Abstract
Importance: Posttraumatic stress disorder (PTSD) is a common psychiatric illness, increasingly in the public spotlight in the United States due its prevalence in the soldiers returning from combat in Iraq and Afghanistan. This educational review presents a contemporary approach for how to incorporate a modern neuroscience perspective into an integrative case formulation. The article is organized around key neuroscience "themes" most relevant for PTSD. Within each theme, the article highlights how seemingly diverse biological, psychological, and social perspectives all intersect with our current understanding of neuroscience.
Observations: Any contemporary neuroscience formulation of PTSD should include an understanding of fear conditioning, dysregulated circuits, memory reconsolidation, epigenetics, and genetic factors. Fear conditioning and other elements of basic learning theory offer a framework for understanding how traumatic events can lead to a range of behaviors associated with PTSD. A circuit dysregulation framework focuses more broadly on aberrant network connectivity, including between the prefrontal cortex and limbic structures. In the process of memory reconsolidation, it is now clear that every time a memory is reactivated it becomes momentarily labile-with implications for the genesis, maintenance, and treatment of PTSD. Epigenetic changes secondary to various experiences, especially early in life, can have long-term effects, including on the regulation of the hypothalamic-pituitary-adrenal axis, thereby affecting an individual's ability to regulate the stress response. Genetic factors are surprisingly relevant: PTSD has been shown to be highly heritable despite being definitionally linked to specific experiences. The relevance of each of these themes to current clinical practice and its potential to transform future care are discussed.
Conclusions and relevance: Together, these perspectives contribute to an integrative, neuroscience-informed approach to case formulation and treatment planning. This may help to bridge the gap between the traditionally distinct viewpoints of clinicians and researchers.
In the Clinical Challenge in this issue of JAMA Psychiatry, we describe the case of a soldier who experienced multiple life-threatening events during a military deployment and then struggled with a number of problems on his return home.
Although the details of the case are contemporary, the overall arc of the narrative is hardly new. Through much of history there are accounts of similar individuals who, following exposure to a life-threatening event, have struggled to readjust to “normal” life. These accounts include descriptions in The Odyssey of soldiers returning from the Trojan war and of a survivor of the Great Fire of London in the 1600s. At different times in history, various names have been used to describe the broad phenomenon of difficulty recovering from combat experiences, including nostalgia or soldier's heart (Civil War), shell shock (World War I), battle exhaustion (World War II), and post-Vietnam syndrome. Although some core features are similar across these entities, each has distinct aspects reflecting the unique time and culture.
In 1980, in part because of political factors, the DSM-III introduced the diagnosis of posttraumatic stress disorder (PTSD). These criteria were held constant until publication of the DSM-5 in 2013 (although experts continue to debate this nosology, including vis-à-vis what constitutes a traumatic experience and the role of complex neuroscience domains in diagnosis).
Phenomenologically, most individuals who are exposed to traumatic events experience transient aftereffects that resolve within the first month (eg, numbness or hyperemotionality, nightmares, anxiety, and hypervigilance). In a minority of individuals (approximately 10%-20%, depending on the type of trauma), these symptoms may persist and cause lasting and potentially debilitating dysfunction.
With PTSD—perhaps more than with other psychiatric illnesses—it is critical to recognize the context of each individual's personal history: prior experiences (including trauma or resilience), belief systems, culture, social supports, and myriad other exacerbating and protective factors. As psychiatrists, we aspire to treat people rather than diseases—doing so requires a broad approach that incorporates diverse clinical perspectives. Within this complexity, a range of biological factors play crucial roles. To this end, we review a set of core neuroscience themes relevant to PTSD.
Theme 1: Fear Conditioning
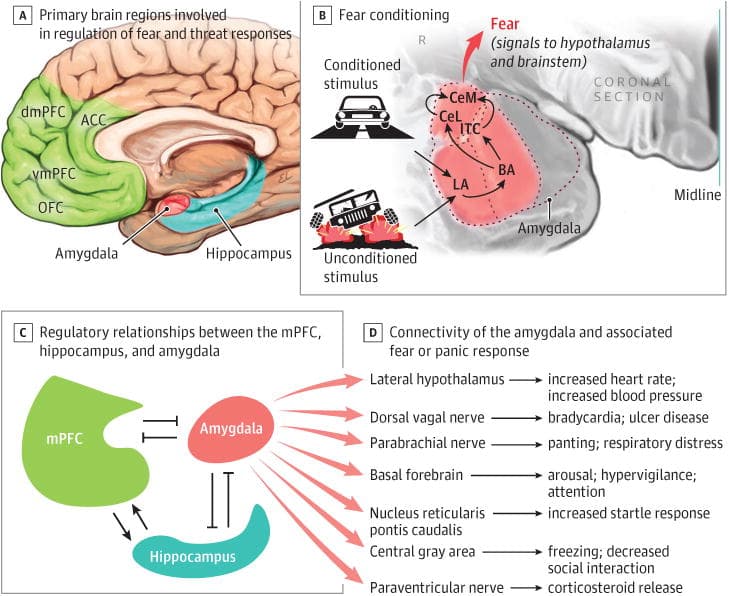
Any conversation about the neurobiology of PTSD needs to begin with what happens in the brain following a traumatic event. How does the brain, from the lowest vertebrates to humans, reflexively respond to a life-threatening event to ensure survival? We study this process through a behavior called fear (or threat) conditioning, a form of classical conditioning in which an innate response to an unconditioned stimulus (eg, a shock or other unexpected painful stimulus) becomes associated with another previously neutral (conditioned) stimulus. From an evolutionary perspective, this form of learning is highly adaptive: it is very beneficial to know—and thereby avoid—contextual cues that may predict dangerous outcomes.
When an individual experiences a traumatic event (eg, as happened to the soldier described in the Clinical Challenge1), the physiologic response to the trauma can become paired with previously neutral environmental cues. Long after the precipitating traumatic event, environmental cues will continue to serve as triggers for a similar physiologic response. This process corresponds to the DSM-5 symptom of intense or prolonged distress after exposure to traumatic reminders (Table). The patient may be consciously aware of these triggers, such as walking on a city street or being in the desert. Importantly, there may also be subtle contextual cues that induce symptoms of fear and anxiety without conscious awareness of the trigger (eg, fleeting peripheral movement, an unexpected object at the side of the road, or even the aroused emotional response of asexual partner). The physiologic responses of increased startle, hypervigilance, increased heart rate and respiration, dry mouth, and emotional reactivity and defensive behavior may all be triggered by these experiences, with the most extreme experiences activating a flashback in which the patient has temporary difficulty separating past traumatic experiences from the present. Figure 1 shows a diagram of the basic neural circuits that are relevant to fear conditioning.
Table. DSM-5 Symptoms and Related Neuroscience Constructs.
DSM-5 Symptoms | Related Constructs Informed by Neuroscience |
|---|---|
Intrusive recollection: intense or prolonged distress after exposure to traumatic reminders | Classical fear conditioning or the pairing of an innate response (startle, increased heart rate and respiration, dry mouth, and emotional reactivity) to an unconditioned stimulus (eg, a shock or other unexpected painful stimulus) with another previously neutral (conditioned) stimulus |
Avoidance symptoms | Operant conditioning or negative reinforcement when a behavior that leads to the avoidance or removal of an aversive stimulus is increased in frequency |
Increased arousal | Abnormalities in regulation of the sympathetic nervous system and the hypothalamic-pituitary-adrenal stress response (perhaps through epigenetic changes) |
On multiple levels, it is not surprising that individuals exposed to trauma would avoid situations that remind them of these events. This process reflects a form of operant conditioning (Box) known as negative reinforcement, that is, when a behavior that leads to the avoidance or removal of an aversive stimulus is increased in frequency. This process correlates with the DSM-5 category C avoidance symptoms of PTSD. For example, a patient exposed to an ambush while traveling in a military convoy abroad may subsequently avoid driving on major roads at home so as to prevent the physiologic and affective response that occurs with trauma reminders. As described in the accompanying Clinical Challenge, because speaking about traumatic experiences may be a potent trigger of negative affect, the patient may also avoid therapy. This avoidance is a significant barrier to treatment and may underlie recent concerns about certain forms of therapy being less effective in the real world.
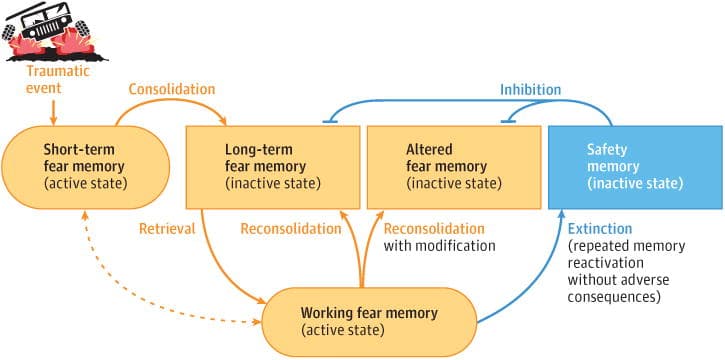
Box. PTSD Terms and Definitions. Classical Conditioning Classical conditioning is a process wherein an innate response to a specific stimulus (eg, salivating at the sight of food) becomes paired to a neutral stimulus (such as a bell ringing) by repeated presentation of the two stimuli, in the case of appetitive classical conditioning. One prototypical example of aversive conditioning is fear (or threat) conditioning, in which an aversive event (unconditioned stimulus) triggers autonomic arousal and intense fear (the unconditioned response) and contextual cues in the environment (eg, sights, sounds, and smells) become conditionally associated with the trauma. The conditional cues will then trigger the experience of autonomic arousal and intense fear as in the original situation (the conditioned response) as shown in Figure 1. Operant Conditioning Operant conditioning, by contrast, is a process by which behaviors are increased or decreased in frequency based on the presence of rewards or noxious stimuli. Reinforcement means that a behavior is increased in frequency based on either the presence of reward (positive reinforcement, as seen in cocaine-seeking behavior) or the removal/avoidance of a noxious stimulus (negative reinforcement, as seen in avoidance of unpleasant situations/circumstances). Punishment means that a behavior is decreased in frequency based on either the addition of a noxious stimulus (positive punishment, such as spanking a child) or the removal of a rewarding stimulus (negative punishment, such as taking away a child's toys). Extinction The term extinction was originally coined in a behavioral context: repeated exposure to a conditioned stimulus led to the disappearance of the fear response behavior. Recent work, however, has shown that the conditioned association and response can be brought back (reinstated) by re-exposure to the fear-inducing cue. Thus, it appears that behavioral extinction paradigms are actually teaching individuals to overlearn a safety association on top of the existing fear conditioning. This contrasts with the discussion of reconsolidation that occurs later in this article (a process which may genuinely alter or disrupt the memory of an event). A visual schematic of these opponent processes is shown in Figure 2. |
Fear conditioning and the avoidance of conditioned contextual cues are adaptive in a dangerous environment—they support survival. However, the same behaviors become maladaptive when one is returned to a safe environment, where rational, nonreactive, and socially “appropriate” responses are preferred over defensive reflexes. In this regard, ongoing PTSD in the aftermath of trauma exposure may be thought of as a failure to unlearn adaptive thoughts and behaviors on the return to a safe place.
The best evidence-based treatments for PTSD are forms of psychotherapy that are designed to reverse the lasting impact of fear conditioning (eg, prolonged exposure therapy and cognitive processing therapy). To do so, patients are encouraged to engage and process traumatic memories in the absence of the feared out-come. Early on in treatment, patients may experience increased anxiety as they engage with these difficult memories. However, over time, exposure to the conditioned stimulus in a safe environment without the expected adverse outcome can lead to habituation (weakening of the intensity of response to a stimulus over time) and extinction (the conditioned stimulus is no longer associated with the aversive unconditioned stimulus) (Box). A visual schematic of these opponent processes is shown in Figure 2. Helping patients understand this process—critically, including the role of negative reinforcement and avoidance in perpetuating symptoms, and that these are robust neurobiological phenomena—may improve patients' motivation, decrease their self-doubt about recovery, and improve their ability to engage in therapy.
Future Directions
One promising line of inquiry is the use of plasticity-enhancing agents, such as d-cycloserine, apartial agonist of the N-methyl-d-aspartate receptor, to augment the effects of psychotherapy. By increasing the brain's capacity for learning, these medications may allow patients to complete an exposure-based therapy more rapidly, as shown in studies of acrophobia. Although d-cycloserine it self has limitations, enhanced plasticity may be a shared mechanism of action by which other medications benefit patients with PTSD: for example, a known downstream effect of selective serotonin reuptake inhibitors is to increase brain-derived neurotrophic factor and thereby enhance plasticity.
A different approach to treatment may be to interfere with the initial process of fear conditioning. The strength of an initial memory will depend on many factors (eg, it maybe increased in the context of elevated norepinephrine levels, as seen in trauma). There is also a temporal window during which the consolidation of this initial memory occurs. Thus, in some circumstances, it may be possible to disrupt or diminish the strength of the initial encoding. This principle underlies both medication trials (eg, with propranolol and opiates) to potentially prevent the onset of PTSD and, similarly, forms the rationale for early cognitive-behavioral interventions.
Theme 2: Dysregulated Circuits
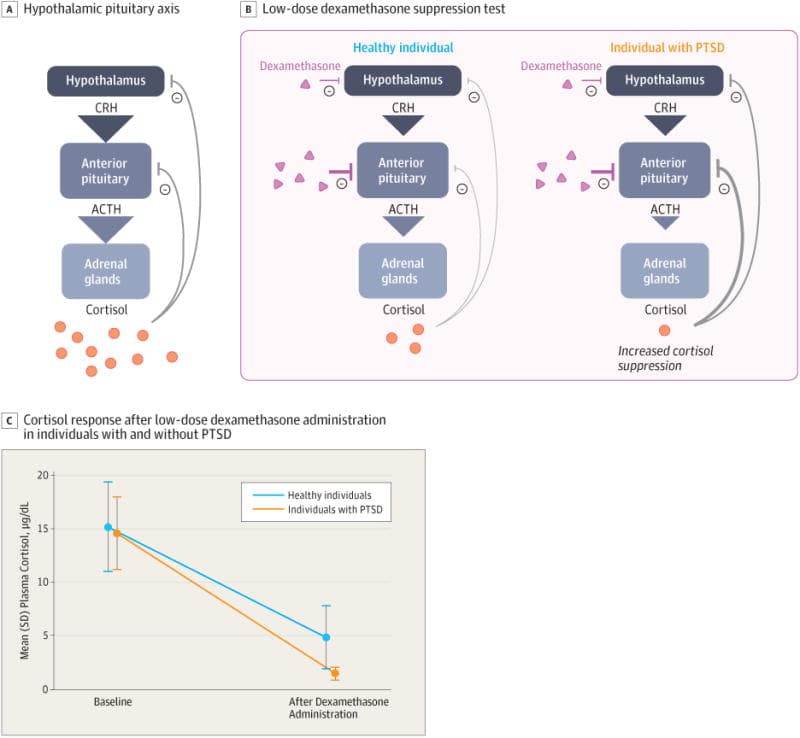
Some of the earliest research findings with PTSD suggested abnormalities in regulation of the sympathetic nervous system and the hypothalamic-pituitary-adrenal (HPA) axis. This hypothesis led to clinical trials with adrenergic blockers (eg, clonidine and prazosin) that ultimately were not shown to be effective, although recent research has found prazosin to be effective for treating trauma-related nightmares, in part through its α-1 antagonist properties in normalizing sleep. The most common HPA dysregulation finding included enhanced cortisol suppression following low-dose dexamethasone treatment. These data suggested enhanced sensitivity to glucocorticoid activation. More recent work has also suggested that the stress response system may be hyperreactive to triggers, both in the magnitude of response and in the time it takes to return to baseline. Figure 3 illustrates aspects of the above-described commonly observed aspects of HPA dysregulation seen in individuals with PTSD.
Connecting this work back to the basic circuit diagrammed in Figure 1, a core aspect of normal functioning is the reciprocal inhibition between the medial prefrontal cortex (mPFC) and the amygdala: during stress, limbic activation inhibits PFC functioning; conversely, PFC activity is able to inhibit the amygdala and, resultantly, decrease the stress response. Individuals with PTSD may have a regulatory imbalance in which amygdala activation is exaggerated while the function of the PFC is diminished. Much work on the output of amygdala activation has led to a greater understanding of many of the downstream neural pathways that mediate the enhanced startle response, hyperarousal, increased heart rate, and other core aspects of response to fear and threats.
From this perspective, a wide range of treatments for PTSD may share a central therapeutic mechanism of restoring balance between PFC and amygdala function. Selective serotonin reuptake inhibitors may exert their benefit by decreasing hyperreactivity in the amygdala. In addition, different forms of psychotherapy may help individuals restore top-down (PFC) control to regulate arousal and anxiety. A helpful line of inquiry comes from research into the phenomenon of resilience. This area of work aims to identify factors that protect individuals from developing PTSD. Resilient individuals have been shown to have better regulation of their stress response, mediated by a number of possible pathways, including neuropeptide Y. It has also been shown that early exposure to manageable stress may confer resilience toward future trauma—a process known as stress inoculation.
Future Directions
As described above, many current treatments align well with a circuit-based model of PTSD including, most notably, forms of psychotherapy that may help to restore balance between PFC and limbic structures.
In recent years, considerable research in psychiatry has explored the role of a wide range of interventional approaches to help regulate circuits. These interventions include electroconvulsive therapy, deep brain stimulation, vagal nerve stimulation, and, more recently, repetitive transcranial magnetic stimulation and transcranial direct current stimulation. To date, research findings with interventional approaches for PTSD have been limited. However, one might hope that these methods may eventually prove to be able to restore balance to dysregulated circuits by altering function in specific regions.
Theme 3: Memory Reconsolidation
Autobiographical memories are formed when stimuli that represent an experience are encoded in working and short-term memory and then consolidated into long-term memory. At one time, it was thought that such memories were indelible and reflected the initial information that was encoded. Recent research, including examining the accuracy of “flashbulb memories” for major events (eg, the assassination of President Kennedy or the 9/11 terrorist attacks), has suggested a different story.
The concept of memory reconsolidation is that every time a memory is recalled it is momentarily made labile and then needs to be reconsolidated. During this process, the memory may be updated or changed based on new experience. From this perspective, any particular memory may be thought of as being only as old as the last time it was recalled (Figure 2).
This process has clear implications in PTSD. For better or for worse, each time a traumatic experience is recalled, the patient's memory may be updated. Returning to our Clinical Challenge patient: left to his own, one imagines that each time he recalls the trauma there is a high potential that the reconsolidation process may reinforce prior beliefs and interpretations (likely including cognitive distortions around guilt, responsibility, and self-blame);in contrast, in the context of therapy one might view this as an opportunity for a combination of fear extinction, as outlined above, along with updating the memory to incorporate new data and perspectives into a more adaptive overall representation.
Future Directions
There is considerable interest in developing treatments that may capitalize on this process. Some behavioral therapies have been explicitly designed to leverage the reconsolidation process. Other studies have sought to combine therapy with pharmacologic agents that may help to block the reconsolidation of traumatic memories (eg, propranolol or xenon gas, the latter of which is thought to inhibit the N-methyl-d-aspartate receptor). A recent study also demonstrated the possibility of using the globally amnestic properties of electroconvulsive therapy to disrupt the reconsolidation of memories.
Theme 4: Epigenetic Considerations
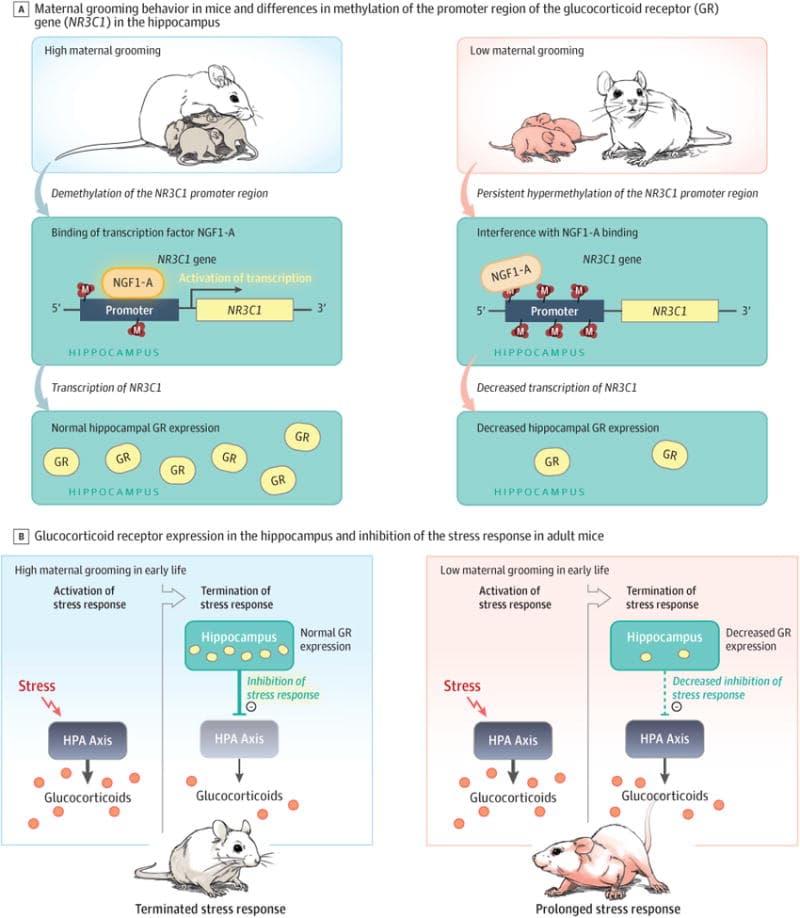
Epigenetics refers to mechanisms (eg, DNA methylation or histone acetylation) by which environmental exposures may influence the functional expression of genes. A large amount of literature has demonstrated that early childhood neglect or trauma can epigenetically program the stress system, leading to aberrant regulation of the HPA axis and maladaptive, prolonged responses to stressors en-countered later in life. This effect appears to occur by the inhibition of the expression of hippocampal glucocorticoid receptors(GRs) via DNA methylation along the GR gene promoter.
As illustrated in Figure 4, GRs in the hippocampus are central to effective regulation of the HPA s axis. Under ideal conditions, the body is able to mount a cortisol stress response that quickly shuts off once the danger has passed. This response occurs through negative feedback at the level of the GR (with increased density of receptors correlating with improved regulation). Studies of rodents and humans suggest that GR expression is significantly reduced by childhood abuse or neglect and that this difference persists into adulthood. These individuals then have inefficient negative HPA feed-back and a prolonged stress response, similar to that in patients with PTSD.
From this perspective, for the veteran we have been discussing, it is clinically important to recognize that his history of childhood trauma is itself a risk factor for developing PTSD and other psychiatric illnesses (including depression and substance use disorders), perhaps in part through a dysregulated stress response system. Of interest, this same process of dysregulated stress response may also be associated with a range of other health problems, including heart disease and stroke, thus giving cause for increased vigilance in routine health monitoring.
Recent work has also provided evidence that epigenetic mechanisms may be able to act across generations, possibly being transmitted through gametes. Thus, environmental exposures experienced by an individual may even affect gene expression in offspring, with potentially broad influences including susceptibility to trauma. In this regard, clinicians should be thoughtful in obtaining a family history and also in considering supports and resources that may be appropriate for patients' children and other family members.
Future Directions
Several researchers are exploring the potential value of an epigenetic perspective for the diagnosis and treatment of PTSD. Major areas of inquiry include whether epigenetic data could be used to identify populations at risk for developing PTSD, to help diagnose PTSD, and as biomarkers to predict who will respond to specific types of treatment. Early positive findings for each of these ideas have been shown in studies that examined military service members before and after deployment. Of particular interest, some patterns of methylation that are associated with PTSD were shown to be reversed during the course of psychotherapy, thus suggesting that, although epigenetic changes are enduring, they are not immutable.
There is also interest in developing pharmacotherapies that could help modify epigenetic changes. The best-explored line of inquiry has examined histone deacetylase inhibitors. In animal models, these medications have been shown to augment fear extinction through multiple complex pathways, including brain-derived neurotrophic factor and N-methyl-d-aspartate receptor signaling. To date, these ideas have not translated into clinical populations, although sodium valproate seems to have some action as a histone deacetylase inhibitor, possibly accounting for some of its efficacy in a broad range of psychiatric disorders.
Of course, the ideal intervention from an epigenetic perspective would be to implement interventions that either prevent early trauma and/or minimize its long-term impact. Improved public health measures would be invaluable.
Theme 5: Genetic Considerations
As alluded to above, a central research question is why, in the face of trauma, only some individuals develop PTSD. Despite the disease being definitionally linked to an external event, research studies (eTable in the Supplement) have consistently shown that PTSD is highly heritable (approximately 40%-50%). Here, we would continue to emphasize that there are many nonbiological factors that may also confer risk or resilience. As far as identifying specific risk genes, findings to date have been mixed, likely reflecting methodological challenges, including the difficulty of achieving adequate sample sizes in which cases can be compared with trauma-exposed controls. The most promising findings have involved genes influencing molecules that are associated with neural plasticity (eg, brain-derived neurotrophic factor), neural inhibition (γ-aminobutyric baacid), and stress response (glucocorticoids). A large, recent genome-wide association study reflecting more than 13 000 trauma exposed soldiers found no genome-wide significant loci in their main analysis. The investigators found the association of a single nucleotide polymorphism at genome wide significance in the ANKRD55 gene (known to be involved in inflammatory and autoimmune disorders) only in African American participants. The authors of that study noted that their sample size may not have been adequately powered to detect other significant findings. The eTable in the Supplement highlights key findings pertaining to the recent genome-wide association study of unbiased genetic approaches to understanding PTSD.
As discussed above, and as with all patients, it is important to take a careful family history. Given the frequent role of guilt and self-blame as a core aspect of PTSD (now acknowledged in the DSM-5 criterion of “persistent, distorted cognitions about the cause or con-sequences of the traumatic event(s) that lead the individual to blame himself/herself or others”), discussing biological predisposing factors may be a valuable tool in the process of therapeutic communication.
Future Directions
A major obstacle in psychiatric practice today is that clinical diagnoses are based on behaviorally defined criteria that may encompass heterogeneous populations at a neurobiological level. The Research Domain Criteria project was created with the goal of understanding psychiatric illness based on relevant neurobiological domains. This parallels broader efforts—most notably in oncology—to move toward precision medicine.
From this perspective, understanding relevant genetic contributions serves 2 purposes. First, identifying genes implicated in PTSD may help researchers better understand underlying molecular mechanisms, which could inform the development of future treatments. Second, it is possible that patterns in gene expression may allow us to identify subgroups that are either at risk for PTSD or are more likely to respond to a specific treatment.
Caveats and Additional Perspectives
Throughout this article, we have discussed PTSD in a relatively generic manner, as if it were a single diagnostic entity. Of course, in psychiatry every case is unique, as is especially true with trauma. Factors that may affect both the incidence and severity of PTSD include type of trauma (eg, natural disasters vs assault vs motor vehicle accidents vs combat related), severity of the trauma (in conjunction with an individual's pre-existing resilience/vulnerability), the cultural context of the event, and the individual's perception and interpretation of the event. This last idea is especially relevant for cognitive models of PTSD (consider, as an example, the literature on “moral injury”) and is also reflected in the considerable controversy regarding the update made to DSM-5 criteria.
In addition, although we have generally discussed PTSD as a discrete condition, it is highly comorbid with other psychiatric illnesses, including depression and substance use disorders. Each of these possible diagnoses would carry its own implications for formulation and treatment planning.
Another important caveat with respect to neuroscience is that much of our understanding comes from animal models. Although useful in many ways, these models are also intrinsically limited. This point may be especially relevant to our discussion of fear conditioning, wherein the protocols used to induce fear conditioning in animals may differ greatly from the types of experiences that cause PTSD in our patients.
Finally, although we have selected 5 key themes to discuss, there are obviously other relevant domains. One especially important area relates to sleep, in which there is extensive literature on rapid eye movement disturbances that occur following trauma. Although findings have been variable, it is plausible that sleep disruption plays a central role in the development and/or persistence of PTSD symptoms.
Conclusions
Modern neuroscience is leading to dramatic shifts in how we understand psychiatric illness. Amid this revolution, PTSD is one of the disorders (along with substance use disorders) for which we have the most compelling evidence relating to the underlying neurobiology. In this article, we have highlighted 5 compelling neuroscience themes relevant to PTSD: the role of fear conditioning and associated processes (including extinction and negative reinforcement); a circuit-based perspective, with a central emphasis on the reciprocal inhibitory connections between the mPFC and the amygdala; the new concept of memory reconsolidation, suggesting that any time a memory is reactivated it becomes briefly labile and thereby amenable to strengthening or weakening; the role of epigenetics, including extensive data on how early traumatic experiences may lead to long-term dysregulation in the HPA axis; and the role of genetic factors in this highly heritable disease, opening doors for new research approaches and, perhaps, someday leading to a precision medicine–based approach.