Abstract
Collective traumas, such as war, genocide, natural disasters, and systemic oppression, have profound and lasting effects, not only on survivors but also on their descendants. Understanding how these traumas are transmitted across generations is essential to inform effective interventions and policy responses. This systematic review aimed to synthesize quantitative evidence on the physiological and psychological outcomes observed in second-generation descendants of individuals exposed to collective trauma. We included English-language, peer-reviewed quantitative studies published between 1997 and 2022 that investigated intergenerational trauma among second-generation descendants of survivors of collective trauma. Exclusion criteria included qualitative studies, and those that involved third-generation descendants. We conducted a comprehensive search across six databases: PsycINFO, PsycARTICLES, MEDLINE, Web of Science Core Collection, Embase, and PubMed. The final search was completed in December 2022. Search terms included keywords such as “intergenerational trauma,” “transgenerational trauma,” “collective trauma,” and “historical trauma.” Two independent reviewers screened titles and abstracts, followed by full-text assessments for eligibility. Discrepancies were resolved through discussion. Study quality was evaluated using the Critical Appraisal Skills Programme (CASP) checklist. Each study was assessed independently by two reviewers, with disagreements resolved by consensus. A narrative synthesis was conducted. Out of 3,904 records identified, 18 studies met the inclusion criteria. The findings revealed that physiological changes in stress regulation and brain structure suggest biological embedding of trauma across generations. Socially, intergenerational trauma shaped relationships and identity, often fostering mistrust and emotional restraint. Psychologically, descendants showed elevated distress and trauma symptoms, with parental PTSD as a key predictor. The overall quality of evidence was limited by small sample sizes, cross-sectional designs, reliance on self-reported measures, and inadequate control for confounding factors. More longitudinal and methodologically rigorous studies are needed to better understand the pathways of trauma transmission and inform prevention and intervention strategies. This review was registered with PROSPERO (CRD42023433181).
Introduction
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) characterizes a traumatic event as an experience involving actual or threatened death, severe injury, or sexual violence. This exposure can occur in various ways, including direct involvement, witnessing the event, learning that it has happened to a close relative or friend, or repeatedly encountering distressing details related to the event [1]. Throughout history, war and violence have been persistent elements of human existence. Currently, over 65 million people worldwide have been displaced due to armed conflicts, with more than 21 million classified as refugees—over half of whom are under the age of 18. The consequences of war and violence extend beyond societal disruption, profoundly affecting individuals’ lives [2]. Veterans often suffer long-term psychological and physical health challenges following combat exposure, with Post Traumatic Stress Disorder (PTSD) being one of the most prevalent conditions. The impact of war does not only affect the veterans themselves but can also extend to their families [3]. In addition to armed conflict, natural disasters are a significant source of psychological trauma. Research indicates that up to 9% of individuals affected by natural disasters develop PTSD [4]. Other historical traumas, such as the forced displacement of Indigenous children in Canada’s Indian Residential Schools (IRSs) [5], the 1994 genocide against the Tutsi in Rwanda [6], and the institutionalized racial oppression under Apartheid in South Africa [7], have had severe and long-lasting psychological impacts on those who directly experienced them. As the next section will explore, the psychological and social consequences of such traumas often extend beyond the individuals who experienced them firsthand, impacting subsequent generations.
Research studies document that the detrimental effects of trauma can be passed down from one generation of survivors to their children and grandchildren through a phenomenon called intergenerational trauma [8]. The American Psychiatric Association defined “intergenerational trauma” as a situation in which descendants of survivors who have gone through a traumatic incident show similar unfavorable emotional and behavioral responses as those survivors [9]. These responses include feelings of low self-worth, depression, suicidal thoughts, substance abuse, dissociation, hypervigilance, intrusive thoughts, difficulties forming relationships and attachments, difficulties controlling aggression, and extreme reactivity to stress. The impacts of intergenerational trauma are not only manifested in emotional and behavioral responses but also extend to physiological changes. For example, Badel et al. found that maternal PTSD and the age at which mothers were exposed to Holocaust trauma predicted lower cortisol levels in their descendants [10]. Cortisol helps regulate the stress response, and low cortisol levels are associated with a higher predisposition to PTSD. An insufficient cortisol response during or after trauma exposure may fail to contain the stress reaction, leading to over-consolidation of traumatic memories and heightened fear responses, which further increase the risk of developing PTSD [11]. As such, understanding the impacts of intergenerational trauma on second-generation descendants is critical to inform clinical interventions, as well as to develop supportive policies tailored for descendants of trauma survivors.
This systematic review focuses on collective trauma and distinguishes it from individual trauma. Collective trauma refers to the psychological impact experienced by a group of people because of traumatic events, such as natural disasters, genocide, war, or pandemics. This form of trauma is associated with the collective’s shared experiences and emotional reactions and is closely linked to the social and cultural environment of the affected group [12]. In contrast, individual trauma arises from events that directly affect a single person, such as accidents, assaults, or family violence. Its effects are closely related to the circumstances and personal history of the individual who experiences them [13]. This review centers on collective trauma because it affects not only individuals but also entire communities. When a group experiences traumatic events, such as war, genocide, or displacement, the impact can be felt across generations. Collective trauma shapes how people see themselves, relate to others, and how society functions. Unlike individual trauma, collective trauma is distinguished by its broader social scope, its potential to influence cultural values and norms, and the interconnectedness of individual identities within the collective [14]. Understanding collective trauma is essential for developing healing strategies that reach beyond individual therapy to include education, public policy, and community-based support.
This systematic review focuses on the impacts of survivors’ trauma on second-generation descendants, distinguishing them from third-generation descendants, as the effects of trauma are notably different between the two generations. A meta-analysis conducted by Sagi-Schwartz et al. did not find any evidence of tertiary traumatization in the third generation of Holocaust survivors [15]. This study revealed that the third generation does not exhibit inferior outcomes compared to established norms or control groups in many areas, such as general adjustment, aggression, internalizing behaviors, attachment, and other psychological characteristics. Moreover, research conducted in communities has revealed lessened effects of intergenerational trauma across generations, with reduced consequences on the third generation [16].
A robust literature encompassing quantitative studies investigates the impacts of intergenerational collective trauma on second-generation descendants in various contexts, including descendants of survivors of the Holocaust, genocide, war invasions, displacement, and natural disasters. However, these studies present contradictory findings regarding whether intergenerational collective trauma directly impacts the psychological well-being of second-generation descendants. In other words, some of these studies document that trauma experienced by survivors has an impact on their descendants, while other studies refute this conclusion. For instance, Gangi et al. found that adult children of Holocaust survivors had significantly higher levels of anxiety, lower levels of self-esteem, and lower levels of inhibition of aggression compared to adult children of non-Holocaust survivors [17]. Additionally, in their study, Kim et al. found that the offspring of mothers, who experienced more significant levels of trauma during the South African Apartheid, displayed elevated psychiatric problems during late adolescence [7]. On the other hand, some studies have documented that the impacts of intergenerational trauma do not transmit from one generation to the next. For instance, Muhtz et al. found that the mental health and quality of life of adult children of parents with chronic PTSD did not significantly differ from those whose parents did not have PTSD [18]. Finally, Ingabire et al. found that there was no significant relation between both mothers’ trauma exposure and PTSD symptoms and their adult offspring’s depression or PTSD symptoms [6]. As such, it is important to systematically analyze the findings of these quantitative studies while considering their methodological limitations, including sample size, sample characteristics, study design (e.g., cross-sectional vs. longitudinal), and control of potential confounding variables.
On the other hand, while a substantial body of literature has examined the impacts of intergenerational collective trauma on second-generation descendants, the existing evidence remains scattered across various disciplines and marked by considerable variation in research designs and methodologies. Moreover, there is a relative lack of systematic reviews that synthesize these findings. To date, the literature includes one systematic review and two meta-analyses focused specifically on intergenerational collective trauma resulting from war and the Holocaust. However, no systematic reviews have been published that encompass all types of collective trauma or provide a comprehensive overview of associated outcomes. Sangalang et al. conducted a systematic review on the on the intergenerational impacts of war-related trauma among second-generation descendants of refugee families [19]. Moreover, two meta-analyses, by Payne et al. [20] and Van IJzendoorn and Sagi-Schwartz [21], examined whether children of Holocaust survivors were more likely to develop PTSD and whether they exhibited poorer adaptation, respectively. This systematic review is therefore essential to bridge existing gaps by providing a comprehensive synthesis of the diverse and fragmented body of research on intergenerational collective trauma, encompassing a broader range of trauma types and descendants’ outcomes beyond those previously explored.
In conclusion, this review examines the impacts of various forms of intergenerational collective trauma, including genocide, the Holocaust, war, historical trauma, and natural disasters, to address the research question: What are the effects of intergenerational collective trauma on the physiological and psychological outcomes of second-generation descendants? Additionally, the review discusses the limitations of the studies analysed and provides recommendations for future research to deepen our understanding of intergenerational trauma and its effects on subsequent generations.
Methodology
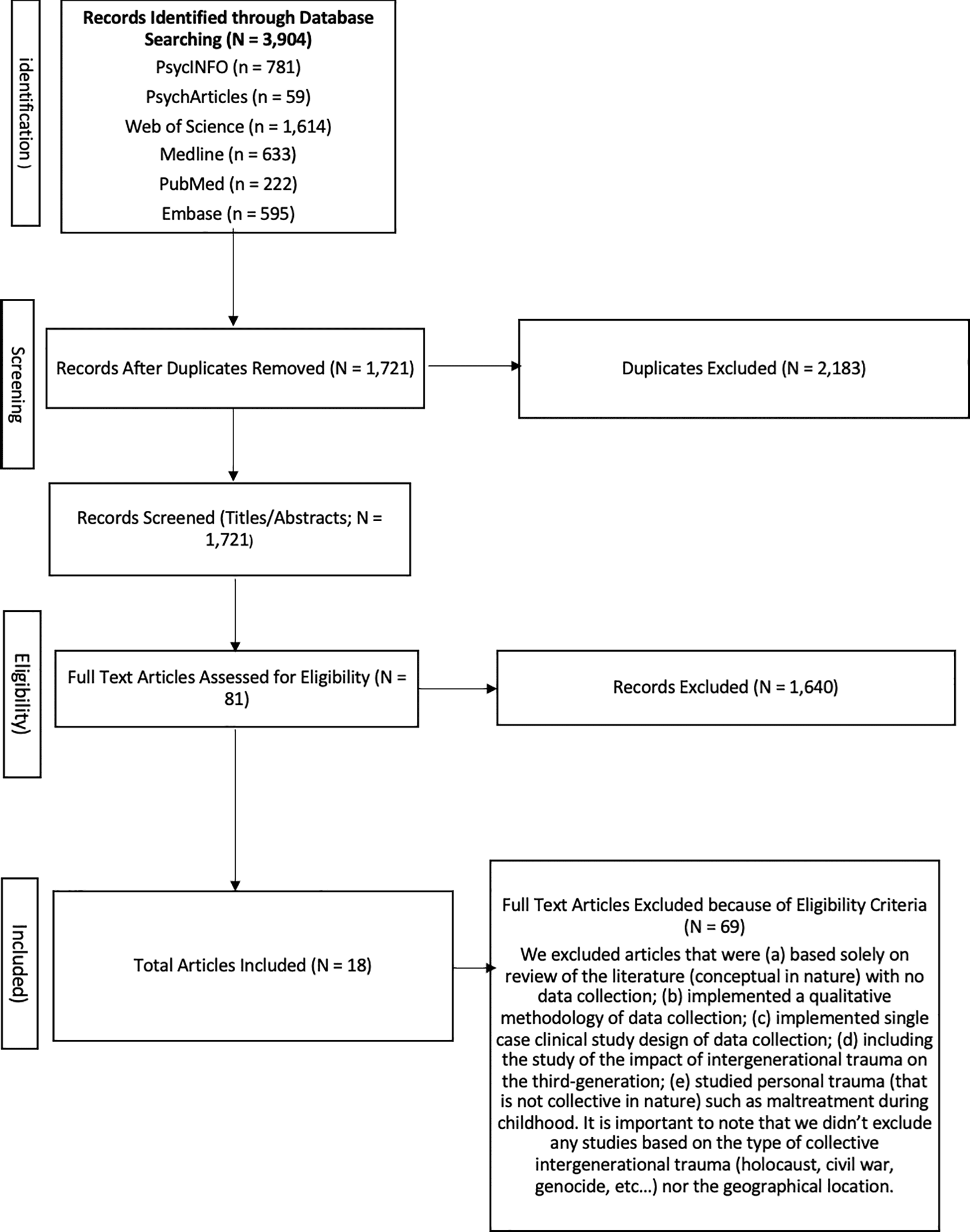
A systematic literature search was conducted between June and December 2023, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22], to identify studies on intergenerational trauma in second-generation descendants published over the past 25 years, from 1997 to 2022. This time frame was selected to balance historical depth with the inclusion of contemporary findings relevant to the evolving understanding of intergenerational trauma. We identified articles through PsychInfo (EBSCO), PsychArticles (EBSCO), Medline (EBSCO), Web of Science Core Collection (Thompson Routers), Embase (Elsevier), and PubMed (National Center for Biotechnology Information) to combine the following keywords: intergenerational trauma, transgenerational trauma, historical trauma, secondary traumatization, and collective trauma. Figure 1 contains a flowchart of the study selection. The studies were considered eligible for inclusion if they: (a) investigated the impact of intergenerational trauma (that was collective) across second-generation descendants of survivors; (b) used quantitative methodology; (c) and published in English in peer-reviewed journals. Excluded were studies (d) based solely on a review of the literature (conceptual) with no data collection; (e) implemented a qualitative methodology of data collection; (f) implemented single case clinical study design of data collection; (g) included the study of the impact of intergenerational trauma on the third-generation descendants; (h) studied personal trauma (that is not collective) such as maternal maltreatment during childhood. Exclusion of studies based on the type of collective intergenerational trauma (holocaust, civil war, genocide, etc.) or the geographical location did not occur.
In the initial search, 3904 studies were retrieved. After excluding duplicates, 1721 studies remained. Next, two researchers independently reviewed the titles and abstracts. After screening the abstracts, 93 articles remained and based on the full text, the final selection consisted of 18 studies. Regarding data extraction, the accuracy of the article extraction was reviewed by two independent authors, and any discrepancies were resolved through discussion until consensus was achieved on all studies. The two reviewers independently screened and extracted data from the 18 included studies.
Results
The final selection of studies encompasses studies that focused on the intergenerational impact of trauma on second-generation descendants. Studies that were reviews or qualitative, not specific to collective trauma, and focused on the effects of the trauma on third-generation descendants did not meet the inclusion criteria and, therefore, could not be included. The CASP quality assessment tool was used to evaluate the quality of the reviewed studies, addressing 11 specific domains: (1) stating a focused issue; (2) use of appropriate methods; (3) acceptable recruitment strategies; (4) accurate, validated measures to reduce bias; (5) data collection strategies; (6) sufficient number of participants to minimize chance; (7) presentation of results; (8) sufficiently rigorous data analysis; (9) clear statement of findings; (10) applicability to the local population; and (11) value of the research conducted [23]. Two authors independently applied the CASP tool to each included study, documenting supporting information and justifications for their risk of bias judgments. Any discrepancies in assessments or justifications were resolved through discussion until a consensus was reached. The assessment revealed that most studies met the criteria for items 1, 2, 5, 7, 8, and 9. However, shortcomings were observed in items 3, 4, 6, 10, and 11. Specifically, some studies could not implement optimal recruitment methods and had to rely on alternative approaches. Others used measures that were not standardized or did not accurately capture the intended variables. Several studies had small sample sizes, often due to the nature of the trauma being studied. Most studies lacked generalizability to the local population, and many provided only preliminary insights rather than conclusive evidence. Nevertheless, the 18 studies were included to conduct this systematic review, as they were appropriate and relevant enough in terms of research objective, data collection and implications.
Overview of study characteristics and emergent themes
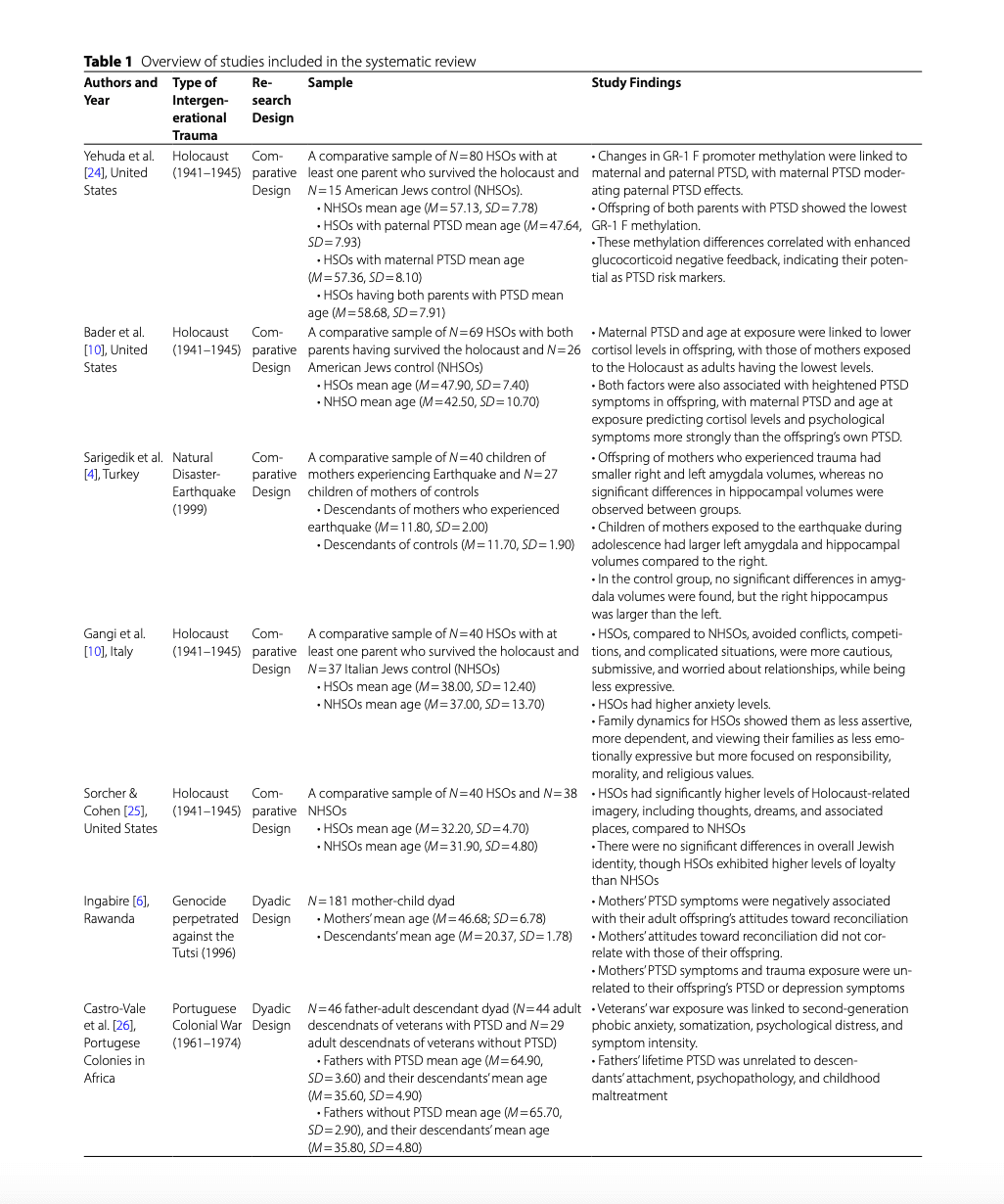
The study characteristics of the selected studies are presented in Table 1. Our review included 18 studies, all of which utilized quantitative methods. Eight studies utilized a parent-child dyadic design, recruiting one or both parents and their descendants to collect data on the trauma experienced by the survivor parents and its direct impacts on the physiological and psychological outcomes in their descendants. Ten studies used comparative analyses to compare two or more groups of descendants, such as those who are offspring of trauma survivors and those who are not, focusing on differences on physiological and psychological outcomes. The themes that emerged from our analysis highlight the impacts of intergenerational trauma on: (a) epigenetics and physiological outcomes; (b) interpersonal relationships and social identity; and (c) psychological distress and psychopathology.
Impacts of intergenerational trauma on the epigenetics and physiology of descendants
Three studies explored the epigenetic and physiological impacts of intergenerational trauma on descendants. These studies consistently demonstrated the effects of intergenerational trauma on both epigenetic and physiological outcomes in descendants. Yehuda et al. [24] and Bader et al. [10] found that offspring of Holocaust survivors with parental PTSD exhibited reduced Glucocorticoid receptor gene exon 1 F promoter region (GR-1 F) gene methylation and lower cortisol levels, respectively, while Sarigedik et al. [4] showed that children of mothers exposed to an earthquake had smaller bilateral amygdala volumes. Yehuda et al. studied Holocaust Survivor Offspring (HSOs) and Non-Holocaust Survivor Offspring (NHSOs) (N = 80 HSOs; N = 15 NHSOs) and found that reduced methylation of the GR-1 F gene promoter was associated with both maternal and paternal PTSD, with maternal PTSD moderating paternal effects; the lowest methylation levels were seen in offspring of two PTSD-affected parents, suggesting heightened vulnerability to stress via impaired glucocorticoid regulation [24]. Bader et al., comparing N = 69 HSOs and N = 26 controls, found that maternal PTSD and the age at which mothers experienced Holocaust trauma predicted lower urinary cortisol levels and greater PTSD symptoms in offspring; effects stronger than those of the offspring’s own trauma exposure [10]. Finally, Sarigedik et al. compared N = 40 children of earthquake-exposed mothers with N = 27 controls in Turkey and found significantly smaller bilateral amygdala volumes in the trauma group. Children of mothers exposed during adolescence had larger left amygdala and hippocampal volumes compared to their right counterparts; though no significant differences in hippocampal volumes were observed between the two groups [4].
Impacts of intergenerational trauma on descendants’ interpersonal relationships and social identity
Three studies explored the impacts of intergenerational trauma on descendants’ interpersonal relationships and social identity. These studies consistently demonstrated the effects of intergenerational trauma on both areas. Gangi et al. [10] found that HSOs showed higher anxiety, avoidance, and defensiveness compared to controls. Sorcher & Cohen [25] observed more Holocaust-related imagery in HSOs, but no difference in Jewish identity. Ingabire et al. [6] found that mothers’ PTSD symptoms negatively influenced their children’s attitudes toward reconciliation. Gangi et al. [10] studied the impact of Holocaust intergenerational trauma on second-generation descendants using a comparative design with 40 HSOs and 37 Italian Jewish controls (NHSOs). They found that HSOs exhibited more avoidance of interpersonal conflicts, competitions, caution, submissiveness, yielded to others and worry about personal relationships, along with less expressiveness and more defensiveness in response to depressive feelings. HSOs also had higher anxiety levels than NHSOs, perceived themselves as less-sufficient and assertive, and perceived their families as less emotionally expressive and more focused on responsibility, morality, and religious values. Finally, in comparison to their actual families, HSOs described the ideal family as more accepting to challenges and more oriented toward competition, compared to NHSOs [10]. Sorcher & Cohen [25] compared 40 HSOs and 38 NHSOs descendants. HSOs had significantly higher levels of Holocaust-related imagery, including thoughts, dreams, and memories of related places, but no significant difference was found in overall Jewish identity between the two groups. HSOs also reported higher levels of loyalty [25]. Finally, Ingabire et al. [6] examined intergenerational trauma from the 1994 Rwandan genocide with 181 mother-child dyads. The study found that mothers’ PTSD symptoms were negatively associated with their adult children’s attitudes toward reconciliation, indicating a link between parental mental health and second-generation attitudes in post-conflict societies. However, there was no direct association between mothers’ attitudes toward reconciliation and those of their offspring, suggesting that the negative attitudes were driven by witnessing their mothers’ psychological distress rather than mimicking their views [6].
Impacts of intergenerational trauma on descendants’ psychological distress and psychopathology
Thirteen studies examined the impact of intergenerational trauma on descendants’ psychological distress and psychopathology. They were categorized by trauma type: three focused on war-related trauma in veterans’ families, two on war-related trauma in refugees, five on genocide, and three on the Holocaust, apartheid, and residential schools.
War veterans’ families
Three studies explored the impact of intergenerational trauma on descendants’ psychological distress and psychopathology in war veterans’ families. Two studies, Castro-Vale et al. [26] and O’Toole et al. [3], consistently demonstrated effects in both areas, while Wasterink and Giarratano [27] did not find such effects, likely due to the small sample size.
Castro-Vale et al. [26] examined intergenerational trauma in 46 Portuguese war veterans, 44 adult children of veterans with PTSD, and 29 of those without. Some families contributed multiple children. Veterans’ trauma exposure was linked to their children’s phobic anxiety, somatization, overall psychological distress, and symptom intensity. However, fathers’ lifetime PTSD was not associated with descendants’ attachment styles, psychopathology, or childhood maltreatment. The authors suggest that higher educational attainment among children may have helped them cope with their fathers’ PTSD, though they were still affected by its emotional burden [26].
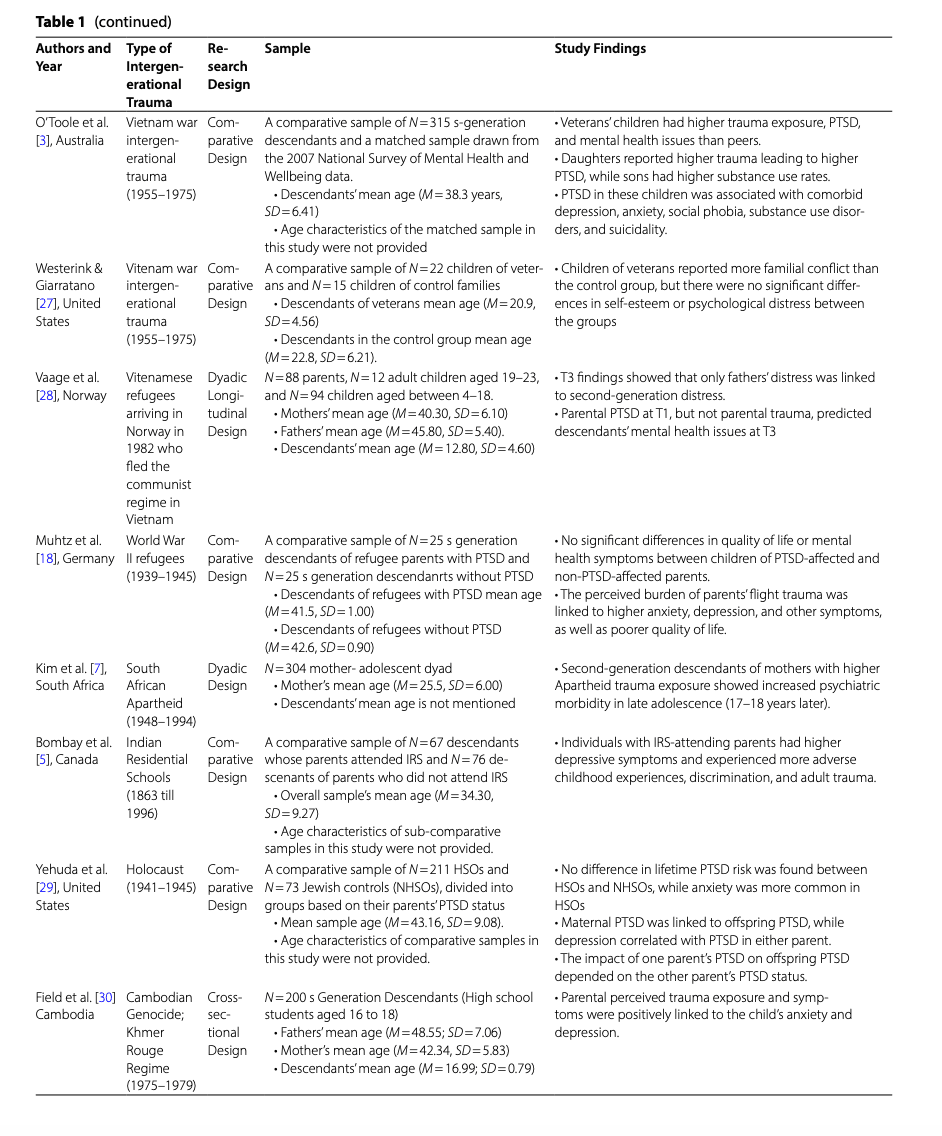
O’Toole et al. [3] and Wasterink and Giarratano [27] both investigated the intergenerational effects of Vietnam War trauma on veterans’ children but reported differing outcomes, largely due to sample size. O’Toole et al., using a large sample of 315 descendants, found significantly higher trauma exposure, PTSD, and mental health issues among veterans’ children compared to matched controls, despite stable family environments. Gender differences emerged, with daughters experiencing more trauma and PTSD, and sons exhibiting higher substance use [3]. In contrast, Wasterink and Giarratano studied a smaller sample of 21 children of veterans with PTSD and 14 controls. While children of veterans reported increased familial conflict, no significant differences were found in self-esteem or psychological distress. The authors acknowledged the limited sample size as a key constraint, suggesting their findings should be viewed as preliminary [27].
War refugees
Vaage et al. [28] and Muhtz et al. [18] both examined intergenerational trauma among refugee families. Both studies showed that intergenerational trauma among refugees impact the psychological distress and psychopathology of descendants. Vaage et al. examined intergenerational trauma in 88 Vietnamese refugee parents, 12 adult children (aged 19–23 years), and 94 children (aged 4–18 years) resettled in Norway, with data collected at arrival (1982, T1), follow-up (1985, T2), and 23 years later (T3). T3 findings showed that paternal, but not maternal, psychological distress was significantly associated with second-generation distress, possibly due to strong father-child bonds in South Asian cultures. PTSD at T1 predicted mental health problems in descendants at T3, though overall parental trauma at T1 did not. Despite 30% of fathers having PTSD, descendants were more resilient than Norwegian peers [28]. Muhtz et al. studied 25 s-generation descendants of WWII refugees with PTSD and 25 without, all from former eastern German territories. They found that perceived burden from parental trauma, not PTSD diagnosis, was linked to poorer mental health and quality of life, especially in areas like pain, physical functioning, and emotional wellbeing. No significant differences were found between children of PTSD and non-PTSD parents when compared as distinct groups. These findings suggest that the intergenerational impact of trauma may be shaped more by how the trauma is emotionally experienced and interpreted by the next generation than by the presence of parental PTSD alone [18].
Apartheid, residential school, and holocaust
Although Kim et al. [7] Bombay et al. [5] and Yehuda et al. [29] investigated the intergenerational impacts of three distinct traumas; South African Apartheid, Indian Residential Schools (IRS), and the Holocaust, their findings converge on key psychological outcomes in second-generation descendants. Kim et al. [7] investigated the impact of trauma during South African Apartheid in a sample of 304 mother-adolescent dyads drawn from the largest and longest-running longitudinal birth cohort study on child development and health in Africa. Their results showed that adolescents whose mothers experienced higher levels of trauma during Apartheid displayed increased psychiatric morbidity in late adolescence, 17 to 18 years after the exposure to prenatal stress, highlighting the lasting intergenerational effects of maternal trauma. Similarly, Bombay et al. [5] examined the intergenerational impact of trauma associated with the Indian Residential School (IRS) system by comparing second-generation descendants of IRS survivors (N = 67) with those whose parents had not attended IRS (N = 76). The study found that descendants of IRS survivors experienced higher levels of depressive symptoms, greater exposure to adverse childhood experiences, adult trauma, and discrimination, despite having comparable levels of education and income to the comparison group. Finally, Yehuda et al. [29] examined the psychiatric outcomes of HSOs compared to NHSOs in the U.S. HSOs showed higher levels of depression, anxiety, and, to a lesser extent, substance use disorders. While PTSD rates did not differ overall between groups, maternal PTSD was consistently associated with offspring PTSD, regardless of paternal PTSD status. Both maternal and paternal PTSD were linked to increased depression in offspring. Anxiety was more common among all HSOs, regardless of parental PTSD. Paternal PTSD influenced offspring PTSD only when maternal PTSD was also present, whereas maternal PTSD had a stronger and independent effect, amplified by the presence of paternal PTSD.
Genocide
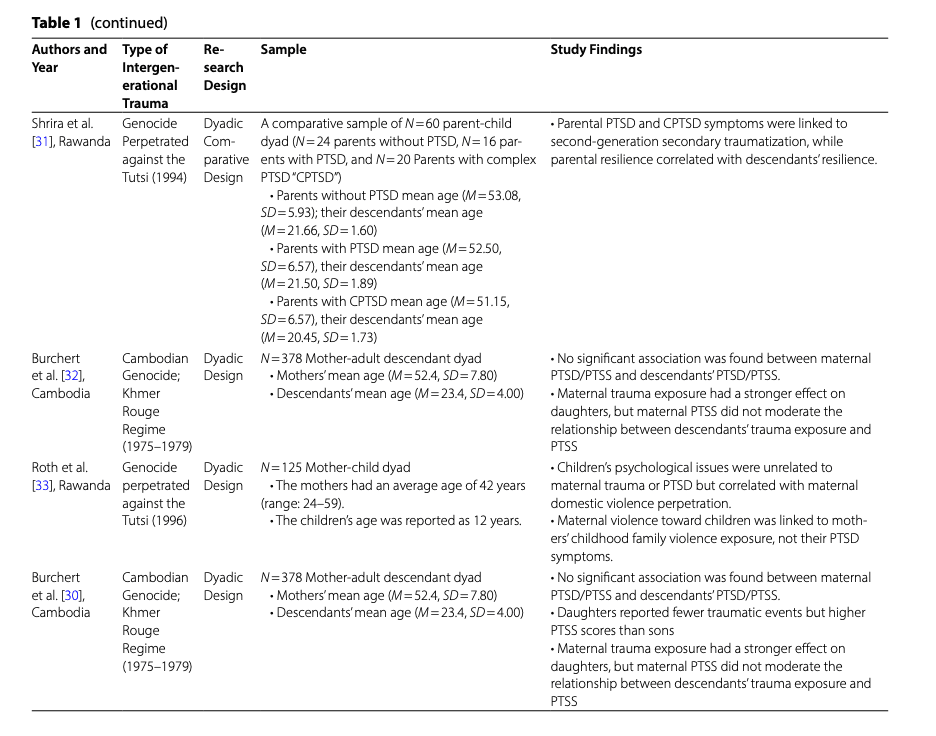
Three studies have explored the intergenerational transmission of trauma stemming from the Cambodian genocide, revealing both converging and diverging findings. Field et al. [30] using a sample of 200 high school students, found that adolescents’ levels of anxiety and depression were positively associated with their perceptions of both paternal and maternal trauma exposure and symptoms. Similarly, Shrira et al. [31] in a study involving 60 parent-child dyads, reported that parental PTSD and Complex PTSD were linked to greater secondary traumatization and reduced resilience among second-generation descendants. They also found that parental resilience was positively correlated with increased resilience in their children, suggesting a potential buffering effect. In contrast, Burchert et al. [32] analyzing data from 378 Cambodian mother-child dyads, found no significant association between maternal PTSD/PTSS (Post Traumatic Stress Symptoms) and the PTSD/PTSS symptoms of their children. This divergence may be attributed to differences in measured outcomes: while Field and Shrira focused on broader psychological effects such as anxiety, depression, and resilience, Burchert et al. specifically assessed trauma-related symptoms (PTSD/PTSS) and found no direct transmission. This suggests that while parental trauma may influence general emotional well-being and coping capacity in children, it may not always manifest in trauma-specific disorders, underscoring the importance of distinguishing between different psychological outcomes when studying intergenerational trauma.
Roth et al. [33] and Ingabire et al. [6] both examined intergenerational trauma stemming from the 1994 Rwandan genocide in mother-child dyads (N = 125 and N = 181, respectively). Both studies found no significant association between maternal trauma exposure or PTSD and their children’s psychological symptoms, general psychological issues in Roth et al., and PTSD and depression in Ingabire et al., after accounting for the child’s own trauma. However, Roth et al. observed that children’s psychological problems were significantly associated with maternal perpetration of domestic violence, which was itself linked to the mothers’ own childhood exposure to violence rather than their PTSD symptoms [33]. Ingabire et al. further emphasized that maternal PTSD was unrelated to adult offspring’s mental health but previously found it influenced their attitudes toward reconciliation. Both studies highlight a key limitation, notably the lack of data on paternal mental health, which may play a crucial role in shaping intergenerational outcomes [6].
Discussion
This review aimed to investigate the impacts of intergenerational trauma on second-generation descendants. We conducted a systematic literature search and included 18 quantitative studies, published between January 1997 and December 2022, that examined the intergenerational impact of trauma on second-generation descendants. Studies focusing on third-generation effects, qualitative or review-based approaches, or non-collective designs were excluded. The CASP quality assessment revealed that while most studies had clear aims, rigorous analyses, and reliable data collection, limitations were noted in recruitment methods, measurement validity, sample size, generalizability, and practical applicability. Despite these limitations, all included studies were deemed sufficiently relevant to the research objectives. The reviewed studies employed either a parent-child dyadic design or comparative group analyses. Three central themes emerged across studies: (a) epigenetic and physiological outcomes; (b) interpersonal relationships and social identity; and (c) psychological distress and psychopathology; highlighting the multifaceted and enduring impacts of intergenerational trauma.
Parental trauma and descendants’ physiological changes
Emerging evidence highlights the physiological and epigenetic consequences of intergenerational trauma. Three studies consistently demonstrate that trauma exposure in parents can alter stress-related biological systems in their offspring. Yehuda et al. and Bader et al. documented that offspring of Holocaust survivors with parental PTSD showed reduced GR-1 F gene methylation [24] and lower cortisol levels [10], respectively, markers of impaired glucocorticoid regulation and heightened stress sensitivity. Reduced methylation of the GR-1 F gene leads to increased expression of glucocorticoid receptors. This means the body becomes more sensitive to cortisol. As a result, the negative feedback loop in the Hypothalamic Pituitary Adrenal (HPA) axis becomes more active, leading to reduced production of cortisol after stress [24, 34]. Cortisol plays a crucial role in regulating the stress response and modulating memory consolidation, particularly in relation to traumatic events, with lower levels being associated with heightened vulnerability to PTSD. When the cortisol response is insufficient during or after trauma, it may fail to adequately contain the stress reaction, resulting in the over-consolidation of traumatic memories and increased fear responses. Additionally, low cortisol levels can impair the body’s ability to effectively shut down the stress response, contributing to chronic hyperarousal and heightened anxiety commonly observed in post-traumatic stress disorder [35,36,37]. Similarly, Sarigedik et al. found that children of earthquake-exposed mothers had significantly smaller amygdala volumes, with developmental timing of maternal trauma influencing neural outcomes [4]. The amygdala region is central to processing emotions such as fear and threat detection. A reduced amygdala volume has been associated with impaired emotional regulation and an overactive stress response, characterized by heightened reactivity to perceived threats even in non-threatening environments. This dysregulation may increase vulnerability to psychological disorders, including post-traumatic stress disorder (PTSD) [38, 39].
Impacts of intergenerational trauma on descendants’ interpersonal relationships and social identity
Intergenerational trauma appears to shape both interpersonal relationships and social identity in descendants. Gangi et al. found that offspring of trauma survivors have been found to exhibit heightened anxiety, avoidance, and interpersonal defensiveness, along with perceptions of their families as less emotionally expressive and more morally rigid [10]. Sorcher & Cohen also reported that descendants exhibited increased trauma-related imagery and a stronger sense of loyalty, despite no significant changes in broader identity markers [25]. In other contexts, such as post-genocide societies, Ingabire et al. found that parental PTSD symptoms have been linked to more negative attitudes toward reconciliation among descendants, likely shaped by witnessing psychological distress rather than directly adopting parental views [6]. These findings suggest that parental trauma can subtly influence how descendants relate to others and construct their social identities. This is consistent with existing research on the effects of the Holocaust and genocide, which shows that intergenerational trauma can have a significant impact on feelings of mistrust and fear toward others [39, 40].
Impacts of intergenerational trauma on descendants’ psychological distress and psychopathology
The impact of intergenerational trauma on descendants’ psychological distress and psychopathology has been widely explored across various trauma types, including war-related trauma, genocide, and experiences related to the Holocaust, apartheid, and residential schools. These studies collectively highlight significant psychological consequences for descendants, although the findings vary based on the specific type of trauma.
In the context of war veterans’ families, several studies have shown that the trauma experienced by veterans, particularly those with PTSD, significantly affects their children. For instance, Castro-Vale et al. [26] found that children of veterans with PTSD exhibited increased psychological distress, including phobic anxiety and somatization. Similarly, O’Toole et al. [3] observed heightened levels of PTSD and trauma exposure among children of Vietnam War veterans. However, Wasterink and Giarratano [27] found no significant psychological distress in children of veterans, a result they attributed to the small sample size. Overall, the studies on war veterans’ families consistently show that the psychological toll of war extends beyond the combatants themselves, affecting the emotional wellbeing of the next generation.
The studies on war refugees further emphasize the enduring effects of intergenerational trauma on descendants. Both Vaage et al. [28] and Muhtz et al. [18] found that the trauma experienced by refugee parents, particularly those with PTSD, had a profound impact on their children’s mental health. Vaage et al. highlighted that paternal trauma was particularly influential on second-generation distress, likely due to the strong father-child bond in many cultures. In contrast, Muhtz et al. noted that the emotional burden perceived by children, rather than the presence of PTSD in parents, was a stronger predictor of poor mental health outcomes in the next generation. These findings suggest that the emotional interpretation and perceived burden of trauma by descendants may play a more significant role in shaping their psychological distress than the mere presence of PTSD in parents.
The studies on the Holocaust, apartheid, and residential schools also reveal notable psychological outcomes in descendants. Kim et al. [7] found that adolescents whose mothers experienced high levels of trauma during apartheid showed increased psychiatric morbidity, highlighting the lasting effects of maternal trauma. Similarly, Bombay et al. [5] reported that descendants of Indian Residential School survivors exhibited more depressive symptoms and adverse childhood experiences. Yehuda et al. [29] found that Holocaust survivor offspring experienced higher levels of depression and anxiety, with maternal PTSD being a particularly strong factor in the transmission of these symptoms.
Studies on the intergenerational transmission of trauma following the Cambodian and Rwandan genocides present a complex and nuanced picture. Research on the Cambodian genocide indicates partial transmission of trauma-related effects across generations, though findings vary depending on the psychological outcomes assessed. Field et al. [30] and Shrira et al. [31] found that parental trauma, especially PTSD and Complex PTSD, was linked to heightened anxiety, depression, and reduced resilience in children, with parental resilience serving a potential protective function. In contrast, Burchert et al. [32] found no direct association between maternal PTSD/PTSS and similar symptoms in offspring, suggesting that trauma may influence broader emotional well-being without necessarily resulting in diagnosable trauma-specific disorders. These discrepancies highlight the importance of distinguishing between general psychological distress and clinical trauma symptoms when assessing intergenerational impacts. Similarly, studies on the Rwandan genocide (Roth et al. [33]; Ingabire et al. [6]) found no significant direct link between maternal trauma or PTSD and the psychological symptoms of their children, once the child’s own trauma exposure was considered. However, Roth et al. noted an indirect pathway, where maternal experiences of childhood violence, rather than their PTSD, were associated with both perpetration of domestic violence and their children’s psychological difficulties. Ingabire et al. also highlighted that maternal PTSD influenced offspring’s reconciliation attitudes, pointing to more subtle, value-based transmissions. It is conceivable that the way a society responds after genocide significantly influences how trauma is passed down through generations. In Rwanda, timely initiatives focused on recognition, justice, and reconciliation have contributed to reducing the transmission of trauma to descendants [41]. Meanwhile, Cambodia’s slower and less comprehensive approach has likely intensified the intergenerational effects of trauma, worsened by ongoing silence and insufficient mental health support [42].
Methodological issues
This study’s strength lies in its systematic analysis of all empirical studies on intergenerational trauma published over the past 25 years. We evaluated a range of factors that were only partially addressed in previous reviews. However, despite focusing solely on quantitative research, our findings highlight significant heterogeneity in sample types and measurement instruments across studies making direct comparisons and drawing unified conclusions. Moreover, only a small number of researchers have investigated intergenerational trauma, and many studies had findings that were not widely generalizable, requiring cautious interpretation. Furthermore, the nature of collective trauma itself may influence its intergenerational effects differently, emphasizing the need to examine specific trauma types separately, rather than assuming a uniform mechanism of transmission. Studies predominantly relied on cross-sectional designs which impede the ability to draw causal inferences about the impact of intergenerational trauma. Longitudinal studies are crucial for identifying causal pathways and understanding how intergenerational trauma evolves [43, 44]. Furthermore, small sample sizes in several dyadic and comparative studies undermine the statistical power and generalizability of their findings, making it difficult to extend conclusions beyond the studied populations [45, 46]. The studies also failed to account for parental exposure to other forms of trauma and confounding variables potentially skewing the observed associations. The exclusive recruitment from non-clinical settings may also lead to an underestimation of the clinical significance of intergenerational trauma [6]. Lastly, the reliance on self-report measures, where some were not standardized, raises concerns about the validity of the reported psychopathology [47].
Recommendations for clinical practice
This systematic review sought to answer the research question: Does intergenerational collective trauma impact the physiological and psychological outcomes of second-generation descendants? The evidence synthesized from 18 quantitative studies strongly supports the notion that intergenerational trauma can profoundly affect second-generation descendants across multiple domains. Physiologically, trauma-related changes in stress regulation systems and brain structures were observed, suggesting biological embedding of trauma across generations. Socially and relationally, intergenerational trauma shaped interpersonal dynamics and influenced social identity formation, often fostering mistrust, emotional restraint, and heightened moral rigidity. Psychologically, descendants exhibited heightened levels of distress, anxiety, depression, and trauma-related symptoms, with parental PTSD emerging as a significant predictor.
To address intergenerational trauma effectively, a multifaceted approach is required, incorporating therapeutic interventions and community initiatives. Emerging physiological and epigenetic evidence; such as reduced cortisol levels, altered glucocorticoid receptor gene methylation, and smaller amygdala volumes, suggests that descendants of trauma survivors may have heightened biological sensitivity to stress and impaired emotional regulation. These findings underscore the need for trauma interventions that are not only psychologically informed but also biologically attuned. Recent studies examining the impact of trauma-focused psychotherapy, including Trauma Focused- Cognitive Behavior Therapy and EMDR (Eye Movement Desensitization and Reprocessing), have begun to show promise in reversing some of these biological effects, such as normalizing stress hormone levels and modulating epigenetic markers [48, 49]. As such, therapeutically, mental health professionals should integrate such interventions that address the epigentic and physiological imprints of intergenerational trauma and support regulation of the stress response. Addditionally, early screening for heightened biological stress sensitivity—even in individuals without direct trauma exposure—can inform personalized treatment planning. This is especially relevant for populations with intergenerational trauma histories, where inherited physiological vulnerabilities may not be immediately visible but still significantly influence mental health outcomes. Mental health practitioners must also develop a comprehensive understanding of the cultural and historical contexts that shape the transmission of intergenerational trauma and its effects on second-generation descendants. A trauma-informed care framework is crucial, recognizing the profound impact trauma has on a descendant’s well-being. Mental health professionals are encouraged to proactively assess exposure to intergenerational trauma during the trauma narrative evaluation, ensuring that therapeutic interventions are tailored to the ways in which intergenerational trauma influences an individual’s psychological well-being, social identity, and potential psychopathological development. Moreover, this approach necessitates that family therapists examine intergenerational patterns of behavior and communication, which may perpetuate the cycle of trauma. At the community level, psychoeducation and awareness campaigns can play a significant role in improving understanding of intergenerational trauma, empowering communities to adopt effective strategies to mitigate its impact. Finally, advocating for policies that address the root causes of trauma, such as poverty, inequality, and systemic violence, is essential to this comprehensive effort.