The association between threat or “unconditioned” stimuli (USs) and the previously neutral but currently conditioned stimuli (CSs) is made in the basolateral nucleus of the amygdala. Once formed, this association enables a reexposure to the CSs to trigger a hardwired, unconditioned defensive response (UCR). The magnitude of the defense response is modulated by brainstem serotonergic, noradrenergic, and dopaminergic neurons in the ventral tegmental area, dorsal and median raphe nuclei, and locus coeruleus. These monoamines affect both the magnitude of UCRs and the consolidation of US–CS associations. The balance of neurotransmitters and neuromodulators activated during unconditioned responses also influences the extent to which contextual stimuli, less temporally associated with the USs, may contribute to overgeneralization of threat stimuli.
Activity within the amygdala is under inhibitory control of the prefrontal cortex (PFC). Specifically, glutamatergic neurons from the PFC activate inhibitory interneurons within the BLA, which in turn suppress BLA outputs to the central nucleus. The monoaminergic effects are further modulated by neuroactive steroids and neuropeptides released by the adrenal gland during stress that further magnify, mitigate, or otherwise shape both fear acquisition extinction and recall.
Associations encoded in the amygdala during traumatic events tend to be robust and resistant to change. Their behavioral expression is subject to extinction, occurring when the conditioned stimulus is no longer associated with threat. Neuronal mechanisms underlying extinction include PFC inhibitory input to the BLA. Extinction involves active learning and as such is subject to forgetting and recall. Prolonged stress after the traumatic event can compromise the PFC’s ability to extinguish fear memories, whereas supportive relationships in a safe environment may enhance it. High levels of continuing stress and absence of soothing contacts decrease the likelihood of efficient extinction and contribute to its consolidation and increase the risk of developing chronic PTSD. To remain efficient, extinction learning must be retained, and studies have shown that PTSD is associated with deficient extinction learning. Finally, upon recall, traumatic memories become transiently plastic and must be reconsolidated in order to persist. Such a “reconsolidation window” offers a transient opportunity for therapeutic intervention.
Threat Detection and Emotion Regulation Circuits
Other circuits implicated in PTSD development mediate threat information processing, mediated by the amygdala, the dorsal anterior cingulate and insular cortices, and regulatory control mechanisms that involve the hippocampus and medial and lateral PFC regions. These regions undergo plastic modifications during exposure to potentially traumatic events. The amygdala assigns rapid “threat potential” tagging of environmental cues. The amygdala-associated PFC regions and insula have been implicated in detecting stimulus saliency and biasing attention to threat. Emotion regulation circuits include the medial PFC and dorsolateral PFC. Evidence from neuronal network studies demonstrates segregation among the salience network, involving regions of the insula, anterior cingulate cortex (ACC), and amygdala; the attention network, involving the dorsolateral and ventrolateral PFC; and the default mode network (DMN), including the medial PFC and hippocampus. Neuroimaging studies in PTSD patients have found abnormalities in threat detection and emotion regulation regions, with increased reactivity of the extended amygdala, insula, and dorsal ACC regions and decreased regulatory activity in subregions of the prefrontal lobe.
Executive Control, Memory, and Attention
Salient PTSD symptoms include inability to concentrate, memory disturbances, and difficulties planning and monitoring one’s activity. Activity in dorsal ACC and frontoparietal attentional networks has been implicated in cognitive control, including performance monitoring, response inhibition, task shifting, working memory, attention, and memory. This dysregulation disengages medial prefrontal–medial parietal DMN regions involved in internally oriented, self-directed mentation. DMN regions are overactive or underdynamic in PTSD, resulting in poorer ability to disengage from threat responses and discriminate truly threatening stimuli reminders of traumatic experiences.
Context Appraisal and Update
Among the key clinical features of PTSD is persistence of fear-driven avoidant behavior, heightened reactivity to reminders, and hypervigilance despite—and often years after—reaching safety. Integrating safety signals is fundamental to realistically appraising and responding to signals (e.g., noise, sirens) within one’s current environment. The persistent and inappropriate hypervigilance and responsivity in PTSD reflect an impaired capacity to update contextual appraisal from threat to safety. Difficulty differentiating safety from threat results in part from improper contextual update processing. Contextual processing is mediated by the ventromedial PFC, the hippocampus, and the thalamus and requires low adrenergic drive during sleep. Decreased activity of the ventromedial PFC in patients with PTSD has been linked to abnormal processing of contextual information, as well as to impaired extinction recall.
Abnormalities in these brain circuits in fear learning, threat detection, executive control, and contextual learning are illustrated in Figure 1.
FIGURE 1. Brain regions implicated in the pathophysiology of PTSDa
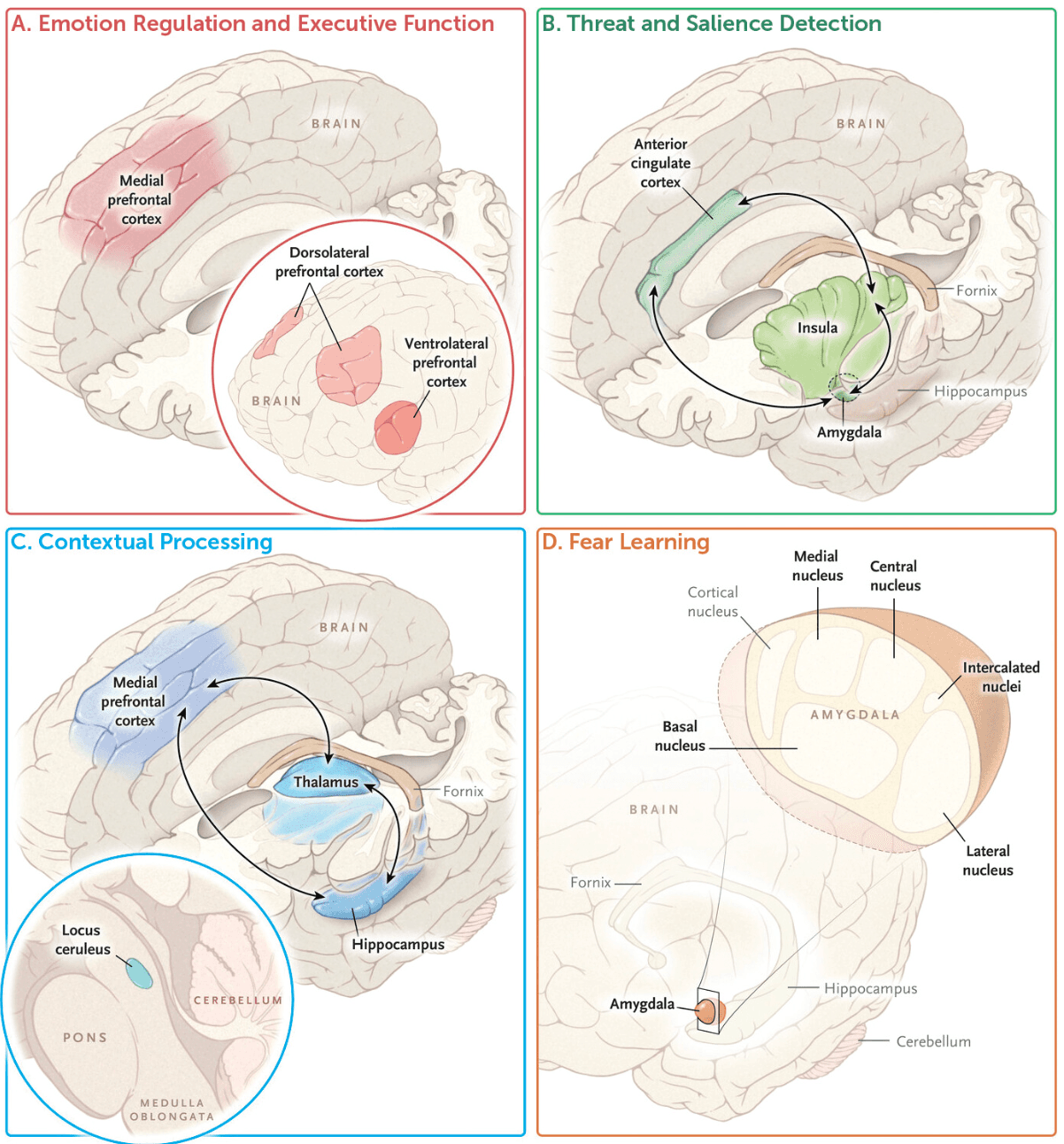
aShown are the known connectivity paths within four dysfunctional circuits that play a part in the psychopathology of PTSD: emotion regulation and executive function, threat detection, contextual processing, and fear learning. (From New England Journal of Medicine, A. Shalev, I. Liberzon, C. Marmar, Post-traumatic stress disorder, vol. 376, pp. 2459–2469, Copyright © 2017 Massachusetts Medical Society. Reprinted with permission.)
Endocrine and Molecular Pathways in PTSD
Glucocorticoids.
The HPA axis and sympathetic nervous system are important stress-reactive systems. They contribute to brain information processing, reactivity, and behavior in response to threat. In PTSD, stress pathways involving cortisol signaling via the HPA axis are altered, with blunted cortisol responses to stressors as a result of enhanced negative feedback from increased glucocorticoid receptor sensitivity in PTSD. Diminished cortisol response to threat is associated with increased and persistent adrenergic responses facilitating fear conditioning, and alarm activation during trauma recall.
Catecholamines.
Exaggerated noradrenergic signaling is related to deficits in frontal lobe executive function, resulting in undermodulated amygdala reactivity as well as sleep fragmentation and nightmares, which are common in PTSD. An exaggerated adrenergic response during trauma exposure and in the hours following exposure may contribute to the formation of more durable emotional memories. Noradrenergic hyperreactivity may be a pretrauma vulnerability trait in some individuals, or, in others, it may develop as a result of trauma exposure. Factors that may contribute to the increased release of norepinephrine in response to traumatic stress or conditioned reminders of the trauma include decreased expression, affinity, or function of inhibitory alpha-2 adrenergic autoreceptors and genetic or stress-induced decreases in neuropeptide Y (NPY). Factors that may enhance amygdala reactivity may include a downregulation of intra-amygdala synaptic GABA receptors or reductions in GABAergic neuroactive steroids, such as allopregnanolone. The alpha-2 antagonist yohimbine induces extreme hyperarousal, flashbacks, vivid intrusive memories, panic, and increases in heart rate and systolic blood pressure in male combat veterans with PTSD. Alpha-1 adrenergic postsynaptic receptor antagonists, such as prazosin, have been used for the treatment of nightmares in PTSD and evaluated for early prevention of PTSD (see the “Treatment” section).
Neurosteroid and neuropeptide interaction with other neurohormonal mediators.
It is also important to evaluate the role of cortisol in the pathophysiology of PTSD in the context of other relevant neurohormonal responses. NPY has anxiolytic and stress resilience effects in numerous animal models and human studies. It stimulates neurogenesis in the hippocampus, supporting recovery from stress. Higher levels of plasma NPY during military special forces simulated captivity training were associated with stress resilience. NPY also has several trophic effects, including improved sleep quality, lower heart rate response to adrenergic stimulation, and better energy balance, affecting recovery from early PTSD symptoms. Allopregnanolone and pregnanolone selectively enhance the effect of the brain principal inhibitory neurotransmitter GABA. They also have neuroprotective effects by increasing myelination, decreasing apoptosis, and increasing neurogenesis. Studies have shown that lower levels of these hormones are associated with higher levels of PTSD symptoms. Dehydroepiandrosterone (DHEA) is the immediate precursor of the androgens testosterone, dihydrotestosterone, and androstenedione and is secreted from the adrenal gland along with cortisol in response to ACTH. DHEA antagonizes GABAA receptors and facilitates N-methyl-d-aspartate (NMDA) receptor function. In humans, higher DHEA levels under stress appear to confer neurocognitive and psychological resilience and may protect against negative health outcomes.
Dopamine and serotonin.
The release of dopamine in the amygdala promotes the expression of unconditioned and conditioned stress responding. Additionally, dopamine may inhibit PFC projections into the BLA and thus diminish the inhibitory control over learned fear responses, contributing to hypervigilance and sensitivity to environmental cues. Dopamine is also highly relevant to reward signaling in the nucleus accumbens, a process that appears to be downregulated in PTSD, including in PTSD with prominent depression symptoms. Psychopharmacological treatment and genetic epidemiological studies suggest that the serotonin (5-HT) system impacts both PTSD risk and symptom severity. Administration of meta-chlorophenylpiperazine (mCPP), which interacts with multiple 5-HT receptor subtypes and with the 5-HT transporter to release 5-HT, provokes anxiety, panic attacks, and PTSD symptoms, including flashbacks, and cognitive changes that are reversible by mixed 5-HT1c/5-HT2 antagonists. Selective serotonin reuptake inhibitors (SSRIs), however, do not reduce the likelihood of developing PTSD when administered shortly after trauma exposure.
Epigenetic Changes Associated With PTSD
The epigenetic regulation of gene transcription may provide new opportunities for understanding PTSD. Epigenetic effects consist of coordinated modification of gene promoters and chromatin such that access to the gene by regulatory elements is either enhanced or limited, including lower methylation of the glucocorticoid receptor gene promoter 1F in peripheral blood cells in veterans. Of note, research has shown differences between groups of persons with and without PTSD in methylation patterns of DNA in white blood cells. A cluster of unmethylated immune system function genes also characterized PTSD, which otherwise showed a greater number of methylated genes. In addition, there were group differences in methylation of the dinucleotide methyl transferase type 3 beta and 3L genes, which are involved in de novo rather than maintenance methylation, suggesting that specific adaptive epigenetic capacities themselves may be altered in PTSD.
The extent to which epigenetic mechanisms, operating after trauma exposure, underlie some of the persistent effects of exposure is an exciting new perspective. Research has shown that immobilization stress in rodents reduced expression of brain-derived neurotrophic factor (BDNF) gene transcripts I and IV in the hippocampus in association with decreases in the level of histone acetylation of the P1 and P4 promoters. Conversely, research has shown that extinction of conditioned fear was accompanied by an increase in the levels of histone acetylation of the gene promoters for BDNF transcripts I and IV. Together this work suggests that activation of specific PFC circuits in combination with agents that facilitate epigenetic processes that enhance synaptic plasticity and stabilization of new neuronal circuits may contribute to the persistence of PTSD and recovery from PTSD. Recent studies have shown that some epigenetic features of PTSD are modified after successful treatment or spontaneous recovery. Successful treatment of PTSD has been shown to be accompanied by significant changes in DNA methylation at 12 differentially methylated regions.
Structural Neuroanatomy
Structural brain imaging.
The first reported structural abnormality in PTSD was reduced left hippocampal volume in Vietnam veterans with PTSD. This finding had been interpreted as reflecting the hippocampus’s vulnerability to excessive stress hormone levels due to prolonged stress. Numerous studies subsequently reported left, right, or bilateral hippocampal volume reduction in PTSD. Other studies, particularly in younger veterans, have failed to replicate this finding, but meta-analyses generally support the existence of reduced hippocampal volume in PTSD. Findings of smaller hippocampal volume in PTSD lack disorder specificity, however, as similar findings have been observed in schizophrenia and affective disorders. A longitudinal study of hippocampal volume in early PTSD has not shown a hippocampus shrinking effect, and an elegant twin study of Vietnam veterans found smaller hippocampi in unexposed identical twins of war veterans with chronic PTSD, thereby positioning smaller hippocampi as a vulnerability factor, rather than a consequence of PTSD.
More recent studies have reported white matter volume reductions in the corpus callosum and gray matter reductions in the amygdala and the insula. The evidence concerning structural alterations of the amygdala is quite weak. Two meta-analyses reached somewhat different conclusions. Several studies have pointed to abnormal structural characteristics in the ACC, including reduced ACC gray matter volumes or white matter abnormalities of the cingulum. These reduced volumes may be particularly characteristic of the rostral and subcallosal portions of the ACC, rather than the dorsal ACC. Rostral ACC volume has been found to predict response to cognitive-behavioral interventions, such that larger volumes were associated with greater symptom reduction. A study of pregenual ACC volumes in monozygotic twins discordant for PTSD suggested that reduced volumes might reflect an acquired trait of PTSD rather than a vulnerability factor.
Functional brain imaging.
Studies of PTSD have revealed various patterns of brain activity and connectivity alterations, including amygdala hyperactivity associated with increased emotional reactivity and vigilance to threat cues; hippocampal dysfunction associated with intrusive memories, flashbacks, and impaired context appraisal; prefrontal cortex dysregulation involved in emotion regulation, cognitive control, and fear extinction; DMN alteration that may contribute to rumination and alterations in self-awareness; and insula dysfunction and fear circuitry dysregulation, as discussed above.
Sleep
Up to 90% of people with PTSD report sleep disturbances such as nightmares and insomnia. In studies examining the physiological basis for sleep disturbances in PTSD, both macro-level sleep architecture (i.e., time spent in various sleep stages overnight) and micro-level physiological measures of autonomic system activity during sleep (i.e., heart rate variability, electrodermal activity) have been implicated. The frequent nightmares that are often the hallmark of PTSD are thought to occur in REM sleep. Additionally, REM sleep has been shown to play a role in the maintenance of fear memories. Sleep abnormalities also characterize the early phases of PTSD: While it is unclear why some survivors develop PTSD and others do not, persistent sleep abnormalities, which are present in upwards of 66% of those who develop the disorder, have been suggested as a contributing factor. More specifically, recent studies have shown that sleep disturbances, measured prior to exposure to traumatic stress, predict the development of PTSD.
Neurobiology of Persistence of PTSD
An intriguing feature of PTSD is its persistence, that is, the failure of extinction despite the absence of further stressor exposure. Longitudinal studies have confirmed a frequent pattern of immediate expression of PTSD symptoms followed by recovery in most of those exposed, and persistence of symptoms in those who develop chronic PTSD. The conditioned fear analogy similarly predicts extinction in the absence of return to a nontraumatic environment, which does not occur in chronic PTSD. A neurobiological account of PTSD therefore must also consider the disorder’s maintaining factors. Several theoretical models account for the persistence of PTSD, including a kindling hypothesis, according to which patterns of pathological neuronal coactivation become “entrenched” by repeated use; an allostatic stress hypothesis presuming a “wear and tear” of CNS emotion control systems (e.g., the hippocampus) by chronic stress; and what might be referred to as a subsystem clash or truncated response view, according to which one brain subsystem blocks another from achieving the full processing of its inherent tasks.
Treatment
Psychological Treatment of PTSD in Adults
A review of 70 studies of psychotherapies involving a total of 4,761 participants showed that many of the studies were rated as being at risk of bias, and sample sizes were generally small and had limited follow-up data. There was evidence for individual trauma-focused cognitive-behavioral therapy (TF-CBT) that includes prolonged exposure, which focuses on reexperiencing the traumatic event through repeatedly engaging with the memories (imaginal exposure) and everyday reminders (in vivo exposure) rather than avoiding triggers, and for eye movement desensitization and reprocessing therapy (EMDR), which includes repeatedly recalling distressing images while receiving sensory inputs. Non-trauma-focused psychotherapies include present-centered therapy (PCT), which focuses on current relationship and work challenges rather than the trauma, are equally effective immediately posttreatment, and there is some evidence that TF-CBT and EMDR are superior to PCT between 1 and 4 months following treatment. Individual TF-CBT, EMDR, and PCT were found to be more effective than other therapies. There is also evidence that cognitive processing therapy, which emphasizes correcting faulty attributions, including posttraumatic overgeneralizations of the world as dangerous, uncontrollable, and unpredictable, is effective for adults with chronic PTSD. A recent study in adults with PTSD reported that interpersonal therapy (IPT), focusing on role expectations in dyadic relationships, was comparable to prolonged exposure for treatment completers, with fewer dropouts among participants with comorbid depression in the IPT group. This study and others raise the provocative question, “Is exposure necessary” for successfully treating PTSD?.
Psychotherapy for Military-Related PTSD
A review of 36 controlled trials found that military-related PTSD is complex and difficult to treat. Trauma-focused treatments and cognitive processing therapy are associated with improvement in symptoms in approximately 60% of veterans but are limited by relatively high dropout rates, and treated patients often remain symptomatic, with more than two-thirds retaining their diagnosis. Non-trauma-focused treatments, which are less demanding for patients and professionals, provide a reasonable option when their use leads to continued willingness to remain in care.
Psychological Therapies for the Treatment of PTSD in Children and Adolescents
A review of 14 controlled studies, including 758 participants exposed to sexual abuse, civil violence, natural disaster, domestic violence, and motor vehicle accidents, found that none of the studies were rated at high risk for selection or detection biases, but a minority were rated at a high risk for attrition, reporting, and other biases. Across all psychological therapies, improvement was significantly better within a month of completing psychological therapy compared with a control condition. The psychological therapy for which there was the best evidence of effectiveness was CBT, with greater improvement lasting up to a year.
Pharmacotherapy for Adults With Chronic PTSD
Meta-analyses comparing the efficacy of different medications for treating PTSD have found that the largest body of evidence for short- and long-term efficacy of medication currently exists for SSRIs, and the strongest evidence is for sertraline and paroxetine, which are approved by the U.S. Food and Drug Administration (FDA) for adults with PTSD. There are promising findings for the serotonin-norepinephrine reuptake inhibitor (SNRI) venlafaxine and the atypical antipsychotic risperidone. Evidence for the effectiveness of benzodiazepines is lacking, despite their continued use in clinical practice. Finally, the alpha-1 adrenergic antagonist prazosin and the atypical antipsychotics show some efficacy in treatment-resistant PTSD, and prazosin shows preliminary efficacy for treating nightmares. Prazosin is more effective in patients with elevated pretreatment standing blood pressure. Insomnia is prevalent and disabling in chronic PTSD, and treatment with low-dose trazodone is preferable to benzodiazepines. The recently developed orexin antagonist suvorexant is promising for managing trauma-related insomnia. Medications in the pipeline are targeting endocannabinoids, including fatty acid amide hydrolase inhibitors, nabilone, and cannabidiol, and other novel targets, including glutamate, BDNF, and the oxytocin receptors.
Several tricyclic antidepressants (TCAs) have been studied in the context of PTSD treatment, including imipramine, amitriptyline, and nortriptyline. While TCAs may offer benefits in managing PTSD symptoms in some patients, they are generally reserved for individuals who have not responded to first-line treatments or who cannot tolerate SSRIs or SNRIs due to side effects or contraindication. Close monitoring is necessary to manage side effects and ensure safety. The evidence supporting the use of monoamine oxidase inhibitors (MAOIs) for PTSD is limited compared to other pharmacological and psychotherapeutic interventions. Additionally, MAOIs have several potential side effects and require dietary restrictions to prevent interactions with certain foods and medications that can lead to a hypertensive crisis. Due to these considerations, MAOIs are usually reserved for individuals who have not responded to other treatments or who cannot tolerate other classes of antidepressants.
Pharmacological Treatment of Comorbid PTSD and Substance Use Disorder
A randomized clinical trial of sertraline did not show overall efficacy for comorbid PTSD and alcohol use disorder (AUD), although it may be useful among light drinkers. Another clinical trial demonstrated the efficacy of both disulfiram and naltrexone for the treatment of AUD in individuals with PTSD. A recent clinical trial suggested that norepinephrine reuptake inhibitors may be useful for comorbid PTSD and AUD. Noradrenergic medications that are promising for comorbid PTSD and substance use disorder include prazosin, guanfacine, and atomoxetine. Promising glutamate/GABA medications include topiramate, memantine, acamprosate, N-acetylcysteine, and ketamine. The safety and efficacy of these medications for the treatment of PTSD and substance use disorder needs to be assessed in controlled clinical trials.
Combined Pharmacotherapy and Psychological Treatments for PTSD
A meta-analysis has assessed whether the combination of psychological therapy and pharmacotherapy is more effective for treating PTSD than either type of intervention alone. Patients of any age or gender, with chronic or recent-onset PTSD arising from any type of event relevant to the diagnostic criteria, were included. Four trials were eligible for inclusion, and one of these trials (N=24) was for children and adolescents. All used an SSRI and prolonged exposure or another cognitive-behavioral intervention. There was no strong evidence for superiority of combined treatment over either psychological therapy or pharmacotherapy used as monotherapy.
MDMA
A recent study evaluated the effect of 3,4-methylenedioxymethamphetamine (MDMA) as add-on therapy provided in conjunction with CBT and found that the combination more efficiently reduced PTSD symptoms than CBT alone. MDMA is widely used as a recreational drug for its effects of mood elevation, altered sensation, and increased empathy and energy. Chemically, MDMA is a substituted amphetamine that primarily increases serotonin, dopamine, and noradrenaline signaling. MDMA was recently reviewed by the FDA, which recommended against approval, expressing concerns about the design of the registration trials, including unblinding and participant and clinician bias, as well as cardiovascular risk and abuse potential.
Alternative and Complementary Treatments
There is preliminary evidence to support the efficacy of acupuncture, breathing and muscle relaxation, mindfulness meditation, and yoga. For body-based therapies, there is limited evidence, including no published studies for movement-based and energy therapies.
Novel and Emerging Treatments
Reconsolidation therapy (RT).
RT is a brief approach that targets memory reconsolidation. The patient develops a detailed written narrative of their trauma, receives a dose of propranolol (1 mg/kg) 90 minutes before treatment, and reads their narrative aloud during the session. It is proposed that the propranolol decouples intense emotions from the recollection of the trauma and a new memory is formed, which is reconsolidated with a factual narrative but without terror, horror, and helplessness and other negative trauma-related emotions, and which replaces the original terror-fueled narrative. This process is repeated over four to six weekly sessions. In a 6-week, double-blind placebo-controlled trial, total PTSD symptom scores declined 11.50 more points in the group that received propranolol compared with the group that received placebo, and the effect size for the treated group was 2.74, compared to 0.55 for the control group. Additional studies provide supportive evidence for propranolol-assisted RT. The positive findings for these RT studies that combine a variation of written narrative exposure with propranolol contrast with a recent meta-analysis that did not find consistent evidence for the efficacy of propranolol as a monotherapy for traumatic memory disruption in PTSD.
Cannabis and cannabidiol (CBD).
In a recent systematic review, cannabis was associated with a reduction in overall PTSD symptoms and improved quality of life. Dry mouth, headaches, and psychoactive effects such as agitation and euphoria were the commonly reported adverse effects. Cannabis was generally well tolerated, but small proportions of patients experienced a worsening of PTSD symptoms. Overall, the evidence to date for cannabis stems from low-quality and high-risk-of-bias studies, and cannabis is not recommended in PTSD patients at risk for substance abuse. Studies of CBD for PTSD, for PTSD comorbid with traumatic brain injury, and for PTSD comorbid with AUD are currently in progress.
Ketamine.
A randomized double-blind crossover study found that a single infusion of 0.5 mg/kg of ketamine, an NMDA and AMPA glutamatergic receptor modulator, led to rapid symptom reduction compared with midazolam. Ketamine was also associated with reductions in depression symptoms. Further clinical trials are required to determine efficacy, safety, and duration of treatment responses.
Psilocybin.
In a rodent model of PTSD, psilocybin increased fear extinction, increased dendritic complexity and spine density in the hippocampus, and reversed stress-induced decreases in proteins associated with neuroplasticity, including BDNF and mTOR. Human neuroimaging studies suggest a reduction in amygdala activity. Clinical trials are required to determine safety and efficacy.
Repetitive transcranial magnetic stimulation (rTMS).
A meta-analysis of 13 studies (549 participants) of rTMS found that this treatment was superior to sham comparisons in reducing PTSD and depression severity. The quality of evidence, however, was limited by small sample sizes, treatment heterogeneity, inconsistent results, and an imprecise pooled effect. Further research is required to advance the evidence on this treatment.
Neurofeedback.
A novel neurofeedback treatment trains individuals with PTSD to directly reduce amygdala activity. Studies are under development, with promising preliminary results. A prospective, multicenter, multinational open trial of amygdala-derived EEG neurofeedback treatment of 79 civilians and veterans reported clinically significant PTSD symptom improvement in 66.7% of the participants. Sham-controlled studies are under way.
Vagal nerve stimulation (VNS) and stellate ganglion block (SGB).
VNS is proposed to reduce amygdala activity in PTSD by modulating the parasympathetic system. Pilot studies have reported benefits, but there are side effects, including coughing, hoarseness, headache, dyspnea, and paresthesia at the implant site. There is insufficient high-quality evidence to support a recommendation at this time. SGB is accomplished by an injection around the stellate ganglion, a sympathetic nerve bundle in the neck. Blocking this ganglion reduces sympathetic activity, potentially modulating the HPA axis and disrupting fear memory consolidation. A multisite study of PTSD randomized 74 participants to SGB and 39 to a sham control treatment. After two treatments (at weeks 0 and 2), PTSD symptoms were reduced at week 8, with a 12.6-point decrease in total score on the Clinician-Administered PTSD Scale for DSM-5 in the SGB group, compared to a 6.1-point decrease in the control group. Side effects include hoarseness, lightheadedness, hypertension, dysphagia, cough, dyspnea, headaches, and visual hallucinations. Rarely, seizures have been reported. Further research is required to determine the risks and benefits of SGB for PTSD.
Early and Preventive Intervention
Early Psychological Interventions for Preventing PTSD
Debriefing.
Psychological debriefing, a widely used method in the 1980s and 1990s, aimed to prevent long-term posttraumatic symptoms by promoting emotional processing of traumatic events. Debriefing was offered unselectively to anyone exposed to a potentially traumatic event. The method typically involved a single session, in either group or individual format, within several days after the trauma exposure, and included general education about the possible effects of trauma exposure, as well as chronological retellings of the recent traumatic event. The method has face validity and is still well known, and therefore it may be expected by laypeople when confronted with traumatic events. However, well-conducted studies showed no evidence of beneficial effects and even suggested that debriefing may have a negative effect on recovery. After a negative Cochrane review first published in 1997, most treatment guidelines have been updated to recommend against providing psychological debriefing on a routine basis for adults after trauma.
CBT for Preventing PTSD
Exposure-based CBT efficiently reduces PTSD symptoms in selected samples. A study using modified prolonged exposure in rape, assault, and motor vehicle accident survivors around 12 hours after trauma found lower PTSD symptoms in the intervention group at 4 and 12 weeks after trauma, mainly for sexual assault victims. Another study found 5 weeks of exposure-based CBT to be effective in reducing PTSD symptoms in participants who met diagnostic criteria for acute stress disorder. Research has also found a reduction of PTSD symptoms at 13 months—but not 3 months—after the traumatic events.
In a study comparing exposure therapy, stress inoculation training, and their combination, researchers showed that early intervention with both exposure-based and non–exposure-based CBT similarly and efficiently reduced the prevalence and the intensity of PTSD symptoms 5 months and 9 months after trauma exposure. The 9-month outcome of delayed CBT (starting 5 months after the event) did not differ from that of the 1-month onset groups. A small study with 3 weeks of prolonged exposure did not find significant symptom improvement with prolonged exposure compared with supportive counseling. Cognitive-based CBT has also shown effectiveness in some but not all studies. Researchers compared CBT to a waiting-list control condition among individuals with acute PTSD and found that CBT accelerated recovery but made no long-term difference.
Modifications of CBT-based interventions have shown varied results. A telephone-based CBT study in patients with PTSD due to experiencing and anticipating cardioverter defibrillator impulses and potential life threat from cardiac arrest reported significant improvements in PTSD symptoms in the CBT group. Researchers developed a self-guided Internet-based intervention (Trauma TIPS) based on CBT to prevent the onset of PTSD symptoms but found in a randomized controlled trial that the results did not support the efficacy of the intervention. EMDR has been recommended as an early intervention by recent treatment guidelines. Remarkably, current EMDR protocols include significant components of trauma-focused and trauma-recollection steps. As with other brief interventions, EMDR may require booster or repeat sessions to sustain its effect.
CBT is currently the mainstay of early prevention of PTSD. Several considerations make the systematic implementation of CBT for all survivors a major challenge, however. First, a meta-analysis of early interventions found that CBT is specifically efficient in participants with diagnosable PTSD at treatment onset, whereas survivors with subthreshold PTSD symptoms recover as well with or without CBT. Second, research in emergency-department-based CBT has shown that the known efficiency of CBT is limited to survivors of sexual assault, showing no effect among accident victims. Moreover, attempts to deliver diluted versions of CBT (such as telephone or web-based communication) have yielded negative results. Interestingly, studies do not show a reduced effect of CBT when administered later in the development of PTSD (e.g., 6 months after trauma exposure instead of 1 month). CBT, therefore, is best positioned by current research as the treatment for ascertained clinical cases and is optimally provided at some temporal distance from the traumatic event. On the positive side, the early outcome of CBT is maintained over time, and thus this intervention is virtually the unique means to stop the progression of early PTSD into chronicity. In its best performance, however, early CBT leaves a substantial number of survivors unaffected and thus should be supplemented by “second-step” interventions or by interventions specifically affecting participants in the nonremission trajectory.
Pharmacological Interventions for Preventing PTSD
Various pharmacological agents have been examined for the prevention of posttraumatic symptoms. A recent review article concluded that, in general, there is moderate-quality evidence for the efficacy of hydrocortisone and no evidence for propranolol, escitalopram, temazepam, and gabapentin. This field is rapidly developing as the underlying neurobiological processes start to be clarified by more studies.
Hydrocortisone.
Hydrocortisone has been shown to be effective especially in patients who have never been treated for psychiatric disorders. The underlying mechanism is not entirely understood. One hypothesis is that hydrocortisone can facilitate extinction learning through both nongenomic and genomic effects. Some also believe that high-dose exogenous hydrocortisone administered shortly after trauma may promote recovery through enhancing synaptic plasticity and connectivity. An animal model showed significantly increased dendritic growth and spine density, with increased levels of BDNF and obtunded postsynaptic density protein-95 (PSD-95) levels in steroid-treated stressed rats. Increasing cortisol levels also counter adrenergic activation, thereby reducing fear conditioning.
Propranolol.
Propranolol is a beta-adrenergic antagonist that crosses the blood-brain barrier and is therefore capable of reducing the CNS adrenergic drive associated with defensive threat responses. Experimental studies of propranolol in healthy subjects have shown that its administration prior to exposure to potentially traumatic narratives reduced the recollection of stressful elements of the narrative without affecting the general recall. It was thereby positioned as a prime candidate to affect traumatic recall in PTSD. Early treatment with propranolol aims to mitigate overconsolidation of traumatic memories by blocking the memory-enhancing influence of stress hormones. Theoretically, therefore, it should be initiated while memories of the trauma are encoded and consolidated, preferably within hours of the traumatic event. However, controlled studies in the first hours after exposure have failed to show a preventive effect of propranolol on PTSD symptoms, although they showed a reduction in physiological responses to reminders. The documented gap between propranolol’s effect in physiological responses to trauma reminders and its lack of effect in PTSD symptoms could be interpreted as suggesting that the pathogenesis of PTSD is not limited to amygdala-mediated threat conditioning and involves other brain areas and memory systems.
Benzodiazepines.
Benzodiazepines are a group of GABA agonists, and thus they enhance the inhibitory transmission in wide areas of the brain. They are used as anxiolytics and sleep inducers but also interfere with long-term potentiation, learning, and memory. As such, they were positioned as capable of reducing excessive “learning” occurring during or following trauma exposure. However, three human studies have shown that participants receiving benzodiazepines fared worse than those who were not treated at all. An animal “predator stress” study found that administering diazepam shortly after predator odor exposure enhanced the acquisition of long-term fear responses. While the exact mechanism by which benzodiazepines increase the risk of PTSD following traumatic exposure is unknown, it is possible that these compounds interfere with post-event learning of extinction. Intriguingly, the current data on the use of benzodiazepines for PTSD are based on small studies, while these compounds are widely used to mitigate distress following various stressors. Nonetheless, benzodiazepines are not recommended for use in the aftermath of traumatic events.
Morphine.
Animal studies suggest that morphine can produce retrograde amnesia for contextual conditioned fear, possibly through decreasing cAMP or activating NMDA receptors in the hippocampus. Observational studies of hospital patients suggest a possible beneficial effect of morphine administration within 48 hours after trauma exposure to survivors who have pain, and similar results were reported, retrospectively, in 696 military personnel with severe combat injury. Given the retrospective nature of most studies, more research is needed to separate a specific effect of morphine from a generic “analgesic” effect. Pain after trauma exposure is a potent predictor of PTSD. It is unclear, therefore, whether morphine has any preventive value in trauma survivors without physical pain.
Other and Investigational Approaches
Oxytocin is involved in emotion stress regulation, social engagement, and attachment, and preliminary studies suggest that it may buffer the development of PTSD when administered shortly after trauma exposure. NPY is another neuroendocrine candidate for early intervention. A rodent study showed a significant impact of NPY in mitigating PTSD-like symptoms, which could be through NPY’s ability to modulate the dysregulation of the HPA axis and central noradrenergic activity. Small-molecule agonists for the NPY1 and NPY5 receptors are in development.
Besides hormonal intervention, neurobehavioral retraining is also being tested for its capacity to reduce negative emotional processing and enhance executive control. Emerging evidence of impaired emotion regulation and executive functions in PTSD is likely to generate other early neurocognitive approaches.
Limitations and Challenges to PTSD Prevention
Studies on PTSD prevention have demonstrated large variations in study design and methodology. Differences in methodology need to be carefully examined before one can infer from study results and determine the most effective intervention for a certain population or individual. The research evidence also reflects wide heterogeneity in sampling, trauma types (e.g., military vs. nonmilitary, accidents vs. interpersonal trauma), injury severity, comorbid depression, and peritraumatic reactions. Thus, the ultimate choice and integration remains in clinicians’ hands and calls for conceptual as well as clinical expertise.
Among all traditional prevention methods, TF-CBT has been mostly reported as an effective approach. Taking into consideration the heterogeneity of trauma survivors, people with different age, gender, trauma type, and potentially different genetic features, childhood experience, and recovery environment may require different strategies. For example, TF-CBT has been reported to be more effective for victims of traffic accidents, and exposure therapy to be more beneficial for victims of sexual assault and people with high genetic risk for PTSD.
Future Directions
Advancing the Understanding of PTSD Heterogeneity
By definition, PTSD is associated with clinically significant emotional distress and functional impairment. However, as is true for most medical disorders, including back injuries and heart disease, there is not a one-to-one correspondence between symptom severity and relationship and occupational impairment. There are higher-functioning trauma survivors with more severe symptoms and lower-functioning survivors with less severe symptoms. Longitudinal studies show both unremitting symptoms and time-dependent fluctuations in PTSD expression and severity. The latter are often due to trauma reminders and personal and interpersonal pressures. Specifically, PTSD distress and dysfunction can be intensified by loneliness, despondency, meaninglessness, lack of anchor in life, concurrent stressors, trauma reminders, and substance misuse. To advance precision medicine, clinicians need to develop care plans that account for these individual differences in symptom and functioning trajectories.
Mapping Pathways of Pathogenesis to Advance PTSD Subtyping and Personalize Treatment
PTSD is likely multicausal, and hence individuals with differing vulnerabilities and different exposure and postexposure circumstances may express the PTSD symptom complex through individual-specific pathways, and in turn be responsive to individual-specific interventions. One way to advance the prevention and treatment of PTSD is to better map the variety of paths leading to this condition and map those paths onto subsets of trauma-exposed individuals. Once such knowledge becomes available, target-specific early intervention might replace generic treatment protocols applied in a one-size-fits-all approach. By enhancing prediction models, intervention studies can take the important step of selecting the most relevant sample for a more rigorous study design and the most clinical interest. At the same time, research must continue exploring and confirming the underlying mechanisms of posttraumatic pathogenesis. Increasing knowledge of the mechanisms of posttraumatic psychopathology will open opportunities to explore more targeted interventions, outside the range of traditional treatment-derived methods. Such targeted intervention methods could allow clinicians to focus on both specific subgroups and specific pathological processes.
Web-Based and Telehealth Tools
As our world becomes increasingly digitized and AI tools advance PTSD diagnosis, monitoring and management will necessarily include a growing component of digital approaches. As an example, voice markers from smartphones hold promise for high-throughput, low-cost universal screening. Studies of in-person Internet-delivered CBT for PTSD suggest that its efficacy is similar to that of face-to-face real-world interventions. More recently, Internet-delivered PTSD self-assessment tools have become widely distributed and extensively used as alternatives to paper-and-pencil validated rating scales. Moreover, novel psychoeducation, self-training, and intervention tools are currently available for use on all types of digital platforms. These new platforms, as well as steadily emerging ones using AI tools, hold great promise for accessible and affordable diagnostic support tools, stand-alone interventions, and therapist-assisting tools.