Abstract
Research indicates young individuals with traumatic brain injuries (TBI) in juvenile justice settings lack essential support, mainly due to staff members' insufficient knowledge and skills in TBI-related areas stemming from a lack of relevant professional development. This study aimed to improve services for justiceinvolved youths with TBI in juvenile correction facilities by establishing empirically validated core competencies tailored to their needs. Through a Delphi study involving experts in juvenile services, juvenile corrections, TBI, transition services, and professional development, we identified and refined a set of 44 competencies distributed across six domains: knowledge (12 competencies), screening (6 competencies), eligibility (3 competencies), assessment (4 competencies), intervention (10 competencies), and community reentry (9 competencies).
INTRODUCTION
Training of staff in the management of traumatic brain injuries (TBI) within juvenile correction facilities holds a pivotal role in safeguarding the welfare, rehabilitation, and safety of incarcerated young individuals grappling with TBI. TBI is a neurological injury that occurs when an external force causes damage to the brain. TBIs can result from various incidents, including accidents, falls, sports injuries, physical assaults, or any other event where the head sustains a blow, jolt, or penetrating injury. These injuries can range from mild (commonly referred to as concussions) to severe, and they can have a wide range of physical, cognitive, emotional, and behavioral effects on the individual (Centers for Disease Control, 2023).
Extensive research has highlighted the heightened vulnerability of justice involved youth to TBI, primarily attributed to the impulsive and risky behaviors frequently exhibited within this demographic (Browne et al., 2018). Additionally, TBI can amplify preexisting behavioral issues, impair cognitive development, and elevate the risk of repeat offenses (Arciniegas et al., 2015). Astonishingly, rates of brain injuries among incarcerated youth range from 12% to 82%, significantly surpassing those in the general population (Hughes et al., 2015; McKinley & Albicini, 2016; Nagele et al., 2021). TBI has also been associated with heightened aggression and behavioral dysfunctions, which introduce distinctive learning and behavioral traits that likely contribute to the disproportionately high incarceration rates among youth with TBI (Ryan et al., 2015). Many of these individuals tend to engage in risky behaviors and struggle to control their emotions, factors that can lead to delinquent behavior (Ganesalingam et al., 2006).
Moreover, youth with TBI often encounter communication challenges that hinder their effective participation in legal proceedings (Thompson et al., 1994; Wszalek & Turkstra, 2015). Their cognitive struggles can result in aggressive behavior and criminal acts (Max et al., 2005a). Alarmingly, young adults with TBI are four times more likely than their non-disabled peers to develop concurrent mental disorders associated with offending (Orlovska et al., 2014). Post-release, community reentry outcomes for previously incarcerated youth with TBI significantly lag behind those of their non-disabled counterparts (Bullis et al., 2004). These youth exhibit higher conviction rates and a greater likelihood of reoffending (Ray & Richardson, 2017). Cognitive deficits, particularly in executive functioning, learning, and attention, contribute to poor academic performance, school dropout, and impaired decisionmaking—three prominent risk factors for delinquent behavior (McCord, 1992; Wolfgang et al., 1987). The adverse repercussions of TBI consistently manifest in various domains, including general cognitive performance (Slater & Kohr, 1989), deterioration in language function (McInnes et al., 2017; Rowley et al., 2017; Wszalek & Turkstra, 2015), memory and attention deficits (Loken et al., 1995; Max et al., 2004; Max et al., 2005a; Max et al., 2005b), reduced processing speed (Mathias & Wheaton, 2007), compromised executive function (Rode et al., 2014), and impaired visual-motor skills (Thompson et al., 1994).
Given these multifaceted challenges faced by incarcerated youth with TBI, staff within juvenile correction facilities must be equipped with the knowledge and skills required to identify, assess, and address TBI-related issues effectively. On any given day, over 60,000 youth are incarcerated and cared for by a diverse array of staff in juvenile facilities (Gagnon et al., 2012). These professionals encompass therapists, counselors, corrections staff, correctional education personnel, and healthcare providers. Adequate staff training serves as a crucial instrument for early TBI detection, resulting in timely interventions that improve outcomes for affected youths. Through proper training, staff can discern the subtle signs and symptoms of TBI, including cognitive impairments, emotional dysregulation, and hindered social skills, often masked by disruptive behaviors (Bigler et al., 2013). This recognition paves the way for appropriate referrals for medical assessment and rehabilitation services, ensuring justice involved youth receive the essential care they require.
Pre-service and In-service Training
Unfortunately, existing research paints a concerning picture, indicating that youth with TBI in juvenile correction settings often do not receive the requisite support for positive outcomes (Williams & Chitsabesan, 2016). Surveys of correctional staff have revealed that fewer than two-thirds had received any training concerning students with disabilities in general (Kvarfordt et al., 2005). Many staff members in juvenile settings did not receive pre-service training and had limited relevant inservice professional development related to youth with disabilities (Hughes et al., 2015). Furthermore, research suggests that most correctional staff receive minimal professional development specifically tailored to youth with TBI (Gagnon et al., 2013; Mathur et al., 2009; Platt et al., 2015). The current training programs within the juvenile correction system often fall short in addressing common challenges associated with TBI (e.g., empathy, selfmonitoring of behavior) and how to support youth development of skills for successful reintegration and employment (Ray & Richardson, 2017). As a result of this training deficit, many staff members in juvenile settings lack the knowledge and skills needed to effectively address the impacts of TBI and support positive outcomes for youth with TBI (Ernst et al., 2016; Ettel et al., 2016; Graff & Caperell, 2016; Jordan & Linden, 2013).
Given these pressing challenges, there exists a critical imperative to provide counselors, residential staff, educators, administrators, and other support staff with professional development rooted in evidence-based practices to enhance the prospects of positive community integration, health, and employment outcomes for youth with TBI (Hughes et al., 2015; Ryan et al., 2015). Staff trained to employ evidence-based strategies for addressing the behavioral and cognitive issues of young individuals in juvenile correctional settings are pivotal for robust re-entry planning and the future success of these youth (Kvarfordt et al., 2005). Emerging evidence suggests high-quality staff training forms the foundation of interventions associated with improved outcomes for adults with TBI within justice settings (O'Rourke et al., 2016).
Professional Training Competencies
Professional training competencies reflect a desired performance level against which a professional’s performance can be compared. The main purpose of competencies is to develop a thorough understanding of the types of skills and knowledge that various personnel need to perform their jobs. Although professional competencies have been identified specifically for correctional facilities (i.e., Correctional Education Association Standards Commission, 2019), they do not include working with justice involved youth with TBI. For example, the Correctional Education Association Standards Commission recommends that correctional staff receive a total of 40 hours of in-service training on: (a) personnel and education department policies and procedures; (b) alternative, neglected, and delinquent education; (c) basic security training; (d) emergency plans, procedures, and responsibilities; (e) teaching the juvenile justice student; (f) behavior modification; (g) crisis intervention, and (h) learning disabilities (p7). Although these competencies include topics that might be relevant to youth with TBI (e.g., behavior modification, learning disabilities), they do not specifically address the unique needs of youth with TBI (e.g., deficits in executive functioning, communication skills, memory and attention, processing speeds). There is a critical need to identify TBI-specific competencies that could guide specific professional development to improve the knowledge and expertise of corrections professionals and drive programmatic changes for the youth with some of the poorest outcomes.
Recognizing the need to develop professional competencies that support incarcerated youth with TBI, we conducted a Delphi study to collate and refine expert opinions, pinpointing core competencies across various correctional personnel roles. Our primary research inquiry was: What competencies are necessary in staff training to ensure justiceinvolved youth with TBI receive evidence-based services aimed at improving their re-entry and life outcomes?
METHODS
Design
A Delphi approach was utilized to establish agreement on the core training competencies needed to ensure justice-involved youth with TBI receive evidence-based services to improve their re-entry. The Delphi method, a type of nominal group technique, was employed to gather input from experts and achieve consensus within a group regarding personnel competencies needed for supporting youth with TBI in juvenile correction facilities. Consensus was attained through an iterative process that involved experts responding to a series of questionnaires and receiving information in return. The Delphi method offered a structured and systematic approach to data collection, particularly when anecdotal or subjective information was the only available alternative (Linstone & Turoff, 2002). The strengths of the Delphi method included providing a structured communication method for knowledgeable individuals to express diverse perspectives, ongoing feedback, and the ability to revise previous contributions throughout the process, while ensuring the anonymity of expert panel members (Ludwig, 1994; Hsu & Sandford, 2007).
Participants
Given our focus on developing evidence-based staff training competencies, the primary population for this study was juvenile corrections staff. The authors developed a set of inclusion criteria to identify experts in the field of juvenile corrections and TBI. Experts were selected based on their knowledge, expertise, and experience relevant to the study topic. They were identified through our project advisory committee, literature review, recommendations from professionals, and professional associations. For the purpose of this study, an individual was deemed an expert if they met one or more of the following inclusion criteria:
Author/researcher of scholarly, peer-reviewed work relative to brain injury, brain injury and professional development, and/or brain injury and juvenile justice (JJ).
Practitioner (e.g., teacher, service provider [behavioral health, physical health, residential, vocational], correctional administrator, line staff, parole probation staff) with a minimum of two years of service in juvenile correctional facilities.
Practitioner (e.g., teacher, service provider [behavioral health, physical health, residential, vocational], juvenile justice administrator, line staff, parole probation staff) with a minimum of two years of service with youth with TBI.
The authors initially generated a list of 35 potential experts. The 35 individuals represented researchers with expertise in brain injury and professional development (n=2), brain injury and JJ (n=3), education (n=2), and behavioral health (n=2). Important to note two researchers had expertise in multiple areas (e.g., education/behavioral health, brain injury and JJ/ behavioral health). The remaining experts were practitioners with expertise in brain injury and JJ (n=2), education (n=3), physical health (n=1), behavioral health (n= 9), correctional administration (n=8), line staff (n=2), residential (n=1), vocational (n=1), and parole/ probation (n=2). As with researchers, one practitioner had expertise in multiple areas (i.e., brain injury and JJ/behavioral health). The 35 experts were sent an email letter describing the purpose and process of the study and inviting them to participate. Of the 35 experts, 21 responded to the invitation to participate. Of the 21 respondents, 14 were female, 7 were male, 11 were practitioners with two or more years’ service with youth with TBI or in youth correctional facilities, and 5 were authors/ researchers of scholarly, peer-reviewed work relative to brain injury, brain injury and professional development, and/or brain injury and JJ.
Procedures
Data were collected in three phases: (1) clarifying initial competencies from research literature and stakeholder feedback, (2) soliciting input from experts and voting on competencies, and (3) reviewing final competencies to ensure applicability to justice-involved youth with TBI and to determine which training competencies were relevant to professional roles within juvenile correction settings. Next, we describe the process used in each phase of the Delphi procedures.
Phase One
In phase one to develop a thorough understanding of the types of skills and knowledge that various personnel working in juvenile correction settings need to perform their jobs, we conducted a review of existing competency frameworks related to juvenile justice and working with youth with brain injury. We identified multiple frameworks that were relevant to the context, the first of which was In-the-Classroom (ITC) (Glang et al., 2019). These competencies were developed from a National Institute on Disability Independent Living Rehabilitation Research (NIDILRR)-funded project [#90IF0067] and focused on youth with brain injury and return-to-school, screening and services, accommodations and modifications, classroom strategies, promoting social interactions, behavior, transition, parent communication, and other resources. Next was a list of competencies developed by the Criminal Juvenile Justice Administration for Community Living (ACL) Work group (2020). These competencies covered brain injury basics, screening, co-occurring conditions, community-based resources and interventions, symptomology and behavior, and services and supports. Last, was Return to Learn School ACL Work Group Competencies. This set of competencies focused specifically on students who experienced concussions and returning to school.
The research team analyzed each framework to understand its structure, core competencies, and associated levels or proficiency indicators. We identified overlapping or similar competencies across the frameworks and noted any unique or specialized competencies. In this process we established alignment criteria. We considered factors such as relevance to the target context, importance to the desired outcomes, and feasibility of assessment and development. Then the research team created a crosswalk to align similar competencies based on their descriptions, definitions, and performance criteria. We noted differences in wording, emphasis, and depth. Next, we identified overarching competencies (i.e., competencies reflecting core skills and knowledge required to support youth with brain injury in juvenile justice settings) present in the multiple frameworks considered essential in the youth corrections context. The research team then worked to harmonize the competencies by resolving any inconsistencies or discrepancies identified during the comparison process. The team developed a unified language and structure for the competencies that was clear, concise, and aligned with the target context. The team extensively reviewed and modified competencies, converting them into knowledge and skill-based competencies. Knowledgebased competencies started with the word “knows” and the skills-based competencies started with an active verb such as “screens,” “assesses” or “documents”. The research team then categorized the competencies and continued to refine and delete duplicate competencies. The categories included (a) staff awareness/ knowledge of brain injury; (b) screening/identification; (c) eligibility determination; (d) assessment to inform intervention; (e) intervention plans/accommodations; and (f) communication/resource/ referral.
Lastly, we sought feedback from relevant stakeholders. Stakeholders included an international expert in brain injury and juvenile justice and clinical and policy experts in brain injury, juvenile justice, workforce development, and secondary special education and transition. Stakeholders also included a cultural consultant and others with expertise across multiple topics (e.g., education, behavioral health, brain injury and adult corrections, medical rehabilitation). Stakeholders were provided a brief video overviewing the development process along with the competency matrix to review prior to meeting. We then met via Zoom to discuss. Stakeholders were asked to comment on what we missed, what additions were needed, what was included but should not have been, and wording changes needed for the target audience and potential to minimize jargon. Stakeholders shared notes about the relevance of the competency to the context as well as clarity (e.g., language used, complexity of competency). As a result, the research team incorporated the input and made necessary adjustments to ensure the framework was comprehensive and accurate, then moved to phase two.
Phase Two
Phase two was the initial phase in the structured and iterative research process aimed at gathering and synthesizing expert opinions on the competency framework. This phase consisted of soliciting information from the experts through multiple rounds of questionnaires distributed via Qualtrics, an on-line survey software program. We used both qualitative and quantitative procedures to analyze the Delphi process.
Phase two, round one
In round one, respondents were provided the final list of competencies (see Appendix A) generated in phase one. Competencies were organized by knowledge and skills in the following categories: (a) awareness and knowledge, (b) screening and identification, (c) eligibility determination, (c) assessment to inform intervention, (d) intervention plans and accommodations, and (e) community reentry. Respondents were first asked to review each set of knowledge and skills and identify how important the knowledge or skill was in carrying out the responsibilities to support youth with TBI in juvenile settings. Then respondents were asked to describe via an open-text box knowledge and skills they believed individuals working in juvenile settings supporting students with brain injury should know that was not listed. At the end of this round, the research team aggregated responses, eliminated duplicates, refined, or added competencies based on expert recommendations and distributed the complete list of competencies a second time.
Throughout the process of building consensus in round one and subsequent rounds, we were mindful of maintaining our role as researchers and preventing our personal professional experiences from influencing the results. To achieve this, we implemented several strategies to ensure the outcomes accurately represented the intentions of the experts rather than those of the researchers. To minimize researcher bias, we employed the following techniques:
Use of Brackets: We used brackets (i.e., [ ]) to indicate any words inserted by us. This approach made it clear which parts of the results were contributed by the researchers and allowed for transparency in the analysis.
Collaborative Decision-Making: When making decisions, we worked in pairs or triads to promote collective decision-making. This collaborative approach helped in reducing individual biases and encouraged a more balanced and objective assessment of the responses.
Peer Review: Before proceeding further, we checked our decisions with our co-researchers to ensure consensus and validate the objectivity of our assessments. This step provided an additional layer of scrutiny and helped identify and rectify any potential biases or errors.
Expert Validation: To validate and enhance the credibility of the results, we sought input from the experts themselves. We allowed them to vote on recommended changes, ensuring any modifications or adjustments were supported by a collective agreement before moving on to the next round of rankings.
By implementing these strategies, we aimed to uphold the integrity of the research process, minimize any potential biases, and ensure the outcomes accurately reflected the perspectives and intentions of the participating experts.
Phase two, round two
During round two, respondents were asked to review each newly suggested or revised competency and identify how important the knowledge or skill was in carrying out the responsibilities to support youth with TBI in juvenile settings. The research team tabulated the number of respondents indicating a required competency. Competencies were determined critical if a simple majority of respondents (i.e., 50% or higher) responded that it was important and if determined critical they were added to the finalized list of competencies for phase three.
Phase Three
In phase three, respondents were provided the finalized list of knowledge and skills and asked to determine which competencies are necessary for which roles in supporting youth with TBI in juvenile settings. The survey presented each competency, organized by section, and respondents were asked to check the appropriate boxes for which role that competency applied (i.e., correctional administration, line staff, residential staff, vocational staff, parole/probation staff, education staff, physical health staff, behavioral health staff). The research team tabulated the number of respondents indicating a required competency overall and for each of the respective roles. Each competency with a simple majority of respondents (i.e., 50% or higher) for each respective role was considered a critical competency for that role.
RESULTS
Next, we describe the response rate and final competencies identified over the course of the three phase Delphi procedure.
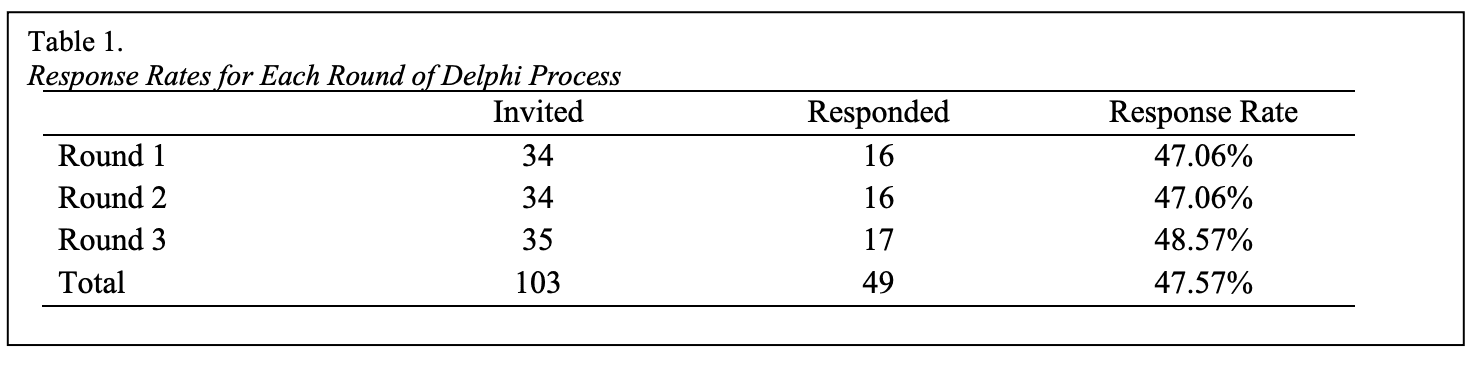
Response Rate
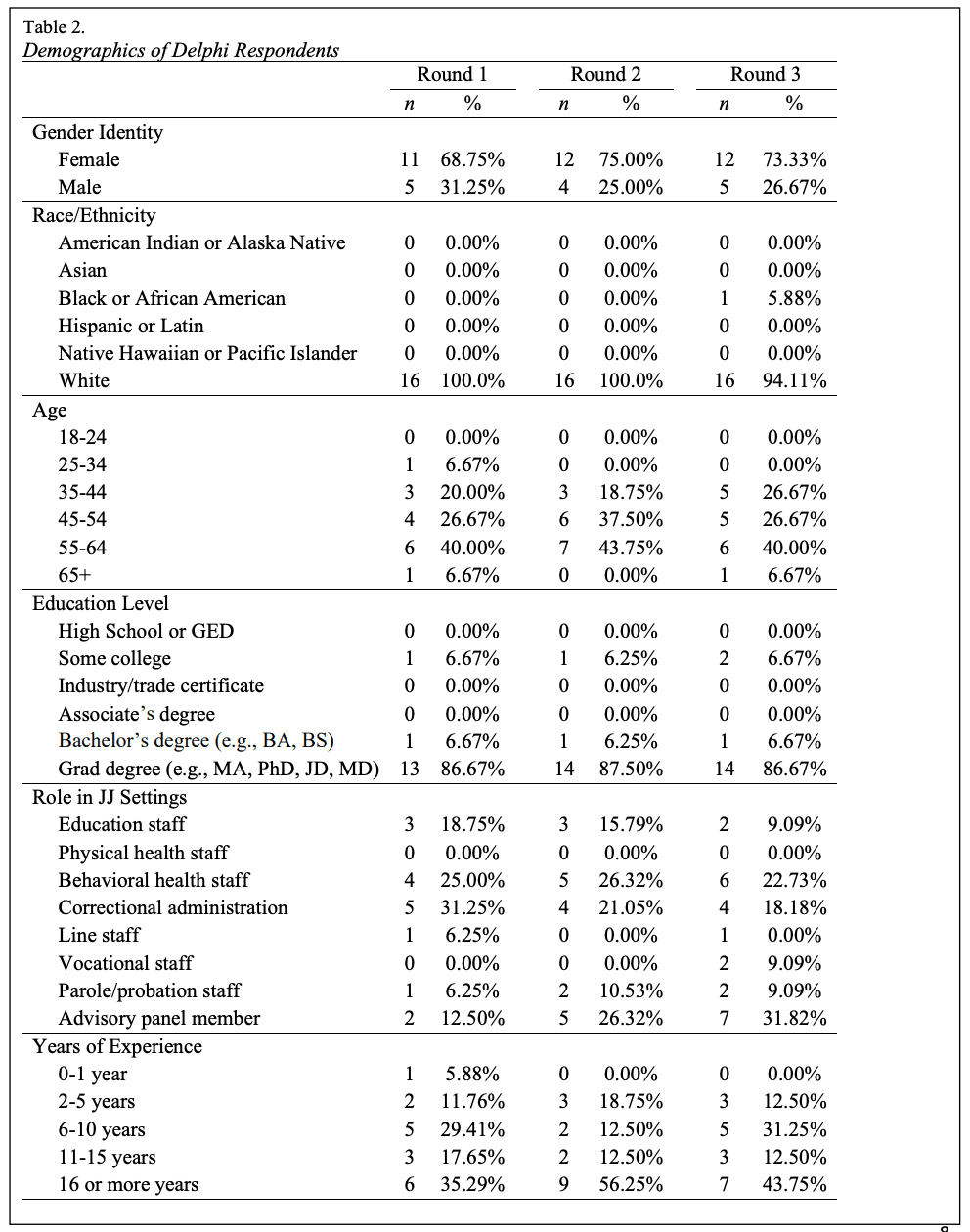
Of the 35 individuals invited to participate as experts in the Delphi study, 21 agreed to participate. In three rounds of voting, experts reached consensus on the core competencies required of facility personnel to adequately support justice involved youth with TBI in juvenile settings. The overall response rate, calculated as total number of respondents by total number of possible respondents across all rounds of ranking, was 48%. Response rates varied across rounds as seen in Table 1. Individuals representing each of the inclusion criteria participated in each round. Five respondents met the first criteria as an author/researcher of scholarly, peer-reviewed work relative to brain injury and/or juvenile justice; thirteen met the second inclusion criteria as a practitioner in juvenile corrections facilities; and five met the third criteria as a practitioner serving youth with TBI. Two respondents met both inclusion criteria one and three. Table 2 presents an overview of the demographic characteristics of respondents.
Final Competencies
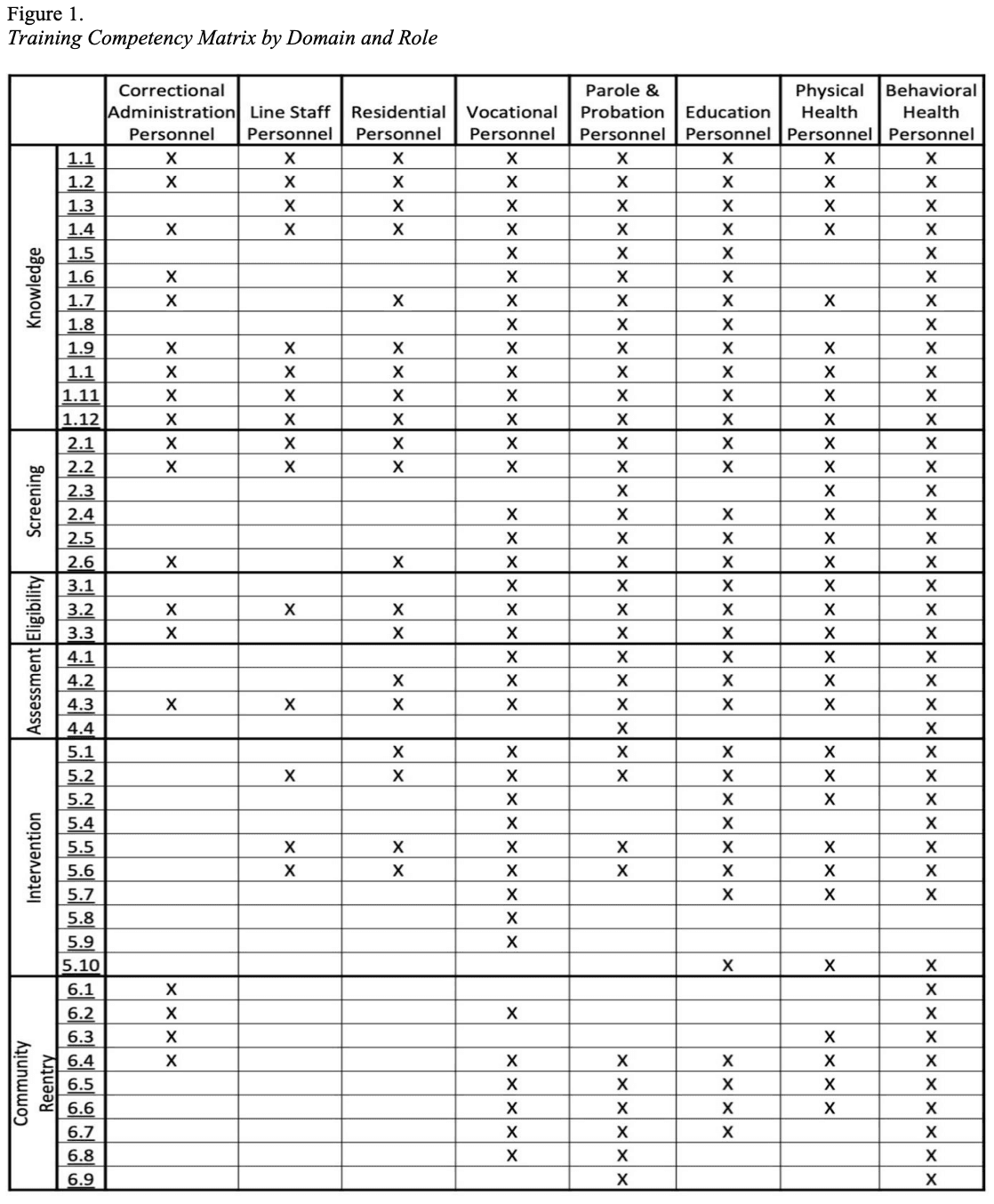
The Delphi process resulted in a final set of 44 competencies divided across six domains: Knowledge (twelve competencies), screening (six competencies), eligibility (three competencies), assessment (four competencies), intervention (ten competencies), and community reentry (nine competencies). See Appendix A for a list of all competencies organized by domain area. Each competency was deemed relevant to at least one of eight role types in juvenile residential settings and eleven competencies were deemed to be necessary across all role types. What follows is a description of the results from each of the three phases of the Delphi process.
Phase 1
Our process for phase one, involving a review of currently existing and relevant frameworks, resulted in 39 competencies among the six domain areas (i.e., eight knowledge, six screening, two eligibility, four assessment, ten intervention, and eight community reentry competencies) that were sent to reviewers for rounds one and two of phase two.
Phase 2
Our expert reviewers in round one of phase two determined that all 39 initial training competencies were essential for individuals supporting youth with brain injury in juvenile settings and as such they were retained for future rounds. Our experts suggested 15 additional competencies (i.e., eight knowledge, four screening, one eligibility, and two assessment) and after review by our research team according to the process detailed in our procedures, it was determined that five new competencies needed to be added. Examples of new competencies added include items like “I can describe how brain injury affects cognition and communication,” and “I recognize that negative early life experiences and trauma can be associated with brain injury and criminal behavior.”
Four pre-existing competencies were revised to incorporate the comments and suggestions from reviewers. Some competencies were revised to add words or adjust stem (e.g., I follow state and federal laws and policies relevant to youth with brain injury in the justice system. [added the words "state and federal" and changed stem to say "I follow"]). Others required further clarification in terms of examples (e.g., Based on brain injury screening results or history of brain injury, I refer youth for further assessment (e.g., school psychological, neuropsychological, employment) [added "history of brain injury" and "e.g."]).
The new and revised competencies were sent back out to our experts for review in round two, resulting in the integration of revisions and the retention of the five newly suggested competencies. This resulted in a finalized competency list of 44 competencies (i.e., twelve knowledge, six screening, three eligibility, four assessment, ten intervention, and nine community reentry competencies).
Phase 3
Phase three involved sending the finalized list of 44 competencies back to our reviewers and asking them to determine which competencies were essential for which of the eight personnel role types that support youth with brain injury in juvenile settings (i.e., correctional administration personnel, line staff personnel, residential personnel, vocational personnel, educational personnel, parole and probation personnel, physical health personnel, and behavioral health personnel). Reviewers determined eleven competencies were necessary across all eight role types and each competency was relevant to, at minimum, one role type. Figure 1 presents a competency matrix that displays the results of this round, using the corresponding competency list in Appendix A as a guide.
The overarching objective of the proposed research was the development of professional training competencies for personnel working with justice involved youth with TBI inside juvenile settings. Justice involved youth with TBI experience unique identification and service needs, and it is unclear whether the vast array of diverse personnel in correctional settings have the knowledge and skills needed to support these youths’ positive re-entry. Through a rigorous, iterative Delphi process we established empirically based core training competencies for juvenile justice personnel.
Limitations
When analyzing these findings, it is important to acknowledge four limitations that should be considered: (a) the selection process of experts, (b) the response rate, (c) the use of online communication, and (d) the potential introduction of bias by the researchers. One primary limitation commonly recognized in studies employing the Delphi procedure pertains to the selection of participants chosen to contribute their experience and expertise to the research (Linstone & Turoff, 2002; Schmidt et al., 2001; Welty, 1972). Despite adhering to stringent inclusion criteria to ensure diversity in content expertise (e.g., JJ, behavioral health, education) and practical application of knowledge (e.g., researchers/ academics and JJ staff), the selection of experts was constrained by our personal knowledge of their research focus, years of experience, and professional work. The selection process did not involve a comprehensive survey of professionals in these fields (e.g., membership of relevant professional organizations) or an analysis of their individual contributions. Therefore, we cannot make any definitive statements about how the opinions of these experts would generalize to other professionals in the field.
A further limitation of this study pertains to the low response rates observed from experts throughout the different rounds. To encourage active participation and completion of all rounds in the Delphi study, initial personal emails were sent to invite individuals to take part. Subsequent emails were sent during each round to remind participants of the study's objective and emphasize the significance of their contribution. While the response rate was below 50% across rounds, it is worth noting that existing literature on Delphi procedures indicates a common issue of declining response rates with each consecutive voting round (Linstone & Turoff, 2002). However, it is important to acknowledge that individuals representing each of the inclusion criteria participated in all phases of the study. This includes authors/researchers of scholarly, peer-reviewed work relative to brain injury and/or juvenile justice (JJ) and practitioners in juvenile justice facilities, or practitioners serving youth with TBI. To increase response rate and maintain a steady rate for the remainder of the study, we included all 35 initially invited experts across rounds in phase two and in phase three.
Third, it is important to note all interactions with experts were conducted solely through electronic communication, such as surveys and emails. Consequently, any intention behind edits or changes could only be expressed in writing. This means if experts had intended to convey different meanings through voice tone or facial expressions, such nuances could not be discerned in the methodology employed, as neither focus groups nor interviews were conducted.
Furthermore, while we made conscious efforts to avoid introducing our personal and professional knowledge into the study and took measures to maintain transparency when altering any wording, it is essential to acknowledge no research study can be completely devoid of bias. It is possible other researchers, when presented with the same suggestions, might have made different edits to the responses. However, it is crucial to emphasize all edits were approved by the respondents themselves. Despite these limitations, the findings of this study hold significant implications for practitioners and researchers alike to consider.
Implications for Practice
Creating a competency framework for staff working with justice involved youth who have experienced TBI brings forth several practical implications. These evidence-based competencies can serve as a foundation for juvenile correction facility administrators to evaluate their existing practices and procedures in supporting justiceinvolved youth with brain injuries. Furthermore, they enable an assessment of the knowledge and skills possessed by current staff members.
Following this assessment, administrators can pinpoint any deficiencies in their current practices and procedures. This allows for necessary adjustments to ensure youth with brain injuries receive the best possible services within the facility. For instance, one potential gap might involve communication breakdowns among different personnel. For example, if a youth is identified as having a prior brain injury through screening, the results might not be shared with school or residential staff, hindering targeted programming in the educational or residential settings.
Moreover, tailored professional development and training programs can be designed for existing staff, along with mandatory training for new hires, ensuring they acquire the required knowledge and skills as part of their roles and responsibilities. Ongoing coaching focused on the specific competencies will guarantee the consistent provision of services to justice-involved youth who have experienced prior brain injuries and require some form of intervention (Lory et al., 2023; Odom et al., 2014; Webster-Stratton et al., 2011). To ensure the mastery of these competencies, they can be incorporated into performance evaluations, serving as a mechanism for maintaining the quality of services offered to youth with brain injuries.
Recommendations for Further Research and Policy Implementation
Identifying essential competencies for effectively serving youth with TBI in juvenile justice facilities represents a crucial initial step in equipping staff with the necessary knowledge and skills. However, translating this research into practical implementation is equally vital. Given justice-involved youth are at a heightened risk of having a history of brain injury (Nagele et al., 2021), it becomes imperative to ensure the application of these competencies within justice settings is best practice.
Further research is required to ascertain the existing policies, practices, and procedures within juvenile correction settings. For instance, in September 2018, the National Partnership for Juvenile Services (NPJS) adopted a position statement regarding the identification and response to justice-involved youth with brain injuries (NPJS, 2018). Investigating the current implementation of this statement within juvenile justice settings is essential. Equally important is the need to examine the re-entry outcomes of justice-involved youth with brain injuries when policies and procedures are established for this demographic. If disparities exist, there may be a rationale for defining more intensive services.
To enhance the generalizability of these competencies, a validation study could be conducted via a survey involving a more diverse array of participants, spanning various personnel roles such as administrators, behavioral health professionals, and residential staff. This survey among diverse stakeholders could also serve as a foundation for systematically reviewing and updating the competency framework as additional best practices for youth with brain injuries emerge.
Finally, despite the existence of training resources for working with students and youth with brain injuries, their adaptability for the context of juvenile correction settings remains uncertain. It is imperative to develop empirically based training modules specifically tailored for juvenile settings, following an iterative process. These modules should be rigorously tested to ensure the effective implementtation of best practices for working with justice-involved youth with TBI.
CONCULSIONS
This study sought to create empirically grounded training competencies tailored to the multifaceted personnel within juvenile justice settings, focusing on youth who are at a heightened risk of having a history of brain injury, which can significantly affect their behavior and cognition. It is our fervent hope these competencies will not merely remain confined within the pages of this research but will be actively embraced and implemented within juvenile justice settings. By doing so, we aspire to see a positive transformation in service delivery and, more importantly, an upward shift in the life trajectories of justice-involved youth who have grappled with the challenges of brain injury. These competencies, when put into action, have the potential to make a lasting and meaningful impact on the lives of the youth we serve, fostering brighter futures and contributing to a more just and inclusive society.