Abstract
Posttraumatic stress disorder (PTSD) has received considerable attention with regard to the ongoing wars in Iraq and Afghanistan. In studies of veterans, behavioral sequelae of PTSD can include hostile and violent behavior. Rates of PTSD found in impoverished, high-risk urban populations within U.S. inner cities are as high as in returning veterans. The objective of this study was to determine whether civilian PTSD is associated with increased risk of incarceration and charges related to violence in a low-income, urban population. Participants (n = 4,113) recruited from Grady Memorial Hospital in Atlanta, Georgia, completed self-report measures assessing history of trauma, PTSD symptoms, and incarceration. Both trauma exposure and civilian PTSD remained strongly associated with increased risk of involvement in the criminal justice system and charges of a violent offense, even after adjustment for sex, age, race, education, employment, income, and substance abuse in a regression model. Trauma and PTSD have important implications for public safety and recidivism.
Posttraumatic stress disorder (PTSD) has recently received attention with regard to soldiers returning from Iraq and Afghanistan. This anxiety disorder can result from experiencing or witnessing a traumatic event that elicits fear, horror, or helplessness. PTSD is characterized by three symptom clusters: re-experiencing the traumatic event, avoiding reminders of the event, and persistent hyperarousal. Since the inception of the diagnosis in Diagnostic and Statistical Manual of Mental Disorders, Third Edition (DSM-III), PTSD has most commonly been understood as a potential consequence of war.
Less public awareness has focused on civilian PTSD, which results from trauma exposure that is not combat related. Much of the research on civilian PTSD has focused on the sequelae of a single, disastrous event, such as the Oklahoma City bombing, September 11th attacks, and Hurricane Katrina. More recently, however, researchers have found alarmingly high rates of trauma and civilian PTSD in populations of inner-city youths and adults whose lives are rooted in continuously stressful and violent contexts.
An epidemiological study of residents of Detroit, Michigan, offers an example of the high prevalence of PTSD among inner-city residents. When compared with those in other areas, inner-city residents were found to be exposed more frequently to all types of trauma assessed in the study, including assaultive violence, other injury or shock, trauma to others, and unexpected death. Among inner-city residents, 54.2 percent experienced assaultive violence, compared with 33.5 percent of residents from other areas. Inner-city residents in Detroit were nearly twice as likely to be at risk of PTSD than were those living in the suburbs. Similar studies of participants from other U.S. inner cities show high rates of trauma exposure and a strong prevalence of PTSD. Researchers interviewing patients at Howard University Hospital in the District of Columbia found that 65 percent (n = 617) of the sample experienced at least one event that was sufficiently traumatic to initiate the onset of PTSD symptoms. Of the traumatized sample (n =279), 51 percent met diagnostic criteria for lifetime PTSD.
From 1977 to 2005, the number of inmates in the United States has increased 400 percent, and both race and income levels are strongly associated with risk of involvement with the criminal justice system. Such mass incarceration may pose a threat to public health. For example, incarceration is associated with increased risk for negative health outcomes, including higher rates of infectious diseases such as hepatitis, tuberculosis, and HIV. Other negative health outcomes (e.g., hypertension) are more common among individuals with a history of incarceration, even after adjustment for other risk factors.
Research on veterans has found behavioral sequelae of PTSD to include aggressive, hostile, and violent behavior. Incarcerated veterans with PTSD have more serious legal problems than do incarcerated veterans without the disorder, offering convincing yet inadequate evidence of a relation between PTSD and involvement in the criminal justice system. Although violent crime rates in inner cities are significantly higher than those in rural and suburban areas, researchers have yet to investigate whether civilian PTSD is associated with higher levels of illegal behavior, particularly violent behavior in inner-city, adult populations, which have the highest rates of incarceration. We examined whether trauma exposure and civilian PTSD are associated with a history of violent charges and incarceration among inner-city residents of Atlanta, Georgia. This study has two main hypotheses: highly traumatized participants will report more substantial incarceration records than will participants with less trauma exposure and participants with a PTSD diagnosis will report greater instances of incarceration than will those who have no diagnosis of PTSD, even after accounting for trauma exposure.
Methods
Recruitment and Procedures
The participants (n = 4,113) were recruited from the waiting rooms of primary care (nonpsychiatric) medical clinics at Grady Memorial Hospital in Atlanta, Georgia, from 2005 to 2011. Recruitment consisted of a cross-sectional, randomized approach in a sample of convenience obtained from those seated in public hospital waiting areas. An interview that included self-report measures on demographic characteristics, trauma exposure during childhood and adulthood, current PTSD symptoms, and history of incarceration was completed. Each participant was compensated $15 for taking part in the interview. We also performed more in-depth interviews of a subset of 531 participants who returned to complete an additional measure that assessed lifetime PTSD. These subjects were compensated $60 for participating in this secondary interview. Because the literacy of the participants varied, all self-report measures were obtained by verbal interviews.
Written, informed consent was obtained for all participants. Exclusion criteria included mental retardation, active psychosis, and age less than 18 years. All procedures in this study were approved by the Institutional Review Board of Emory University.
Measures
An assessment of demographic characteristics included questions on the participant’s sex, self-identified race, education, employment, household income, alcohol and drug abuse history, and history of PTSD treatment. Information on legal history was obtained through a self-report measure that assessed the presence and frequency of arrests, jail sentences, and imprisonments. In addition, participants reported any encounters with the criminal justice system that were due to a charge involving violence. Childhood trauma was assessed using the Childhood Trauma Questionnaire (CTQ), a self-report inventory assessing childhood physical, sexual, and emotional abuse. The internal consistency, stability over time, and criterion validity of the original 70-item and the current brief versions have been established. Adult trauma was assessed using the Traumatic Events Inventory (TEI), a 14-item measure investigating trauma exposure in childhood and adulthood. In addition to screening items for physical and sexual abuse as well as being involved in or witnessing a life-threatening accident, the questionnaire also includes trauma exposures relevant to an inner-city population, including having a close friend or family member who has been murdered, being attacked with a knife or gun, or being attacked by another person with the intent to kill. The TEI accounts for both the frequency of exposures and the age at which the traumatic events first occurred. For the purposes of this study, adulthood trauma included incidents occurring at age of 18 or older. The PTSD diagnosis was determined with the Modified PTSD Symptoms Scale (PSS). A psychometrically valid, 18-item measure, the PSS assesses the frequency of PTSD symptoms during the two weeks before rating and distinguishes between intrusive, avoidance, and hyperarousal symptoms. We based the categorical diagnosis of PTSD on DSM-IV criteria A through E responses to the PSS questionnaire (A, presence of trauma; B, presence of at least one re-experiencing symptom; C, presence of at least three avoidance/numbing symptoms; D, presence of at least two hyperarousal symptoms; and E, present for at least one month). We used the Clinician Administered PTSD Scale (CAPS) to compare current with lifetime PTSD diagnoses. An interviewer-administered measure, the CAPS has established psychometric properties and assesses both current and lifetime PTSD.
Statistical Analyses
Demographic data, including sex, race, education, employment, income, and substance abuse history were analyzed across PTSD status with chi-square analyses; categorical variables from the legal history form (ever been arrested, jailed, imprisoned) were also included in a chi-square analysis with PTSD status. Continuous measures of PTSD symptoms, according to the total and subcluster PSS scores and trauma history scores (CTQ, TEI), were assessed with univariate analyses of covariance (ANCOVA), with legal history variables as between-groups factors and demographics and substance abuse as covariates. Finally, a logistic regression was performed to determine if trauma exposure and PTSD symptoms contributed independently to incarceration, after accounting for the demographic and substance abuse variables. All analyses were performed with SPSS16 for Windows.
Results
The Sample
The majority (n = 3,811; 93.1%) of the participants self-identified as African American (Table 1). Nearly a quarter (n = 979; 23.9%) of the subjects had not earned a high school diploma, and less than one-tenth (n = 331; 8.1%) had obtained a college degree. The majority (n = 2,825; 69.1%) of the participants were unemployed during the time of the interview. More than half (n = 2,511; 63.3%) had household monthly incomes of less than $1,000. More than a quarter (n = 1,126; 27.7%) had substance abuse problems before the interview.
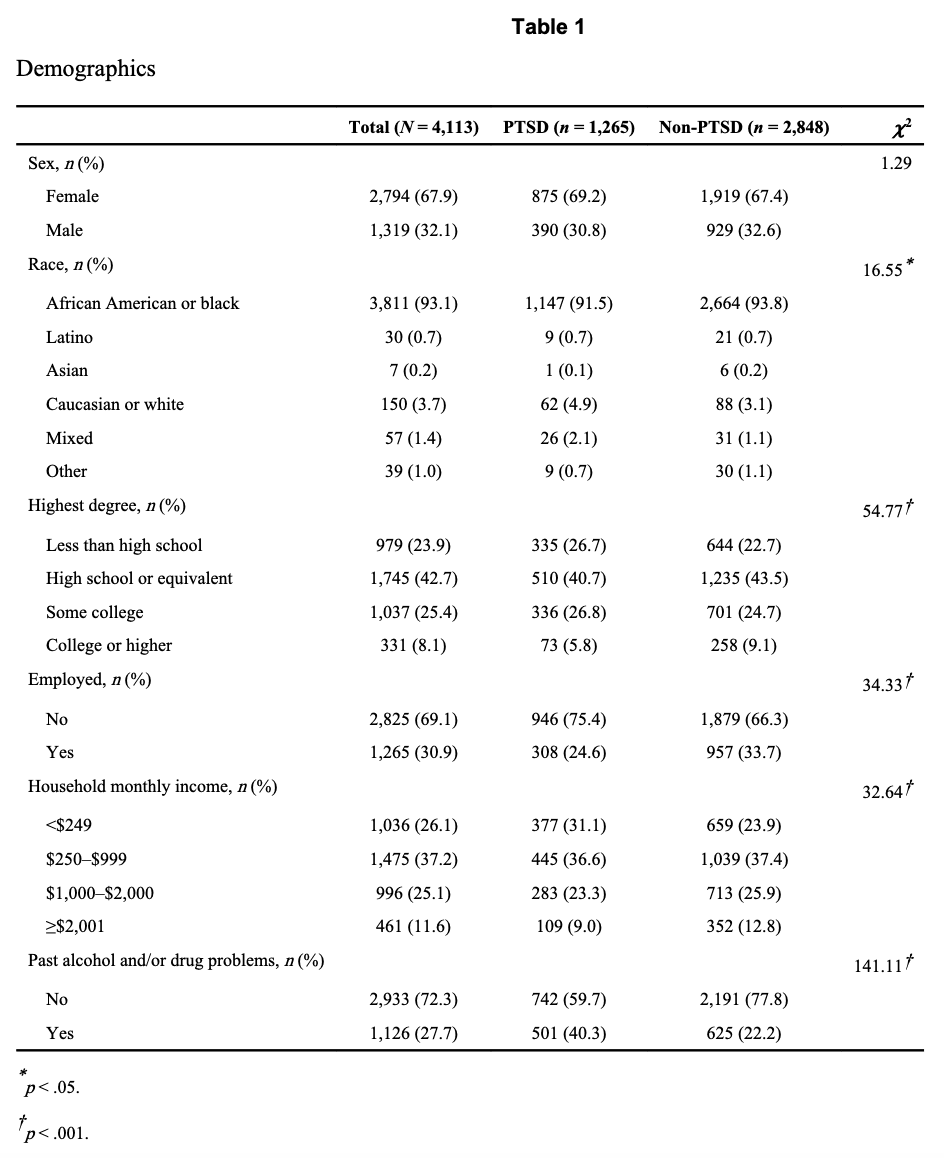
The results are expressed as the mean ±SE. Thirty percent (n = 1,265) of the participants met the diagnostic criteria for current PTSD at the time of the interview, based on the PSS. Within this PTSD-positive group, only 13 percent (n = 161) reported having been treated for PTSD. The subjects with PTSD were found to have significantly higher levels of childhood trauma (CTQ, 49.49 ± 0.57) when compared with the subjects who did not have PTSD (CTQ, 37.02 (0.26; F(1,4068) = 516.7; p < .001). In addition, the PTSD subjects had experienced significantly more types of adult trauma (TEI, 5.71 ± 0.08) than the non-PTSD subjects had (TEI, 3.37 ± 0.05; F(1,4003) = 624.5; p < .001). The participants in the PTSD group were significantly more likely to be unemployed (χ2 =34.33; p <.001) and to have a history of alcohol and drug problems (χ2 = 141.11; p < .001). Of the participants who completed the CAPS interview (n = 531), those who endorsed current PTSD symptoms on the PSS were also more likely to meet diagnostic criteria for lifetime PTSD on the CAPS (χ2 = 44.3; p < 10e-5).
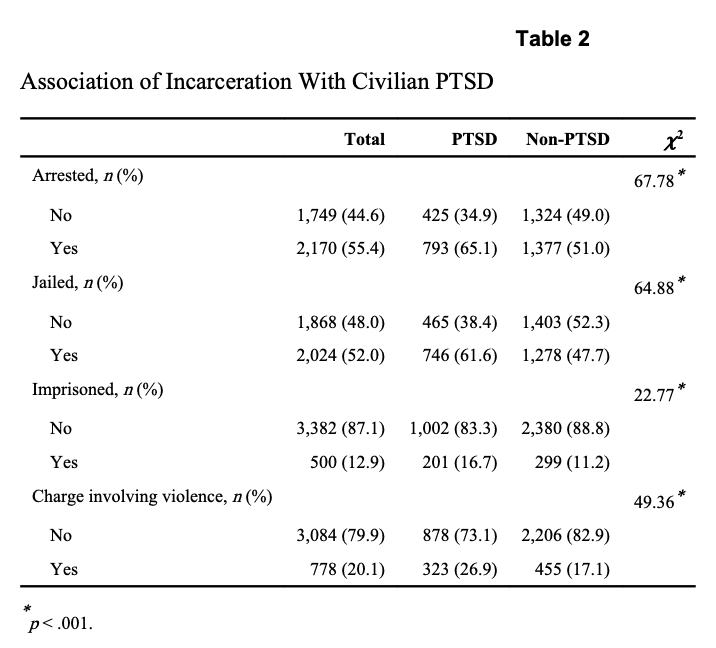
Overall, legal difficulties were common in this sample. More than half the participants had experienced an arrest (n = 2,170; 55.4%) and jail time (n = 2,024; 52.0%), 12.9 percent (n = 500) had served time in prison, and 20.1 percent (n = 778) had been arrested or incarcerated for a charge involving violence (Table 2).
PTSD Is Associated With Incarceration History
The participants with PTSD were significantly more likely to have encountered the criminal justice system in more than one way (Table 2). Specifically, when compared with the participants without PTSD, those with PTSD were significantly more likely to have been arrested (χ2 =67.8; p <.001), to have served time in jail (χ2 = 64.9; p < .001) or prison (χ2 = 22.8; p < .001), and to have been charged with a violent offense (χ2 =49.4; p <.001). Arrest, incarceration, and violent offense charges were particularly common among the males with PTSD. Of those, 88 percent (n = 330) had been arrested, 87 percent (n = 326) jailed, 36.3 percent (n = 131) imprisoned, and 37.1 percent (n = 138) charged with a violent offense.
When an ANOVA was performed with the frequency of offenses as the dependent variable, the results were similar. The participants with PTSD experienced more arrests (4.64 ± 0.26) than did those without PTSD (3.37 ± 0.20; F(1,2657) = 14.39; p < .001). Those with PTSD experienced more jail sentences (4.45 ± 0.28) than did those without PTSD (3.02 ± 0.15; F(1,2554) = 24.3; p < .001). Finally, the subjects with a diagnosis of PTSD experienced, on average, a greater number of prison sentences (0.86 ± 0.08) than did the subjects who did not have the diagnosis (0.54 ± 0.05; F(1,1496) = 13.4; p < .001).
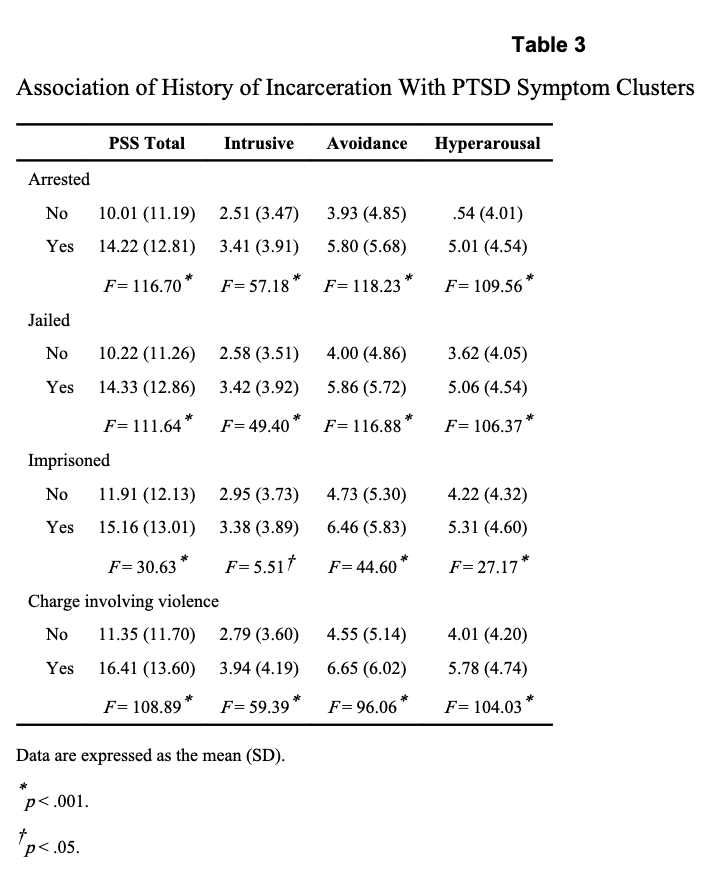
When PTSD symptom clusters were examined separately, the participants who had a history of any type of illegal activity experienced significantly higher intrusive, avoidance, and hyperarousal symptoms than did those who did not have such a history (Table 3). More specifically, the participants who were charged with a violent offense had more symptoms in all three PTSD clusters than did those who were never charged with a violent offense.
Trauma Is Associated With Incarceration History
Arrest, incarceration, and violent charges were highly associated with a history of childhood trauma (Table 4). An ANOVA showed that the participants who experienced arrest, served time in jail or prison, or had charges of violent offenses had significantly higher levels of childhood trauma than those who did not.
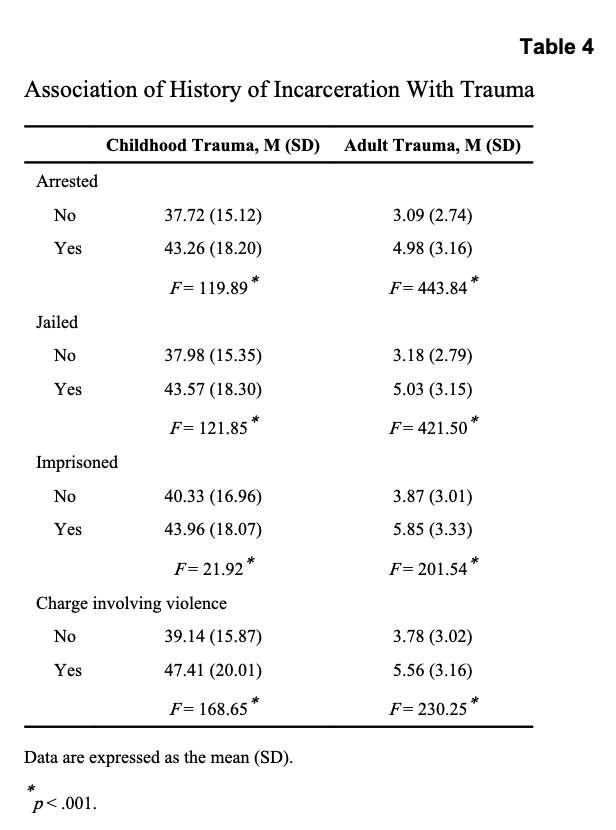
History of incarceration and history of violent charges were also associated with adult trauma (Table 4), in that the participants with all types of charges, arrests, and incarceration had significantly higher levels of adult trauma relative to the comparison group.
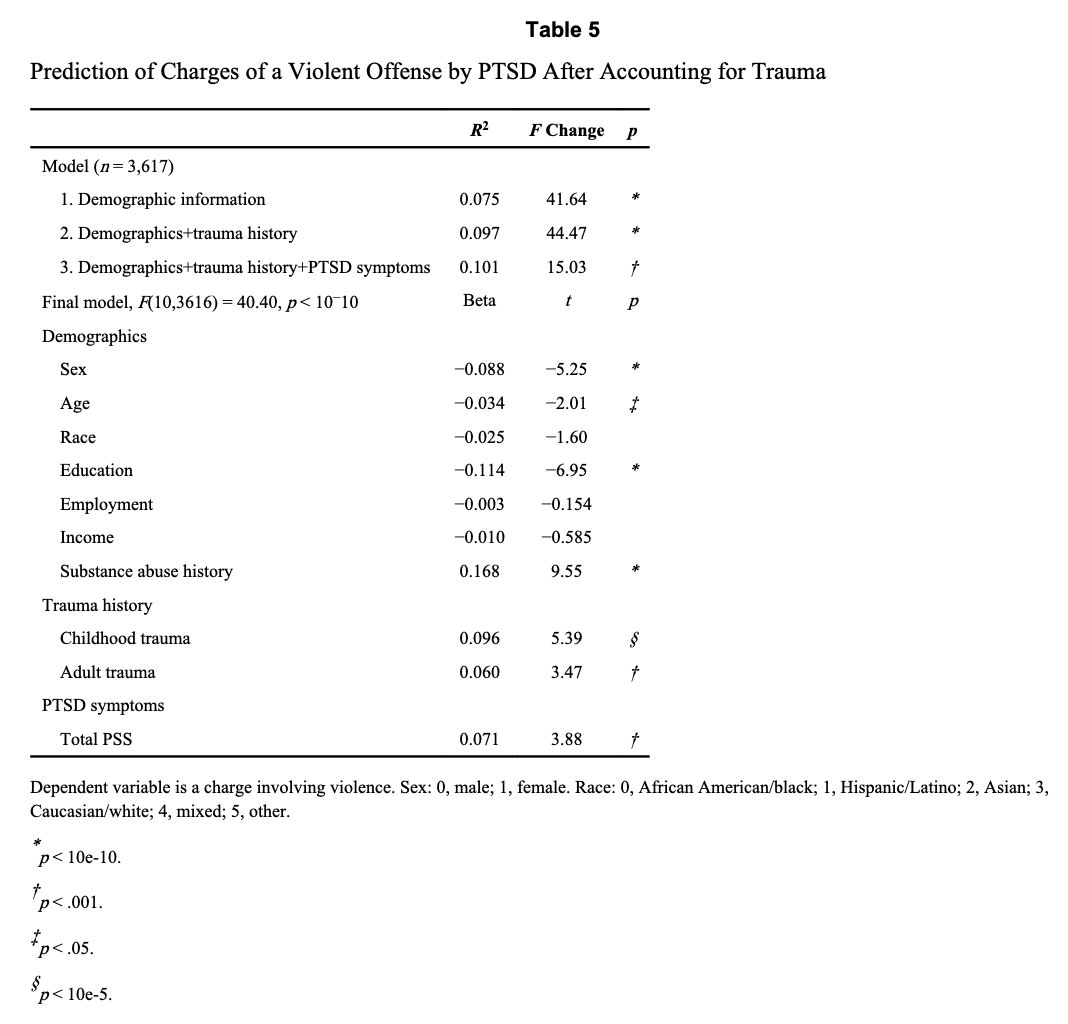
Trauma and PTSD Both Contribute to Charges Involving Violence
To examine whether PTSD remained significantly associated with legal history, even after adjustment for potentially confounding variables, we performed a hierarchical stepwise regression entering demographic information in the first step, trauma history in the second, and PTSD symptoms in the third (Table 5). We performed a regression analysis for the incarceration history variable associated with violence (ôHave you ever had an arrest, jail, or prison charge involving violenceö) entered as a dependent variable. Charges involving violence were significantly associated with both trauma history (F2nd step(2,3617) = 44.5; p < .0001) and PTSD symptoms (F3rd step(1,3617) = 15.0; p < .001), independently. Table 5 shows the regression model for charges involving violence. The overall model was significant (F(10,3616) = 40.4; p < .0001), accounting for 10.1 percent of the variance.
Discussion
As established in previous studies of this population, rates of trauma and PTSD in this sample were notably high. Of an inner-city sample (n = 4,113) of Grady Memorial Hospital patients in Atlanta, 30.8 percent (n =1,265) met current diagnostic criteria for PTSD. As seen previously, PTSD was vastly under-recognized and undertreated in inner-city communities, with only 13 percent (n =161) of these 1,265 subjects reporting prior treatment for PTSD. The sample as a whole experienced a considerable amount of legal difficulties. However, when incarceration histories were compared between the PTSD and non-PTSD groups, the subjects with PTSD were more likely to have been arrested, jailed, imprisoned, and charged with a violent crime. In addition, a strong association was found between trauma exposure and incarceration histories. A stepwise hierarchical regression showed that trauma histories were significant in predicting arrest, jail, and imprisonment. However, PTSD symptoms were strongly associated with violent charges, even after adjustment for sex, age, race, education, employment, income, substance abuse, and trauma history. Both hypotheses of the study were supported: the participants with more extensive trauma histories and those with a diagnosis of PTSD reported more substantial incarceration records than did those with less extensive trauma histories who did not have the diagnosis. The results of this work support findings from previous studies illustrating the relationship between PTSD and violent behavior. This study adds to previous findings by identifying this association in an inner-city, civilian sample and providing evidence that the behavioral sequelae of civilian PTSD are related to exposure to the criminal justice system.
The current study has several noteworthy strengths, limitations, and implications. First, it is well documented that mental health symptoms are more prevalent in incarcerated populations than in community populations. Most frequently, researchers replicate these findings in institutionalized samples. The current study provides evidence that the relation between incarceration and mental health symptomatology is not limited to samples that are institutionalized at the time of assessment. Nonpsychiatric, community populations with a history of involvement with the criminal justice system may also be at risk for psychiatric symptoms. However, because the current assessment of legal history, trauma history, and PTSD symptomatology did not provide a timeline of events, a cause-and-effect relationship between post-trauma symptomatology and involvement with the criminal justice system could not be established. Because of the prevalence of lifetime PTSD among subjects with active PTSD symptoms and the high level of childhood trauma in the sample, it is possible that for some participants, the behavioral sequelae of post-trauma symptomatology contributed to the likelihood of later involvement in the criminal justice system. Conversely, it may be that exposure to the criminal justice system contributed to some participants’ post-trauma symptomatic behavior. It is also possible that PTSD symptoms developed either from committing the violent offense or during the participant’s incarceration.
Although definitive conclusions cannot be made from the current evidence, the study’s findings warrant further empirical investigation of models that explain the relation between post-trauma symptoms and involvement with the criminal justice system in community populations. Finally, among African American, inner-city populations, arrests and prosecutions are far more common than in other populations, and wrongful arrests and prosecutions are more likely to occur. It is probable that the incarceration histories of some participants do not reflect purely illegal and violent behavior, especially considering that a charge of violence does not invariably result in conviction for the offense. Future studies should consider the use of official legal records in combination with self-reports of criminal justice system contact. Nonetheless, the current study’s use of self-reports of criminal justice system contact is warranted, considering the accuracy of retrospectively reporting salient and unique experiences.
It has been well established that women are more likely to develop PTSD symptoms. In contrast, men with comorbid mental health conditions have higher rates of incarceration. Although we concluded that both trauma and PTSD are associated with violent charges even after adjustment for the individual’s sex, further examination of the intersection of sex, trauma, and risk for incarceration is warranted. Similarly, certain psychiatric conditions have been associated with increased risk of incarceration, including bipolar disorder, substance use disorders, schizophrenia, and other psychotic illnesses. It is possible that the risk of incarceration for some of the participants was related to other psychiatric comorbidities.
Commendably, PTSD is of concern to the United States Department of Veterans Affairs, and efforts are being made to increase awareness of the disorder among veterans and the general population. Concern for the mental health of veterans has been accompanied by funding for services; the President’s proposed budget via the Office of Management and Budget for the 2013 fiscal year includes $662 million dedicated to veterans’ traumatic brain injuries and psychological health. The disparity in interest and services for veterans and civilians should be attended to, as neglect of civilian PTSD as a public health concern may be compromising public safety. This study has shown that trauma and civilian PTSD are highly prevalent among inner-city residents and are strongly associated with incarceration histories and frequency of violent charges. Addressing trauma and PTSD has important implications for public safety and recidivism.