Abstract
Contextual processing is implicated in the pathophysiology of addictive disorders, but the nature of putative deficiencies remains unclear. We assessed some aspects of contextual processing across multimodal experimental procedures with detoxified subjects who were dependent on opioids (n = 18), alcohol- (n = 20), both opioids and alcohol (n = 22) and healthy controls (n = 24) using a) facial- and b) emotionally laden images; c) gambling task and d) sucrose solutions. Healthy subjects displayed consistent response pattern throughout all categories of the presented stimuli. As a group, dependent subjects rated (i.e., valuated) attractive and average faces respectively more and less attractive in comparison to controls. Dependent subjects' motivational effort, measured in the units of computer keypress to determine the attractive faces' viewing time, accorded the valuational context but was diminished relatively to the average faces’ valuation. Dependent subjects’ motivational effort for pleasant and aversive images respectively mirrored the attractive and average faces; their neutral images’ motivational effort was incongruent with the valuational context framed by the intermixed images. Also, dependent subjects’ emotional responses to counterfactual comparisons of gambling outcomes were unmatched by the riskiness context. Moreover, dependent subjects failed to show greater liking of sweet solutions that normally accompanies low sweetness perceptual context indicative of higher sucrose concentration needed for maximal hedonic experience. Consistent differences among the dependent groups (opioid vs. alcohol vs. comorbid) on the above procedures were not observed. The present findings suggest that opioid and/or alcohol dependence may be associated with amplified hedonic and motivational valuation of pleasant stimuli and with a disrupted link between behavioral/emotional responsivity and contextual variations. Further research is warranted to unravel the distinctive features of contextual processing in opioid- vis-à-vis alcohol addiction and how these features may interrelate in comorbid conditions.
Introduction
Opioid misuse is an ominous public health problem with over 16 million addicted people worldwide bringing about heightened morbidity, mortality with annual overdose deaths surpassing 100,000 in the United States alone and the numbers are rising globally. The fact that these numbers are continuously growing calls for novel insights that may inform improved prevention, diagnosis and treatment for the afflicted people. The inquiry into addictive effects of opioids and other substances alike has pointed to both tolerance and sensitization effects altering the function of the brain mesolimbic dopaminergic circuits subserving reward, an intervening variable linking a pleasant value attributed to a goal-object with a motivation, behavior or an internal emotional/physical state.
All other things being the same, many goal-objects may interchange pleasant, aversive or neutral value predicated upon the memorized or perceived contextual factors. Contextual processing thus constitutes a key element of mental function that has evolved beyond immediate survival to support an instantaneous and effortless responsivity to any type of stimuli. In humans, contextual processing has become crucial for most individual and social activities including emotional attachments, group affiliations, free will as well as conformity and obedience to societal norms and edicts. Context-based choices, judgements or decision-making touch almost every facet of personality through enthusiasm, spontaneity, adaptability, motivation, esthetic awareness and risk attitudes. Consequently, lives of people with impaired contextual processing may be difficult because they must cope with the same challenges as others, but without many of the contextually framed achievements and memories, to the point of mounting stress, burnout, and exhaustion.
In view of that, examination of neurocircuitries for opioid- and other groups of substance use disorders reveals overlapping differences between patients and control groups in the brain regions that are implicated in contextual processing. Discounting of big, delayed rewards over smaller yet immediate ones is the most extensively investigated type of contextual processing in opioid addiction. Such delay discounting is only part of a contextual processing constellation and so this work commensurates the clinical impressions of impulsivity, that is, stimulus-driven unplanned and uncontrollable behavioral responsivity to internal/external stimuli notwithstanding the contextual background in the form of negative or disadvantageous consequences.
Several lines of evidence link opioid addiction to contextual processing dysfunction. On the biochemical level, nociception opioid peptide receptors participate in contextual fear acquisition. Naltrexone, a μ-opioid antagonist, acutely altered the effects of contextual cues and valuational assessments of the presented images in unmedicated depressed patients. From a clinical perspective, “contextual healing” of placebo is defined in part by the endogenous opioidergic system while opioid addiction is characterized by insensitivity to social-, safety- and sensory contexts leading to impairments in the interpersonal sphere, to risky behaviors and to catastrophizing of pain. With regard to the underlying neurobiology, contextual dysfunction may be derived from the impaired top-down- and/or bottom-up- interactions between cortical and subcortical structures respectively mediating cognitive and emotional functions.
Despite suggestive clinical experience and supportive animal data, we are unaware of prior studies that comprehensively assessed contextual processing in opioid addiction. Contextual processing inquiry is complicated by its tentative accessibility to self-reports and by a paucity of laboratory-based procedures that induce robust and reproducible activation of the systems involved and can be controlled with respect to the ‘amount’ of the administered stimulus. To that end, we have developed a protocol comprised of three categories of stimuli, namely, (a) sets of images (e.g., faces, objects or scenes) that are differentially pleasant and aversive as measured by subjects’ willingness to physically work via computer keypress to continue viewing them; (b) monetary gains and losses incorporated into a gambling task; and (c) Sweet Taste Test (STT). The complimentary nature of these tasks is derived from their ability to capture distinct aspects of contextual processing including flexibility as the images are attributed alternating motivational contexts in relation to the characteristics of other images with which they are intermixed along with controlled expectation component of the monetary outcomes and lack of performance confounds associated with the STT allowing administration of equivalent intensity stimuli in health and in opioid addiction entailing motivational and attentional deficits that may undermine performance on cognitive/behavioral tasks.
The aim of the present study was threefold: (1) To examine the consistency of the normative contextual processing function across the distinct categories of stimuli within the same healthy individuals; (2) To determine opioid dependence-related contextual processing alterations in comparison to healthy controls; and (3) To assess the specificity of potential contextual processing changes in subjects with opioid dependence by comparing them to cohorts of subjects with dual opioid/alcohol- and alcohol alone dependence where the opioid system is critically implicated including allelic variations in specific opioid genes e.g., OPRM1.
It was hypothesized that there will be a generalized contextual response in controls that is not observed in detoxified subjects due to prolonged effects of addictive substances. Because opioidergic neurotransmission is implicated in contextual processing, a priori emphasis was placed on opioid dependence. Potential differences among the dependent groups (opioids, alcohol, and opioids + alcohol) were analyzed in an exploratory fashion. Additionally, the commonly accepted psychological notion that active avoidance of punishment is rewarding and reinforcing led us to wonder whether the reinforcement context (negative vs. positive) produces quantitatively and qualitatively different responses. Heightened effect of the aversive conditioning and negative reinforcement would be consistent for the well described normative tendency to assign greater weight to a loss than to a gain of equal magnitude.
Material and methods
Subjects
Sixty subjects carrying the diagnosis of opioid (i.e., heroin) dependence (n = 18), alcohol dependence (n = 20), alcohol dependence with fully remitted opioid dependence (n = 22) henceforth dually diagnosed were recruited from the inpatient department of the Leningrad Regional Center of Addictions (LOND), a 300-bed hospital for treating patients with substance addictions residing in the Leningrad Region, Russian Federation. Healthy control subjects (n = 24) were recruited by word of mouth and flyers distributed on the premises of the St. Petersburg State Pavlov Medical University and affiliated Medical Centers. After the procedures were fully explained, all subjects gave written informed consent to the protocol approved by the Institutional Review Board at St. Petersburg Pavlov State Medical University.
Prior to the commencement of the study, the Russian and the US study teams held a series of meetings to assess the treatment milieu, to establish protocol procedures, and to conduct training on the administration of the computerized tasks. The psycho-diagnostic and -metric tools were translated into Russian via a forward-and-backward translation process, by two independent interpreters with subsequent approval by five MD, PhD level addiction experts highly proficient in spoken and written English. The Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) diagnoses of opioid- and alcohol use disorders were established via the best estimate format utilizing all available sources of information, including a clinical interview by an MD Research Addiction Specialist, past medical records, informants’ interviews, Structured Clinical Interview for DSM-IV-TR Axis I Disorders and the Addiction Severity Index (ASI). Participants’ good physical health was ascertained by physical examination, electrocardiogram, screening blood work-up and urinalysis. Psychiatric symptoms and their impact on subjects’ life were rated with the respective Brief Psychiatric Rating Scale (BPRS) and Global Assessment of Functioning (GAF). Eating behavior was assessed by the Three-Factor Eating Questionnaire (TFEQ) namely, cognitive restraint of eating (TFEQ Factor I), disinhibition (TFEQ Factor II) and hunger (TFEQ Factor III).
Heterosexual men were included to adjust for inter-gender variability in response to the facial and emotional images. Other inclusion criteria were GAF > 60, any BPRS’ symptom rating 〈 5, total raw score of 〉 18 points on the Raven's Progressive Standard Matrices V 2.0. Urine toxicology screens were used to rule out recent drug and alcohol consumption at the time of testing; the latter was also ruled out via breathalyzer. Opioid dependent subjects were included if their average alcohol consumption did not exceed 3.5 ounces per week and/or 3.5 ounces per month on a single occasion. The lifetime-use of illicit drug by the included alcohol dependent subjects did not exceed 10 times. Healthy controls were included if consumed up to 3.5 ounces of alcohol per week and/or up to 3.5 ounces on a single occasion per month; their allowed lifetime illicit drug use was limited to 10 times.
Subjects were excluded based on diagnoses of bipolar disorder, schizophrenia spectrum disorder, major depression, drug dependence (other than on alcohol and/or heroin, as appropriate), or eating disorder. Also excluded were subjects with symptoms of drug/alcohol withdrawal or potentially confounding medical conditions (e.g., diabetes mellitus, other endocrinopathy, chronic obstructive pulmonary disease, congestive heart failure, hepatitis, hepatic failure, cirrhosis, end-stage kidney disease, neurological conditions (e.g., seizure disorder, head trauma accompanied by amnesia or loss of consciousness greater than 5 min, past brain surgery, multiple sclerosis, or Parkinson's disease), use of opioid antagonists or agonists other than heroin (as appropriate) or use within the past month of any potentially confounding psychotropic medications or drugs (e.g., barbiturates, antidepressants, psychostimulants, cannabinoids, dopaminergic or antidopaminergic agents, and mood stabilizers).
Experimental design
Therapeutic protocol
At LOND, the standard inpatient therapeutic protocol is comprised of three stages viz., detoxification, stabilization and rehabilitation performed on respective specialized units followed by long-term ambulatory care. Alcohol detoxification lasts 5–7 days and includes benzodiazepines, vitamins (folate and thiamine) and isotonic saline solutions. Heroin detoxification duration ranges 7–14 days and it builds upon pharmacotherapy with clonidine, non-steroidal anti-inflammatory drugs and loperamide. Inpatient rehabilitation program lasts 2–4 weeks and it includes individual and group therapy with cognitive-behavioral-, twelve-step facilitation-, solution-focused- and occupational therapy components. Vocational therapy for subjects with alcohol dependence involves work on a nearby factory or at LOND with mandatory return to the unit by 5 pm; opioid dependent subjects only work at the LOND premises. Returning from work subjects undergo mandatory breathalyzer and toxicology screenings.
Research protocol
Subjects meeting all criteria participated in the present study after 3 weeks of detoxification and stabilization, at least 7 days after the discontinuation of the pharmacotherapy for alcohol and/or heroin withdrawal symptomatology. They reported at 8 am on the day of the study to the LOND research unit after having fasted and refrained from teeth brushing, caffeine intake and strenuous physical activity for 10 h. Four sets of experiments were organized for completion over 4 h. The three psychosocial stimuli tasks wherein seated subjects viewed the stimuli and self-ratings questions on a computer monitor were performed before the STT. They were separated from the STT by 1 hour rest period and administered over one session in the following order: facial-, International Affective Picture System (IAPS)- and monetary stimuli. Subjects were asked not to smoke an hour prior to STT to avoid taste alteration. The subjects and the examiners were ‘blind’ to the study's hypotheses.
Facial stimuli
There were two tasks administered in separate runs: a keypress task, followed by an image attractiveness rating task. The former task was analogous to a Skinner box, in that subjects could bar-press to keep pictures visible longer or bar-press to diminish the time they were viewed. The keypress experiments comprise a response scale (i.e., effort) that is the same across different types of emotional-content images. The extent and rate of response with the keypress method is determined by the experimental subjects and thus, by definition, corresponds directly to external behavior. Also, unlike regular choice procedures yielding one data point per respondent, the keypress method provides a continuous response scale while this response type is incentive compatible, which means that subjects’ best strategy is to respond in a way that best reflects their internal state not entirely accessible to conscious awareness. Since this methodology directly collates the keypresses effort an individual subject expends to observe or not observe an image, it is a quantitative measure of motivational valuation of the stimulus by the subjects. Such valuation resembles the traditional concept of reinforcement reward, and further have some correspondence to the concept of “wanting” that has been juxtaposed to hedonic valuation i.e., “liking” reflected in the hedonic rating of the presented images.
Subjects were presented with 80 non-famous human faces that were selected from print media and classified according to pilot test results in the following four categories of 20 each: average female, attractive female, average male, and attractive male. Attractive faces of the opposite- vs. same sex are respectively perceived as pleasurable and aversive by heterosexual males. The pictures were digitized at 600 dpi in 8-bit grayscale, spatially downsampled, and cut to fit in an oval “window” sized 310–350 pixels wide by 470 pixels high using Photoshop 4.0 software (Adobe Systems). Subjects were informed that the entire task duration was fixed and independent of their actions but that they could control the viewing time of each individual picture. Within each gender block, the average and attractive faces were presented intermingled, in random order allowing the isolation of the contextual attractiveness factors. It was explained to the subjects that they could keep the viewing time at 8 s for a face by not pressing any key, or either increase or decrease this time (depending upon the frequency of the key presses) by alternately pressing a keyboard's “n” and “m,” or “z” and “x” keys, respectively. The former key presses were scored as positive, and the latter as negative yielding negative the total net number for each trial. The relationship between the key press effort and the viewing time is mathematically expressed as: New Total Time = Old Total Time + (Extreme Time – Old Total Time)/K, where Extreme Time is 0 and 8 s for the key presses respectively aimed to decrease or increase the viewing time; the scaling constant K is set at 40. This equation entails decreased efficacy of each successive key press with respect to changing the viewing time. Such an exponential relationship between response and reinforcement rates is considered by some to be the superior strategy for the maintenance of operant behavior in both laboratory animals and in humans.
During the subsequent rating task, the subject rated the attractiveness of the same faces on a visual analog scale ranging from 0 “not attractive at all” to 100 “very attractive.” The value of using the keypress and the hedonic rating tasks is a more conclusive interpretation of the findings. A prior neuroimaging study employing the same pictorial stimuli in males indicated that the key presses, but not the attractiveness ratings, were paralleled by activation of distinct motivational and reward circuitry. Other lines of empirical laboratory-based evidence for the motivational value of beauty rather than social acceptance or desirability of prolonged viewing behavior towards opposite sexes is supported by stronger functional magnetic resonance imaging activations within motivational/reward regions by female than by male faces for heterosexual men and by male than by female faces for heterosexual women.
International affective pictures system stimuli
The IAPS was developed by the National Institute of Mental Health Center for Emotion and Attention, and a group of college students was retained to establish the standardized ratings for the pictures in the IAPS. We used a set of images from the IAPS, while employing the key press mechanics of the aforementioned facial experimental procedure. Based on normative ratings for affective valance (unpleasant to pleasant) and arousal (calm to excited), four categories of 50 IAPS images each were selected namely, “pleasant” (e.g., happy and erotic scenes), “aversive” (e.g., violent scenes) or “extremely aversive” (e.g., mutilated bodies) and “neutral” (e.g., common household objects). The “pleasant” images were selected from those with the highest normative arousal- and valence intensity scores. The “aversive” and “extremely aversive” images were with the highest normative arousal score and the respectively low and lowest normative valence scores. Neutral images were with the highest normative arousal score selected from pictures with the median valence scores. Subjects were given on option to opt out of viewing the “extremely aversive” images; they were exposed to “aversive” images in their stead. The images were organized in two blocks by valence, pleasant and aversive/extremely aversive. Within each block, pleasant or (extremely) aversive images were presented in a pseudorandom order intermingled with “neutral” images. Thus, in addition to measuring motivational effort via keypress activity, this task provides important data on contextual processing as neutral images are attributed different motivational value depending on the qualities of other images with which they are intermixed.
Monetary stimulus
As alluded above, the stimuli values are not absolute; they depend on several contextual factors, including prior expectations, level of uncertainty, quantitative information processing, decision making and judgment. Money, an easily quantifiable and ubiquitously recognized stimulus that can be incorporated into contextual judgment tasks, provides a meaningful framework for clinical research by integrating concepts from experimental psychology and economics. Accordingly, we employed a monetary task eliciting decision making under risk and uncertainty, emotional responses and counterfactual comparison triggered by alternative and unrealized payoffs underlying “what could have happened” types of contextual processing. The stimulus display comprised two disks, divided into blue- and yellow-colored sectors with areas corresponding to respective probabilities of receiving a monetary payoff or nothing (Fig. 1). By reading a set text, subjects were informed that they would participate in a game of chance and could earn money via a randomly selected winning bet at the conclusion of the task. It was further explained to the subjects that an arrow would spin around a spinner and come to rest in either of the two differentially colored sectors representing monetary gains or nothing. Subjects’ familiarity with the spinners was confirmed using a brief computerized quiz, completion of which was conditioned on the correct understanding of the task. The task was subdivided into two blocks either retaining the non-selected disk (to allow counterfactual comparison) or omitting it from the outcome phase of the same 30 trials presented in a pseudorandom order. The prompted counterfactual comparison between the obtained and the alternative (i.e., non-selected) outcome was reflected in a yes–no “Do you regret your choice?” question when appropriate. The trial sequence was identical for all subjects.
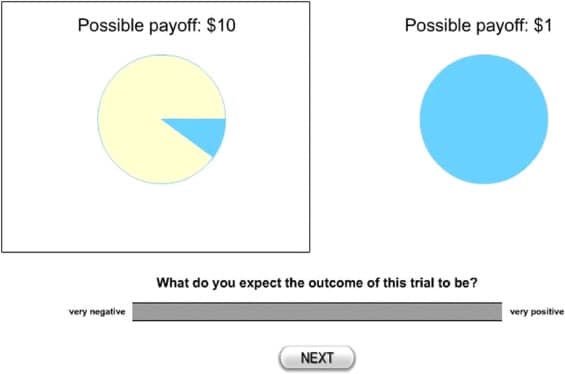
Using the computer mouse click, the subjects placed a bet on a more- or on a less risky option of an equal expected value (e.g., 10% for $10 or 100% for $1) within each pair followed by marking a point along a 100 mm visual analog scale (VAS) beneath the question: “What do you expect the outcome of this trial to be?” anchored “very negative” and “very positive” at the far left and right, respectively (Fig. 1). The question and the VAS scale then disappeared, and a spinning arrow was superimposed over the disk. The arrow's landing on one sector designated the monetary outcome of that trial. The subjects rated their satisfaction with the outcome on a 100 mm VAS scale by answering the question “How happy are you with the outcome?” that appeared below the spinner with the anchors of “not happy at all” and “very happy.”
Sweet tasting test
We used the STT, a validated by us single-blind procedure involving collection of subjective self-reports on hedonic value of a biochemical stimulus, sucrose (i.e., table sugar comprised of glucose and fructose) against the contextual backdrop of its sensory assessment. STT has an ecological validity in opioid addiction as sugar's hedonic properties are mediated by the opioidergic neurotransmission aimed at reinforcement of procurement behaviors of this indispensable energy source that is neither stored nor it is produced throughout the central nervous system.
Subjects were administered sucrose solutions at 0.05 M, 0.10 M, 0.21 M, 0.42 M and 0.83 М (for comparison: sucrose concentration in a 12 oz can of Coca Cola is 0.61 M) three times in for a total of 15 samples. The sequence of the sucrose concentrations was pseudorandom. Random shuffling the order of the stimuli helped to prevent adaptation and ensured that each stimulus was perceived as accurately as possible. This approach also helped to reduce the influence of potential order effects, where the order of presentation might have influenced subjects' ratings. The subjects were instructed to sip the solution, swish it around in their mouths, and spit it out, rinse their mouth with distilled water, make the rating and proceed to the next solution. They were then asked to rate “How sweet was the taste?” and “How much do you like the taste?” on a 100-mm analog scale anchored “not at all” and “very much” with 50 mm rating designated affective/hedonic neutrality.
Statistical analyses
Data were analyzed using the statistical package Statistica (StatSoft, Inc., Tulsa, OK). The statistical analyses of the experimental data first sought to determine the presence of differences between the entire dependent group (n = 60; consisted of subjects with opioid dependence and of those with alcohol dependence and dually diagnosed) and healthy subjects. The differences were analyzed by means of a nested analysis of variance (ANOVA) with Diagnosis (dependent and healthy) as a grouping factor and number of key presses or subjective ratings as a within-subjects factor (key presses and ratings were nested within subjects). The sweet taste ratings were analyzed with ANOVA with two between-subjects factors namely, Diagnosis (dependent and healthy) and Trial (first, second and third) and sucrose concentrations as within subjects’ factor. Analyses of covariance (ANCOVA) were performed for liking ratings entailing two within-subjects factors namely, Diagnosis and Trial. To control for the possibility that a difference in a liking rating merely reflected a difference of taste perception, this variable was employed as a covariate.
A significant Diagnosis by a within subject factor interaction prompted post-hoc Newman–Keuls t-tests to determine the level of the within subjects’ factor (e.g., type of images) that defined the group differences. Furthermore, such interaction justified additional nested ANOVAs performed separately with each dependent group, followed by post-hoc Newman–Keuls t-tests to determine if and which of the dependent subgroups was different from the healthy group and if and how the dependent groups were different among each other. Independent samples t-tests (or Fisher's exact tests as appropriate) were employed to analyze baseline demographic and clinical differences (Table 1). Group data were summarized as mean ± standard error of the mean (SEM). All analyses were two-tailed, and p < 0.05 defined statistical significance. Due to a scheduling error, facial key press- and STT data were respectively unavailable for one subject with alcohol dependence and for one control subject. These missing data were replaced by two subjects fulfilling the respective inclusion criteria.
Results
Clinical and demographic data
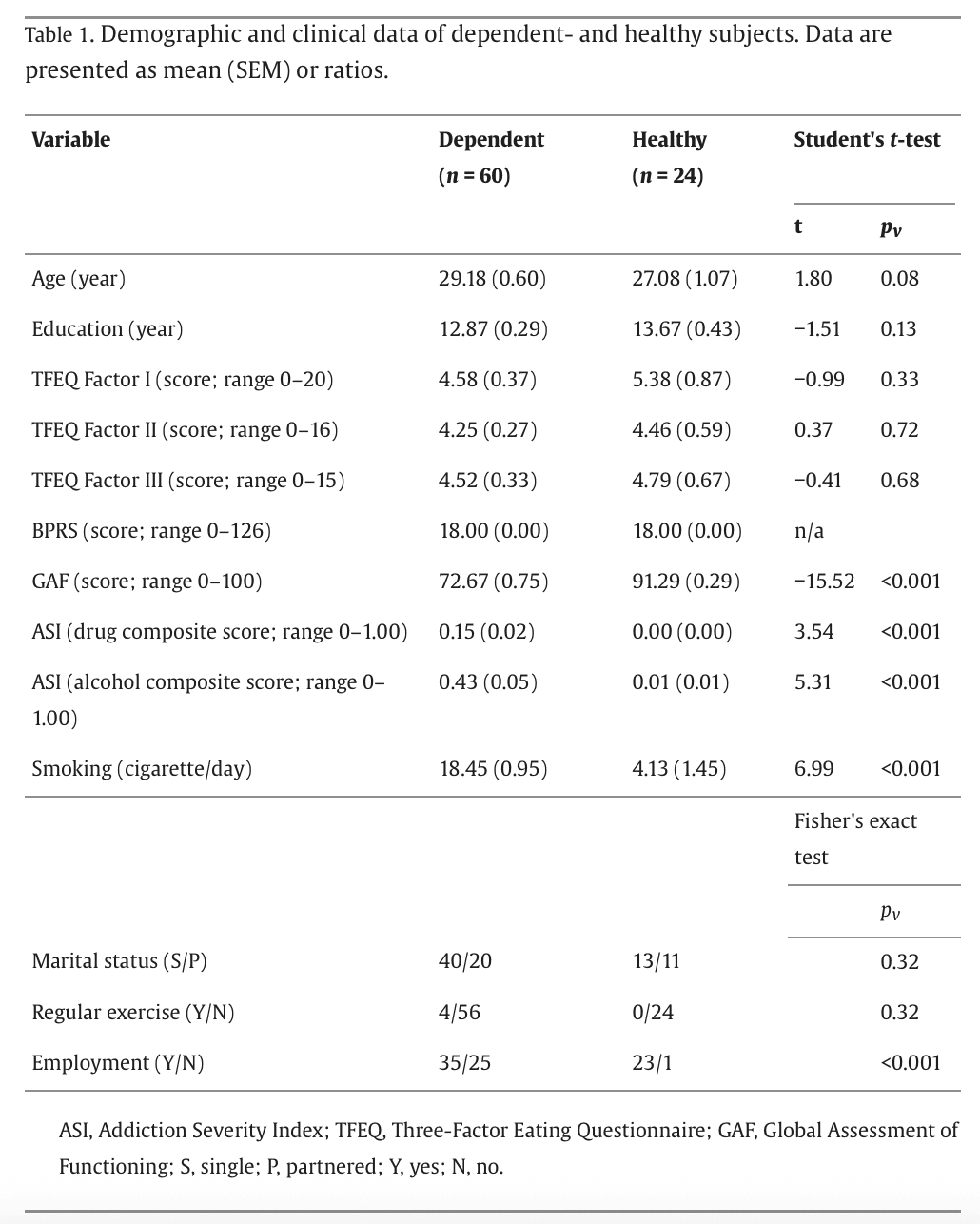
Dependent and healthy subjects were not significantly different with respect to age, race (all Caucasian), education, marital status, eating behavior, psychiatric symptoms, and physical exercise (Table 1). As planned, the ASI drug and alcohol composite scores were significantly higher in the dependent than in healthy subjects. Dependent subjects presented lower GAF scores with greater rates of smoking and unemployment.
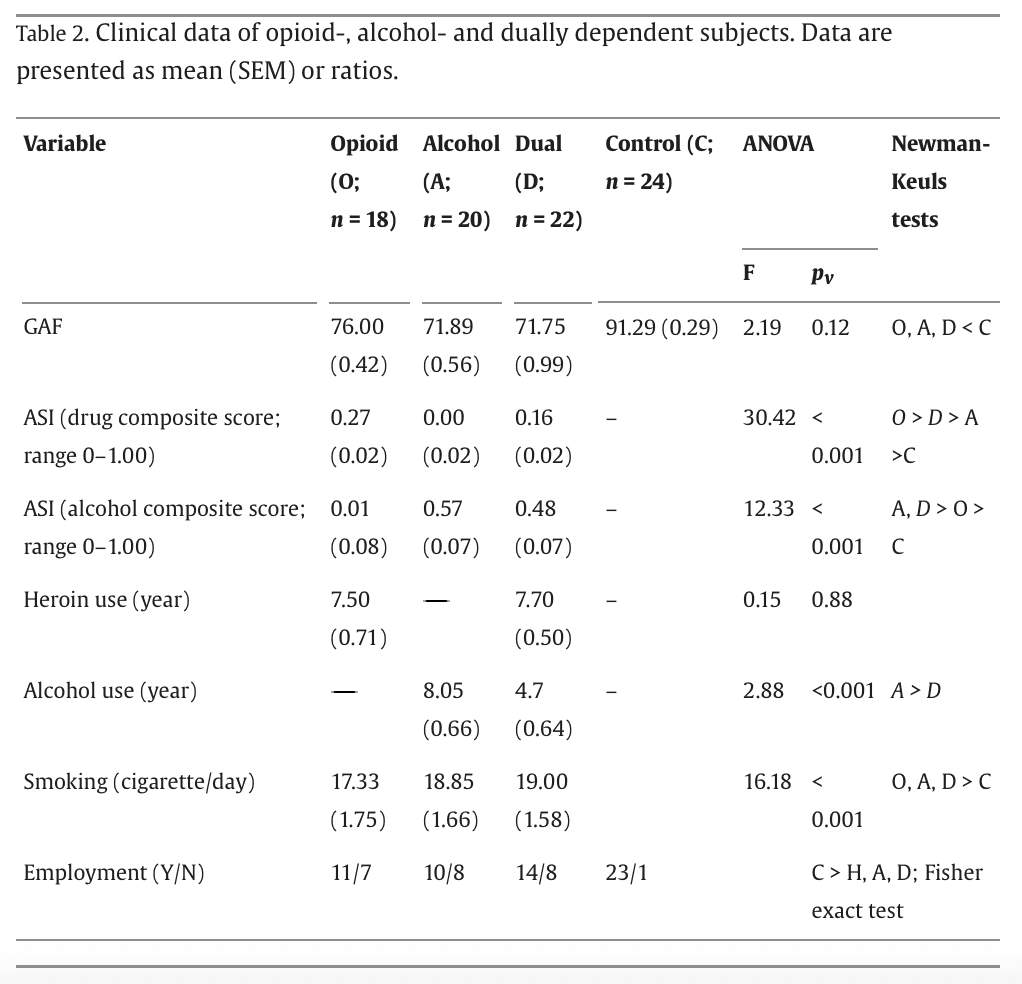
Table 2 presents the means for each study groups separately, along with results of the nested ANOVA and significant pairwise group differences. The dependent groups presented similar GAF scores, smoking and employment status. The duration of alcohol use was longer in alcohol dependent- than in dually diagnosed subjects due to the prior years of the sole heroin consumption in the latter group. Opioid dependent and dually diagnosed subjects used heroin for a similar period. The ASI drug and alcohol severity composite scores were respectively higher in opioid- and alcohol dependent- than in dually diagnosed subjects.
Procedural outcomes
Facial stimuli
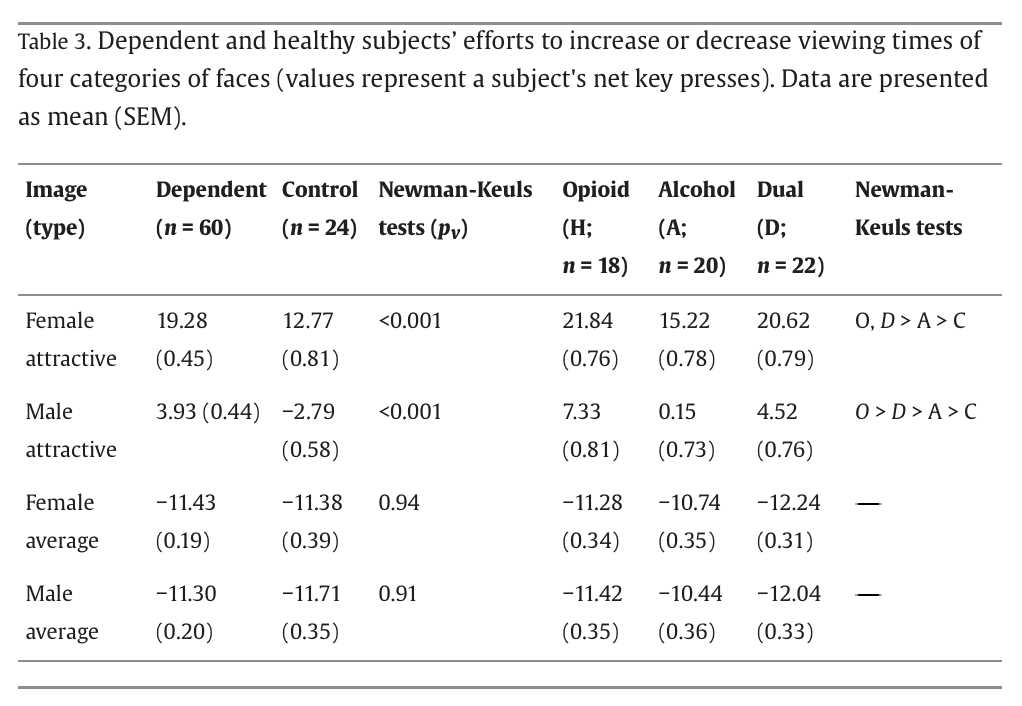
For the key press data, the nested ANOVA results yielded a significant group effect (F = 29.19, p < 0.001) and group by face type interaction (F = 20.17, p < 0.001), with post-hoc Newman–Keuls t tests showing a higher number of key presses in the dependent group for attractive female and male images (Table 3). The dependent subjects increased the viewing time of the attractive male images while the control subjects displayed an opposite directionality of their response. The group effect (F = 37.38, p < 0.001) and group by face type interaction (F = 17.80, p < 0.001) were also significant for additional nested ANOVAs performed separately with each dependent group. The key press numbers for attractive female and male were the highest in opioid dependent subjects followed by the dually diagnosed subjects (Table 3).
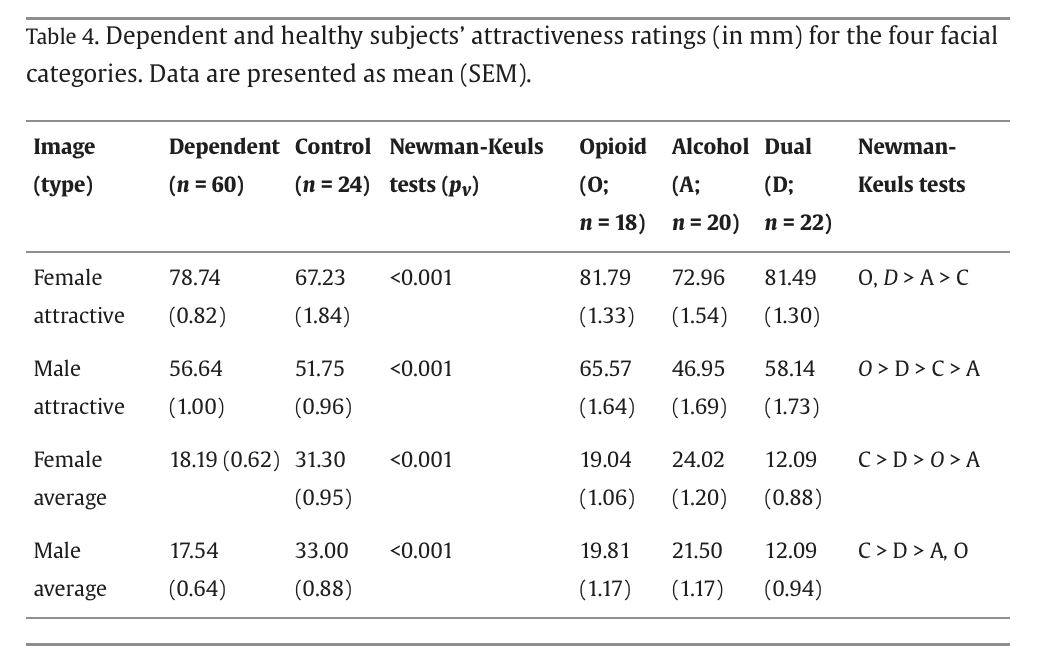
The dependent and healthy groups differed in the attractiveness ratings (group effect: F = 25.23, p < 0.001; group by face type interaction: F = 17.56, p < 0.001). Additional nested ANOVAs performed separately with each dependent group also resulted in significant group effect (F = 25.23, p < 0.001) and group by face type interaction (F = 17.56, p < 0.001). Dependent subjects rated significantly higher female and male attractive faces and significantly lower average female and male attractive faces (Table 4). These effects were respectively most pronounced in heroin dependent- and dually diagnosed subjects. The ratings of male attractiveness were, however, close to neutral in both dependent and control groups.
IAPS stimuli
A greater (p < 0.05; Fisher exact test) proportion of dependent (30.00%) - than healthy (8.33%) subjects opted out from viewing the extremely aversive images. The opioid (20.0%)-, alcohol (40.0%) - and dual (31.81%) groups were not significantly different (p > 0.16) among each other.
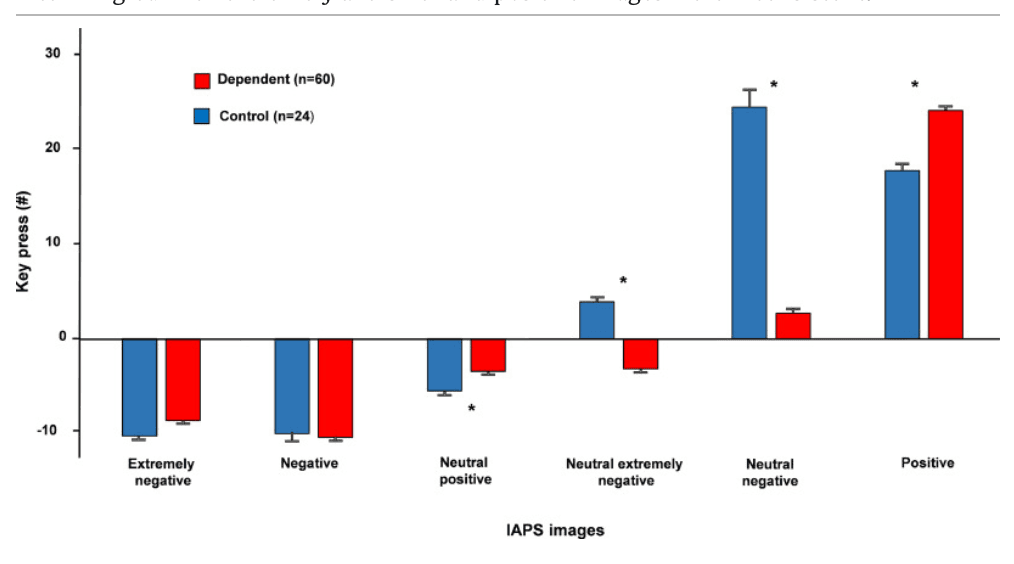
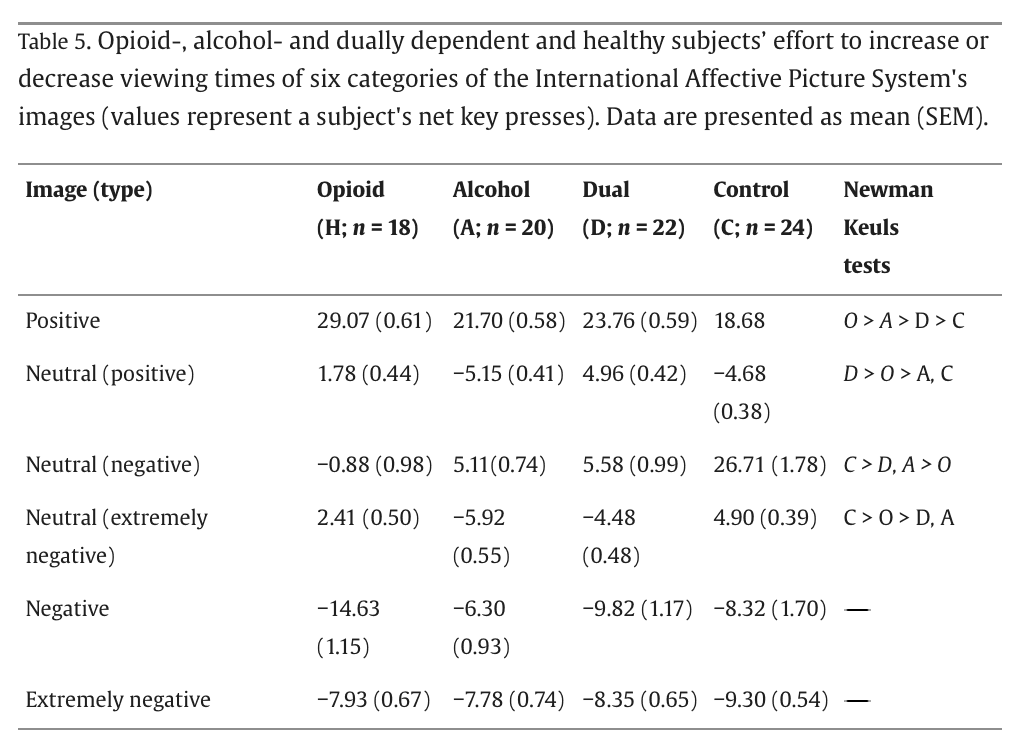
Between-group analyses of key-press data for pleasant-, aversive-, extremely aversive-, neutral intermingled with pleasant-, neutral intermingled with aversive- and neutral intermingled with extremely aversive images produced a significant group effect (F = 19.66, p < 0.001) and group by image type interaction (F = 21.22, p < 0.001). Post-hoc Newman–Keuls t tests showed a significant higher number of key presses for the pleasant images but not for aversive- or extremely aversive images in the dependent group. Moreover, dependent subjects made a significantly smaller effort to reduce the viewing of neutral images when viewed in the context of pleasant images or to increase the viewing of neutral images when viewed in the context of (extremely) aversive images (Fig. 2). Follow up ANOVA performed separately with each dependent group also resulted in significant group effect (F = 41.19, p < 0.001) and group by image type interaction (F = 51.57, p < 0.001). As presented in Table 5, opioid dependent subjects exerted the highest effort for positive images and the lowest effort for neutral images intermingled with stressful images. The differences among dependent group for neutral images intermingled with extremely aversive- and positive images were inconsistent.
Monetary stimuli
The dependent and control subjects displayed no significant group differences in the number of risky choices (Table 6). Parenthetically, the groups also did not differ in the rates of risk seekers (20% vs. 29%; p = 0.40, Fisher exact test) defined as over 50% risky choices on at least one of the two blocks (with- or without counterfactual comparison). The t-tests (independent samples) revealed significant differences between dependent and control groups in the mean number of the reported counterfactual regrets for both gains [1.88(0.29) and 0.44(0.39); t = 2.46; p = 0.02] and losses [3.43(0.45) and 1.41(0.76); t = 2.18; p = 0.03]. Follow up ANOVA performed separately with each dependent group did not reveal significant counterfactual regret differences among the dependent groups. Counterfactual comparison was used as a within-subjects factor (two levels: present vs. absent) in the subsequent monetary stimuli analyses (Table 6).
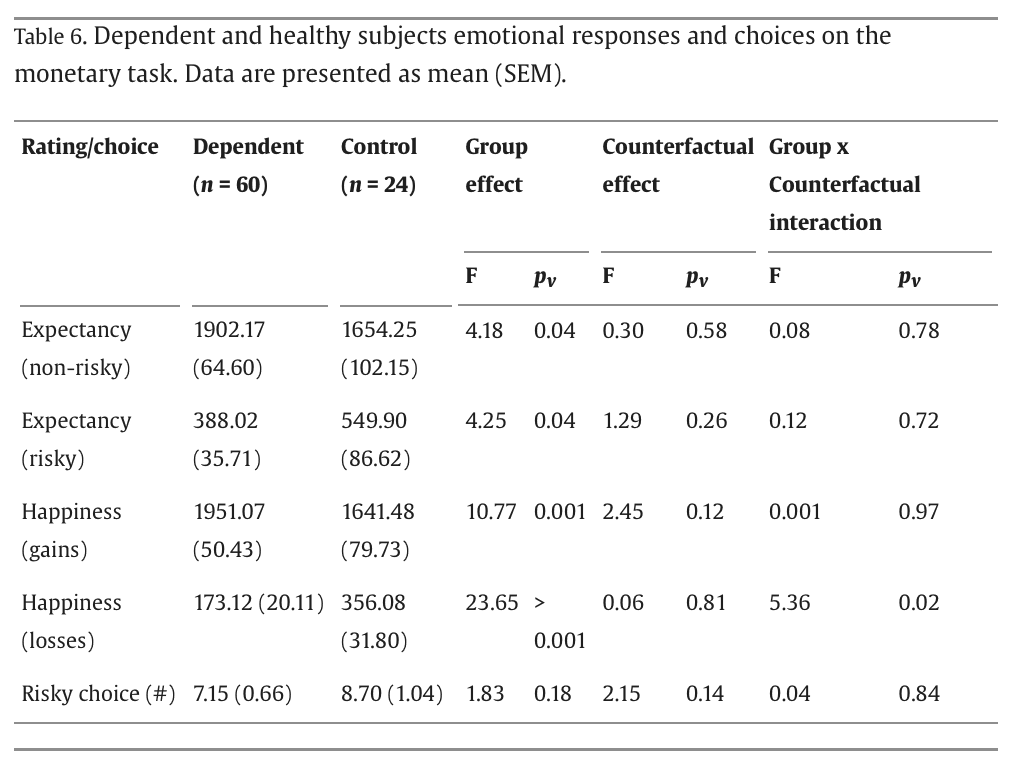
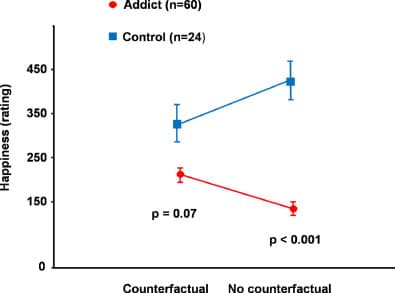
In comparison to healthy controls, dependent subjects reported lower expectancy for risky bets and higher expectancy for non-risky bets resulting in significant group effects, but no counterfactual effect or counterfactual by group interaction. In a similar fashion, respectively higher satisfaction with gains and lower satisfaction with losses by dependent subjects produced significant group effects. The group by counterfactual comparison interaction was significant for losses (F = 5.36; p = 0.02) when alternative outcome was gain but not for gains (F = 0.001; p = 0.97) when alternative outcome was loss (Fig. 3). Contextual processing impairment in the dependent subjects is thus evident in their failure to match the loss (dis)satisfaction response to “what could have happened” (i.e., gain) contextual comparison. The dependent groups did not differ significantly among each other regarding their expectancy and satisfaction ratings.
Sweet tasting test (STT)
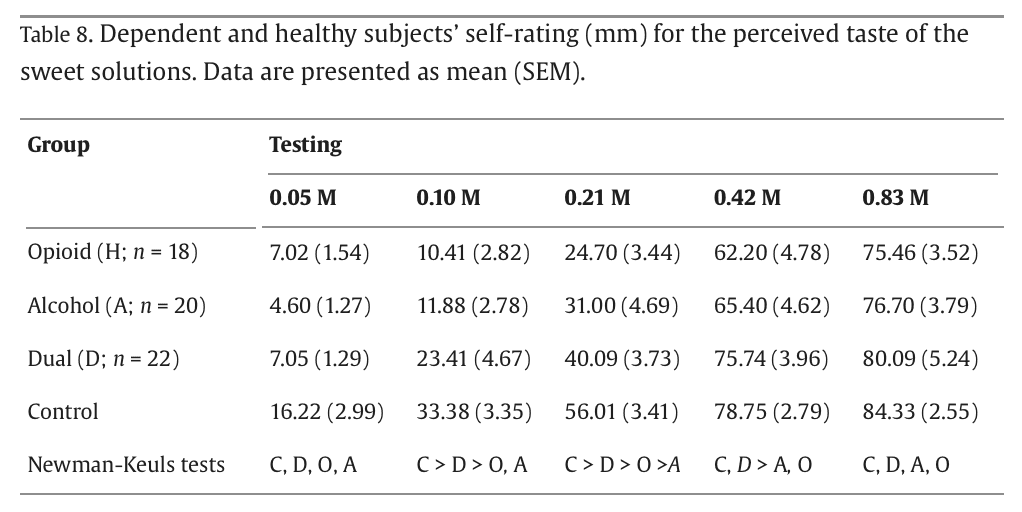
The hunger and thirst ratings were not different between dependent and healthy subjects before and after the STT (Table 7). Data analytic approaches to STT data analyses were recently reviewed. Sweetness rating increased monotonically (F = 579.82; p < 0.001) in both groups (i.e., concentration effect). All subjects gave highest sweetness ratings to high sucrose concentrations (0.42 M and 0.83М). The solutions were assessed to be less sweet by the dependent subjects (Fig. 4) resulting in a significant group effect (F = 59.83; p < 0.001) and a group by concentration interaction (F = 7.38; p < 0.001), but no significant effect of the trial (F = 0.006; p = 0.99). Post-hoc Newman–Keuls tests revealed that taste rating by dependent subjects were significantly lower for the 0.05 M (p = 0.001), 0.10 M (p < 0.001), 0.21 M (p < 0.001), 0.42 M (p < 0.001) and 0.83М (p < 0.05) sucrose concentrations (Fig. 4). Follow up ANOVAs performed separately with each dependent group also resulted in significant group effect (F = 27.95, p < 0.001) and group by concentration interaction (F = 3.98, p < 0.001). Dependent subjects rated significantly lower 0.10 M, 0.21 M and 0.42 M sucrose concentrations. This was particularly so for opioid- and alcohol dependent subjects (Table 8).
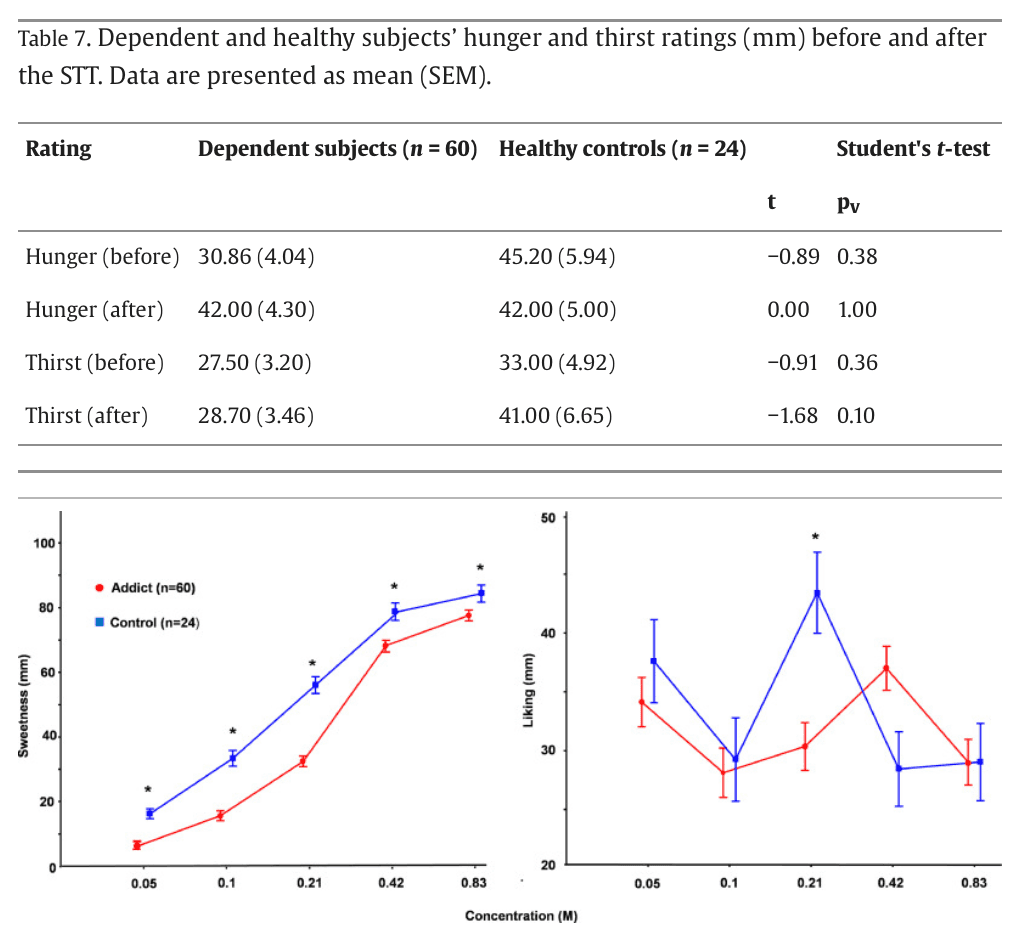
The subjects reported different liking (pleasantness) ratings across the rising sucrose concentrations i.e., concentration effect (F = 5.68; p < 0.001); the group by concentration interaction (F = 5.93; p < 0.001), but not group (F = 0.44; p = 0.51) or trial (F = 1.20; p = 0.30) effects were significant. Dependent subjects provided lower (p < 0.001) ratings than controls for the 0.21 M breakpoint, according to post-hoc Newman–Keuls tests; the liking ratings provided for other concentrations were not statistically different among the dependent and control subjects. Additional follow up ANCOVA covaring for the 0.21 M sweet taste rating yielded significant group effect (F = 6.78; p < 0.001) with controls providing higher ratings than subjects with dual diagnosis; the latter ratings were greater than those by the opioid- or alcohol dependent groups.
Contrary to the quantitative data above, a greater (p = 0.03; Fisher exact test) proportion of dependent (56.67%) than healthy (29.17%) subjects liked the high concentrations’ solutions, defined as the highest rating given to the 0.42 M or 0.83 M sucrose solutions. Pairwise comparison indicated that the above difference was driven by the alcohol dependent (75.0%) group; opioid (38.89%)-, and dually diagnosed (54.55%) groups were not significantly different from the controls.
Summary of results
Healthy subjects displayed consistent response pattern across all categories of the presented stimuli including: 1) heightened hedonic ratings for attractive faces and for 2) moderately sweet solutions; 3) heightened effort to extend the viewing time of the attractive faces and positive IAPS images and 4) to diminish the viewing time of the average- and attractive male faces and of aversive IAPS images; 5) reliable response patterns to neutral IAPS images presented in the context of pleasant vs. aversive images and 6) during the expectation of monetary outcome, its valuation and counterfactual comparison. The disproportionally low motivational drive to reduce the viewing of extremely aversive vs. aversive images by healthy controls as well as their greater effort to increase the viewing of neutral images in the context of aversive vs. extremely aversive images may be a normative state of decontextualization akin to the failure of graphic cigarette warnings to produce a greater (at times the effect is actually smaller) motivational effect as compared to plain text messages.
Nonetheless, the decontextualization phenomena were more pronounced in dependent subjects manifested in a mismatch between contextual background and the ensuing behavioral, cognitive, and emotional responses. Specifically, dependent subjects rated average faces as less attractive than healthy controls but failed to adjust their effort to decrease the viewing times of these same faces. Also, dependent subjects opted out more of viewing extremely aversive IAPS images while displaying similar motivational effort to decrease aversive and extremely aversive images’ viewing time. Furthermore, dependent subjects failed to modify the types of choices (non-risky vs. risky) despite the growing number of self-reported dissatisfaction and regret ratings; their hedonic rating of 0.21 M sucrose solution was mismatched with the perception of the solution's sweetness.
Discussion
To our knowledge, this is the first demonstration of contextual deficits in opioid and alcohol dependence using four distinct yet complementary stimuli of positive, negative, and neutral valence. The possibility that the dependent subjects’ failure to recognize context represents a general perceptual decrement, rather than a specific contextual processing deficit, is disputed by consistent and adequate valuational assessments of the presented stimuli (e.g., faces, emotional images, and monetary outcomes). As such our data define a novel perspective on emotional and behavioral changes in opioid and alcohol dependence. We discuss the findings of positive stimuli overvaluation and negative stimuli desensitization to put forward a model of free will with contextual processing as a potential driver of addictive behavior.
Positive stimuli: heightened hedonic and motivational valuation
Heightened viewing time of the attractive females by heterosexual male dependent subjects in comparison to heterosexual healthy males demonstrated a motivational effort that matched the subjectively rated value of the presented stimuli. The dependent subjects also extended the viewing time of attractive male faces, that are perceived as aversive by healthy heterosexual males. This suggests that the motivational strength of positively valenced stimuli in dependent subjects may override other contextual deterrents that could arise from such sources as feelings of intimidation, threat, or jealousy, particularly if the displayed individuals are perceived as potential romantic or sexual rivals.
The attractive females and positive IAPS images’ key press data as well as the monetary gains ratings and the proportion of sugar likers are reminiscent of the positive reinforcement mechanisms inherent in addictive disorders, that is to say, pursuit of instantaneous reward such as subjective pleasure or “high” produced by addictive substances even though the overall strategy aimed at procurement of these substances is rendered disadvantageous by the disregard of the health and social contextual factors. In this study, we captured an independent aspect of the positive reinforcement mechanisms triggered by positive stimuli at large not by the addictive substance per se or by the conditioned cues.
The extant clinical and functional neuroimaging data pertaining to positive stimuli responsivity in opioid use disorder are far from consistent and the theoretical considerations are not unambiguous. Recurrent dopaminergictrafficking consequent to opioids or other euphorigenic drugs consumption may eventually result in hypodopaminergic state, clinically noticeable as diminution of drives and of capacity to experience pleasure, mediated by accumulation of the transcription factor, CREB, in the reward and motivational circuits. This notion is echoed by reports on reduced reward function in patients with opioid and alcohol use disorders.
The present and prior empirical findings have not fully supported the above conjecture. In fact, a substantial body of preclinical and clinical research suggests that reward deficiency (if present) is time limited and cannot explain the long-term relapse vulnerability. Accordingly, in rodent models, termination of chronic non-contingent drug exposure results in only a few day-long decreases in basal dopamine transmission or elevation of the brain reward stimulation thresholds. On the other hand, following an extended access to drugs, rodents display stronger preference for social rewards and palatable food e.g., sugar. Likewise, many addicts display preference for sweet food and for smaller yet instantaneous rewards over the delayed ones potentially explaining their favorable response to alternative reinforcement regiments by means of contingency management and community reinforcement. Thus, opioid use may paradoxically produce a seemingly advantageous clinical action in individuals with reward deficits by sensitizing previously non- or under-responsive reward circuitry not only to opioids, but via cross-sensitization processes to natural rewards. The latter is consistent with delay discounting and impulsivity associated with elevated reward-induced dopamine surges.
Negative stimuli: incentive desensitization
Dependent subjects rated average faces as less attractive than healthy controls but expended similar effort to decrease the viewing times of these same faces. Also, dependent subjects opted out more of viewing extremely aversive IAPS images while displaying similar to controls’ motivational effort to decrease extremely aversive and aversive images’ viewing time. The inefficiency of negative reinforcers (negative IAPS and monetary losses) in modulating behavior and choices (i.e., insensitive desensitization to aversive stimuli) is strengthened since it is consistent with prior addiction neuroimaging data on diminished brain activations to non-drug-related aversive stimuli.
While it is commonly theorized that addiction develops via negative reinforcement mechanisms (i.e., a substance is used to ameliorate the unpleasantness of withdrawal and/or of negative affective states arising in the context of social/professional setbacks) our findings support the adaptation of this idea in the form of a positive reinforcement hypothesis that continued substance abuse amplifies hedonic and motivational value of rewarding stimuli. Such hedonic experiences, although overshadowed by the ongoing withdrawal may become conspicuous after full detoxification. Taken together, our findings have implications for clinical addiction medicine by helping to explicate the reasons underlying repeated failures of health- and social deterrents to curb addictive behaviors despite negative consequences.
Implications for the role of free will in addiction
In contrast to other species, humans are not solely driven by instincts and survival considerations but are also endowed with free will allowing them to weigh their choices and consequent actions against the contextual backdrop created by the values attributed to goal-objects. How the decisions and consequent choices are made is a subject of competing theories. Some emphasize physiological needs, the fulfillment of which is prioritized even in the face of scruples and negative consequences. For instance, unrelenting hunger could drive a theft of a bread loaf notwithstanding the looming aversive outcome of imprisonment. Others prioritize personal emotional satisfaction or do quite the opposite by adhering the ethical or religious principles. Once more, a writer and philosopher, Herman Hesse reckoned that: “essentially, people express freedom only in their choice of dependency.”
Addiction is defined by continuous consumption of addictive substances while disregarding the knowledge and experience of their hazardous effects. Some addiction models postulate that patients are conditioned and so driven to seek and consume addictive substances as a result of the usurped brain circuits involved in the exertion of free will. Then again, it has been suggested that outside the realm of addictive substances “most people whom we would consider suffering from addiction remain able to choose advantageously.” The present study offers a view that integrates the above perspectives. Rather than been a unitary state characterized by one set of motivations and emotions free will seems to be modulated by the goal-objects’ valence countenancing freedom to choose among positively reinforcing goal-objects. In contrast, neutral or aversive stimuli findings in the dependent groups signified dissociated motivational and valuational choice components obviating the ability to exercise a free will. The reasons behind dependent subjects’ pattern in giving up the riddance of the negative stimuli while avidly perusing positive stimuli is yet unknown. Subjects may perceive positive stimuli as a more salient and thus more available target in part due to unconscious psychological mechanisms e.g., suppression and denial or due to discussed below dissociated connectivity between the respective brain centers entrusted with valuational and motivational functions.
Contextual processing and addiction
The ballet “Petrushka” by Stravinsky and Benois culminates in a poignant scene of the protagonist's slaying by a romantic rival. The viewer is then left with a lingering doubt of whether to revel in an enchanting amalgamation of music, dance, and colorful décor, to bemoan the demise of an affable and vivacious character or to dismiss the entire occurrence as a flamboyant farce involving dancing puppets, albeit performed by real life people. Addicts may be unable to perceive and cherish the subtitles evoked by alternating contextual backgrounds. Probably the most important is the ‘tug of war’ between the addictive substances’ consumption and the resultant adverse consequences context.
Dissociation between contextual processing and stimuli responsivity in a combined group of dependent subjects is in accord with an earlier study showing that cocaine addiction was associated with contextual processing impairments. Furthermore, our findings extend to the socially-, valuation judgement- and sensory-framed context this prior report on the context set by a variant of the continuous performance test. Although there were methodological similarities between the latter and the current study (e.g., enrollment of addicted subjects and measures of contextual processing), there were also important differences, including samples of opioid-, alcohol- and dually dependent subjects and the use of the multimodal tasks devoid of coordination and motor sequencing components but focused on valuation, motivation, decisions-weighing and on behaviors aimed at reward seeking or avoidance of punishment. Thus, this independent replication supports the validity of the relationship between contextual processing and addiction.
It has been noted that neuropsychiatric disorders with excessive endogenous opioid function e.g., post-traumatic stress disorder, autism spectrum disorders and schizophrenia associated with decontextualization i.e., decoupling of the stimulus from its natural context. Moreover, psychotic symptoms in schizophrenic patients could originate from sporadic or stress-induced dopamine spikes causing loosening of perceptual context via improper context conditioning and/or attribution of aberrant significance to random events. Given the contextual abnormalities arising in patients exposed to endogenous opiate and dopamine outpourings in the limbic system, a compelling a fortiori argument could be that propensity for decontextualization is worsened by the neuropsychopathology associated with erratic supraphysiological opioidergic and dopaminergic bombardment of the limbic system by exogenously administered opioids, alcohol, or other addictive substances.
A rich set of emotional, motivational, and cognitive factors are applicable for charting the course of addictive disorders, in weighing the prospects of addiction relapse or deterioration, and in evaluating the outcomes of ongoing therapy. Among them is the extensive contextual processing system with emotional and cognitive constituents that determines whether an individual ascertains control over desires and temptations with potential adverse consequences. Such desires and temptations may attain control over an individual with impairments in the contextual system manifested in rigid motivational states fixated on idiosyncratic and irrelevant stimuli with diminution of neuronal adaptability and modulation by changing context and salience.
Moreover, in the aforesaid and other psychopathological conditions the brain circuits that are directly responsible for cognitive aspects of contextual processing may function independently from the subcortical limbic input. Such disintegration between contextual processing and stimulus-driven actions and emotions may occur due to (a) substantial dopaminergic surges in reward, motivation, and learning centers leading to “hardwired” neuroplasticity in the striato-thalamic frontal cortical loop, with ensuing top-down dissociation from the subcortical activity; and/or (b) hypofunctionality of the excitatory glutamatergic afferents from the amygdala–hippocampus complex failing to produce bottom-up restrain of the striato-thalamic-frontal cortical loops. For instance, positive symptoms of schizophrenia may become dissociated from the mesolimbic subcortical activity and persist despite complete dopamine blockade by antipsychotic agents. Moreover, craving in patients addicted to opioids induced by contextual cues persists even in the face of presumptively fully occupied opioid receptors in the subcortical limbic areas. This is also the case for cocaine craving in cocaine dependent subjects receiving agonist substitution therapy.
Lack of consistent differences among the groups of dependent subjects
While tremendous progress of basic addiction research has shed light on the key cellular and molecular mechanisms, we still yearn for the discovery of coherent laws that will unite the prevailing models of addictive substances to generate new leads for the development of therapeutic interventions. The mesolimbic dopaminergic pathways are conventionally considered to be the key component of the brain reward and reinforcement system involved in positive subjective responses to both natural rewards and to drugs of abuse. However, conclusion from comprehensive reviews is that the published empirical data from rodent and non-human primate models, and human imaging studies do not fully support a critical role of mesolimbic dopamine even within the same group of addictive substances such as central nervous system depressants like opioids and alcohol. It is therefore useful to divide the multidimensional addiction process into domains based on the underlying system (e.g., the Research Domain Criteria).
The present project enabled identification of opioid and alcohol addictions’ common aspects in terms of contextual processing thus providing a sounder footing for understanding potential interaction between context- with reward- and aversion systems and their role in the generalized circuitry of addiction. Given the challenges inherent in direct comparison of responses to opioid paraphernalia (e.g., needles, syringes, pill bottles, places associated with drug use, or the sight, smell, or taste of the drug itself) and alcohol-related stimuli (e.g., images of people drinking, the smell of alcohol, the sight of a bar or liquor store, or the sound of glasses clinking) it may be valuable to explore whether opioid and/or alcohol exposure have similar effects on the contextual cues responsivity. This could be achieved by identifying the levels of severity in opioid and alcohol use that are linked to comparable degrees of changes during exposure to the above types of stimuli.
Additionally, this study only assessed the interaction of active alcohol dependence with opioid dependence in remission. Future work needs to address the nature of the active opioid-alcohol interactions e.g., competitive, additive, or synergistic. Acutely, the latter two may be the most notable ones as over 50% of overdoses are associated with concurrent opioid and alcohol use. What is more, an in-vitro protozoan motility study showed additive opioid and alcohol effect on the on the membrane stability. Elucidation the shared contextual processing foundation for opioid and alcohol addiction could have important implications. The reinforcing effects of opioids are among those that sensitize over time. If the neural circuitry underlying sensitization plays a role in alcohol consumption, then cross-sensitization might occur as well. If so, exposure to opioids could increase vulnerability to the development of alcohol addiction and vice-versa. After a long period of abstinence, delivery of a priming dose of an addictive drug can re-establish drug self-administration in laboratory animals; this effect is elicited even when the stimulus used for priming is drawn from a different class than the initially administered substance and may even include the positive goal-objects addressed here e.g., sex or sugar. The present data call for further research aimed at understanding the distinctive features of opioids vis-à-vis those of alcohol and comorbid alcohol + opioids and their effects in the unique and shared contextual processing effects.
Caveats
Caveats that should be considered in interpreting our data refer to the type of employed stimuli, design, and participants. The stimuli are qualitatively different from the factors implicated in the pathophysiology of addictive disorders. However, we believe that our results have clinical significance because real life opioid and alcohol consumption affects similar brain areas to those perturbed by the “mating opportunity mindset”-inducing faces, IAPS images, monetary gains and losses and sweet solutions.
At least two possible origins exist for the altered processing of pleasant and aversive stimuli in opioid and/or alcohol dependence. First, chronic administration of opioids and alcohol affects responses at a cellular and molecular level producing long-term changes in the brain structure/function and may alter underlying mechanisms of adaptation. Considering this, it is tempting to surmise that the origin of the contextual processing dysfunction found in this study is damage to the brain induced by the respective substances. It is also possible that a preexisting genetic or acquired risk factor e.g., novelty/thrill seeking, which is manifest in contextual processing is imparting vulnerability for excessive opioid and alcohol consumption. However, before the origin of the aforesaid impairments is to be investigated via prospective and/or twin studies, it is first necessary to show that it exists. The latter, and not the former, was the objective of our project. Also, the way the study was designed does not enable us to make a definite conclusion that the observed contextual processing alterations were the primary feature of addiction or were secondary to the long-term effects of the addictive drugs. To answer this question accurately, we would need to separate the addiction component by studying a behavioral addiction, such as gambling, that does not involve any drug or alcohol usage.
Even though this study relied solely on behavioral and self-report measures and no structural and functional brain data were obtained, our findings provide a foundation for further, more comprehensively designed, brain imaging projects. Such projects may include examination of the potential relationship between brain activations and both objective and subjective outcomes of the study procedures e.g., keypresses and ratings of monetary expectancy/outcome and of sweet solutions. Additionally, while possible withdrawal confounds were reasonably controlled through the employed therapeutic protocol fully addressing this issue would require subjects’ assessment at various stages of the withdrawal and remission course.
There are noteworthy changes from DSM-IV TR to DSM 5 TR addiction diagnostic criteria including, but not limited to the expansion of the type of incorporated symptomatology, elimination of legal problems and to the deletion of a seemingly important abuse and dependence distinction. Consequently, in comparison to DSM-5 TR, DSM-IV TR dependence criteria yield a greater diagnostic sensitivity viz., fewer false negatives’ rates. This raises the possibility of a difference in the present study outcomes using the newer nosology and underscores the importance of the ongoing quest for more refined diagnostic tools particularly in the areas of the impaired control, risky use, social impairment and pharmacological indicators symptoms clusters of addictive disorders.
The subjects’ sample was limited to male participants. Women suffer greater detriment from the opioid addiction then men with steadily growing overdose rates. Furthermore, in comparison to men, women experience substantially greater morbidity from excessive alcohol intake. Alterations in neurohormonal state through the menstrual cycle create potential problems of reproducibility and interpretation of data. For example, menstrual cycle phase may affect women's facial preference; in follicular phase, in comparison to other phases, women are more attentive to stereotypically masculine faces. Therefore the keypress and IAPS data are not generalizable to women. Moreover, brain responses during expectancy and outcome phases of monetary stimuli processing have been found to differ from those of men as a function of menstrual phase, though only in amplitude, not in location. The current sweet taste findings may not also generalize to females’ samples, which exhibit different patterns of glucoregulatory function. In sum, to formulate a viable model for contextual processing in opioid and alcohol addiction, a gender factor should be an important consideration for sequential research projects. This can be achieved by scheduling women for admission in a consistent phase of the menstrual cycle as well as matching and stratifying the study groups by gender.
Conclusions
The present findings suggest that dissection of contextual processing function can be pursued with the goal of understanding the processes generating motivated behavior in health and in addictive disorders. Hitherto, in the addiction literature “context” has been mostly addressed as a factor in a conditioned relapse to substance abuse after a period of abstinence. Our observations extend the prior findings by suggesting that the relationship is not specific to the cues defined by the substances and rather generalizes to other forms of contextual processing be it facial and affective images, money or sweet solutions. The congruence of our data with the results from other research applying the same type of stimuli lend further credence to the suggestion of addiction-driven positive reinforcement operation enabling the exercise of the free will while switching the pursuit of various positive goal-objects for maximizing short-term subjectively pleasurable experiences. At the same time, addicts are only hedonically-, but not motivationally sensitized to negative reinforcement leading to free will impairments in the domain of negative goal-objects. Therefore, contextual processing alterations may evolve as a credible target of both, pharmacological and non-pharmacological interventions emphasizing proper decision-making algorithms and promoting rational choices and behaviors along with prizes for abstinence instead of punishments for lack thereof. The efficacy of such strategies could be monitored via symptomatic improvement and its correlation with the procedures introduced by this project. Ultimately, the value of the contextual processing model will depend upon its ability to account for specific clinical and neurobiological aspects of addictive disorders and the degree to which novel therapeutic strategies based upon this model prove to be therapeutically advantageous.