Abstract
Background Adverse childhood experiences (ACEs) have a profound impact on individuals, shaping their long-term health and life opportunities. This study delves into the complex ties between ACEs and the socioemotional development of Australian children and youth by examining the relationships between adverse childhood experiences and externalizing, internalizing, and prosocial behaviors. Methods This study utilized data from the Longitudinal Study of Australian Children and employed the generalized estimating equation method to investigate the relationships between adverse childhood experiences and externalizing, internalizing, and prosocial behaviors in Australian children and adolescents. Results Adverse childhood experiences such as physical punishment, hostile parenting, parental conflicts, separation, financial strain, and parental mental health issues increased the risk of externalizing and internalizing behaviors while reducing prosocial behaviors. The risk increases with the number of ACEs, as evidenced by the incidence ratio (IR); for example, for externalizing behaviors, an ACEs score of one leads to IR = 1.69, while an ACEs score of 4 results in IR = 3.34. Similar trends were observed for internalizing and prosocial behaviors. Limitations The presence of imbalanced longitudinal data, arising from variations in the number of observations across different time points, challenges robust inferences. Furthermore, this study investigates the relationship between ACEs and behavioral problems, without establishing causality. Consequently, the results should be interpreted with caution. Conclusions The findings of this study highlight that adverse childhood experiences significantly influence behavioral outcomes in children and adolescents. These findings underscore the critical need for early detection and intervention to mitigate the consequences of traumatic childhood experiences.
1. Introduction
Adverse childhood experiences (ACEs) are pivotal traumatic events that children experience during their formative years, impacting not only their immediate well-being but also their long-term health and socioemotional landscape. These experiences, which include physical, emotional, or sexual abuse; financial hardships; and exposure to family discord, substance abuse, or mental illness, are known to have long-lasting repercussions on both the physical and psychological health of children and adolescents (Felitti et al., 1998; Hoppen and Chalder, 2018; Kessler et al., 2005).
The profound physiological changes attributed to these early traumatic events, marked by disruptions in the nervous, endocrine, and immune systems, are a direct result of prolonged exposure to toxic stress (McEwen, 2006; Scientific Council, 2014; Shonkoff et al., 2012). These internal changes often manifest externally in various dysfunctions, from psychological to social, as children transition into adulthood (Danese and McEwen, 2012; Shonkoff et al., 2012). Therefore, significant attention has been given to preventing and addressing the consequences of ACEs, especially in pediatric and adolescent populations (Herzog and Schmahl, 2018; Tonmyr et al., 2020).
Indeed, contemporary studies have consistently underscored the significant link between early exposure to ACEs and an increased risk of engaging in delinquent behavior, along with subsequent manifestations of anxiety and depression during childhood and adolescence (Bellis et al., 2016; Elmore and Crouch, 2020; Hughes et al., 2017; Hughes et al., 2016; Jackson et al., 2023; Jones and Pierce, 2021). Notably, this association appears to follow a grade function association (Hoffmann and Jones, 2022): when children experience multiple ACEs, they are more likely to develop maladaptive emotional regulation (e.g., anxiety and depression) and personality traits, such as anger and callousness (Jones and Hoffmann, 2023; Kalmakis and Chandler, 2015; Lindert et al., 2014; Pervanidou and Chrousos, 2007). Furthermore, multiple ACEs have been found to have an impact on the amygdala, thereby increasing susceptibility to various psychological and somatic disorders (Cheng et al., 2021; Guyer et al., 2008; Herzog and Schmahl, 2018). Therefore, the neurological and emotional responses stemming from chronic ACEs exposure during childhood are strongly associated with an elevated risk of externalizing, internalizing, and poor prosocial behaviors in children and adolescents and persist into later stages of life (Herzog and Schmahl, 2018; Hicks et al., 2021a, Hicks et al., 2021b; Lee et al., 2020).
Previous research has further shown gender-specific responses to ACEs. Studies indicate that girls often exhibit pronounced internalizing behaviors such as sadness and fear(Brody and Fischer, 2000; Brody et al., 2008), while boys may display more externalizing behaviors such as aggression and delinquency (Daughters et al., 2009). Furthermore, some studies have suggested that exposure to ACEs can lead to both externalizing and internalizing behaviors in girls, including hyperactivity and depression(Gajos et al., 2023; Gajos et al., 2022; Leban, 2021). Similarly, boys experiencing a greater number of ACEs tend to engage in more antisocial behavior (Schilling et al., 2007). Despite these insights, there is a gap in the literature regarding how ACEs affect children's developmental trajectories by gender. One of the aims of this study is to explore these nuanced developmental paths and their relationships with emotional and behavioral competence and prosociality over time across genders.
Despite considerable global research on ACEs, comprehensive longitudinal studies, particularly within the Australian context, are lacking. Current research shows that approximately 89 % of Australian youth encounter at least one ACEs (Holmes et al., 2021; Loxton et al., 2021; Malvaso et al., 2022). However, detailed investigations into how ACEs influence various behavioral outcomes (externalizing, internalizing, and prosocial behaviors) by gender remain limited. In particular, a generalized estimating equation (GEE) model, which is crucial for analyzing correlated longitudinal data from repeated measurements over time, is lacking. Additionally, this study employed latent class analysis (LCA). This method is used to identify homogeneous subgroups within a population that have comparable combinations of ACEs risk factors(Masyn, 2013). This approach was instrumental in efforts to dissect the complex relationships between ACEs and a spectrum of behavioral outcomes, including externalizing, internalizing, and prosocial behaviors(Barboza, 2018; Bevilacqua et al., 2021; Nurius and Macy, 2008). Therefore, this paper addresses a critical gap in the literature concerning the relationships between ACEs and gender-specific behavioral development in children and adolescents, utilizing data from the Longitudinal Study of Australian Children (LSAC).
We hypothesize that an increase in ACEs frequency will be positively correlated with heightened internalizing and externalizing behaviors but inversely associated with prosocial behaviors. Additionally, we hypothesize that the relationships between specific ACEs and these outcomes will be distinct and significant, varying across individual experiences. This study makes several significant contributions to the literature. First, it explores the nuanced relationships between individual ACEs, cumulative ACEs, and emotional, behavioral, and prosocial dimensions in children and adolescents. Second, it investigates potential gender-specific relationships with ACEs and how these relationships differ across different ages, thereby enriching our understanding of their developmental implications. Compared with international research, this study offers new insights into how individual ACEs, and ACEs scores are correlated with specific behavioral outcomes. This comprehensive examination underscores the need for a holistic approach to support the well-being of children and adolescents facing adversity.
2. Method
2.1. Study setting, study design, and sample
This study utilized data from the birth cohort of the Longitudinal Study of Australian Children (LSAC), a nationally representative and ongoing household survey of Australian children that began in 2004. The LSAC employs a multistage cluster sampling technique and collects data biennially from parent 1 (primary caregiver), who is the biological mother of the child, in 95 % of cases. In the absence of a biological mother, data were gathered from fathers, grandparents, adopted parents, and stepparents. For adolescents aged 12 and older, the LSAC directly obtains data from the participants themselves. Structured questionnaires were used to collect the data from parents and adolescents.
In this study, we comprehensively utilized data on ACEs collected from parent 1 when the study children were aged 4–5 and 6–7 years or from waves 3 and 4. Subsequently, we use SDQ data collected from both parents and adolescents, spanning from wave 3 to wave 8. The baseline observation included 4386 participants at wave 3, with follow-ups extending to wave 8, resulting in a final sample size of 3127 participants. In total, six data points were considered over the 12 years of follow-up. The detailed methodology of the LSAC is available in other sources (Soloff et al., 2005).
2.2. Dependent variables/outcome variables
2.2.1. Measurement of externalizing, internalizing, and prosocial behaviors
Externalizing, internalizing, and prosocial behaviors are the outcome variables of this study and were assessed using the Strength and Difficulties Questionnaire (SDQ) (Goodman, 1997). The SDQ is a reliable tool for assessing children's and adolescents' emotional, behavioral, and social well-being across five domains: hyperactivity, emotional difficulties, conduct problems, peer problems, and prosocial behaviors (Goodman, 1997; Goodman et al., 2000). In the LSAC, the SDQ measures externalizing behaviors using five items from hyperactivity scales (e.g., restlessness, constant fidgeting, easily getting distracted, taking a moment to think before acting, and a good attention span) and five items from the conduct problems scale (e.g., temperament, compliance with requests, frequent involvement in fights/bullying, arguing with adults, and displaying spiteful behavior toward others). Internalizing behaviors are similarly assessed using the emotional scale (e.g., headache complaints, signs of worry, unhappiness, nervousness, and fear) and the peer problems scale (e.g., playing alone, likability among peers, bullying experiences, quality of relationships with adults, and having at least one close friend). Furthermore, pro-social behaviors (e.g., desire to share with peers, providing support through injuries, kindness with younger children, and a proclivity to volunteer for aid) are measured using the pro-social behavior scale. The responses to the SDQ items were recorded on three-point Likert scales: “Not true,” “Somewhat true,” and “Certainly true”. The sum of the scores within each scale determined the levels of externalizing, internalizing, and prosocial behaviors, showing good internal reliability, with alpha values ranging from 0.7 to 0.9(Goodman et al., 2000). Elevated SDQ scores were associated with externalizing and internalizing behavioral problems, whereas prosocial behaviors were associated with lower SDQ scores in children and adolescents. Conversely, lower scores indicated a positive behavioral and emotional state but a deficit in prosocial behaviors among this age group. It is important to note that, on average, the SDQ score was employed to establish the behavioral, emotional, and prosocial status of Australian children and adolescents. These outcome variables were assessed from wave 3 to wave 8 (i.e., when the participants were aged 4 to 15 years) and analyzed as continuous variables.
2.3. Independent variables
2.3.1. Measure of adverse childhood experiences (ACEs)
Adverse childhood experiences were the key predictors identified in this study. The ACEs is a widely acknowledged and validated tool for assessing childhood adversity (Felitti et al., 1998). Childhood adversity encompasses various aspects, including physical abuse, psychological abuse, childhood sexual abuse, and household dysfunction. Household dysfunction includes exposure to domestic violence, parental separation, parental loss, financial adversity, substance abuse, mental health challenges, and criminal activities within the family context. These ACEs checklists are instrumental for evaluating their potential long-term impacts on adult health, including the development of a wide range of serious and potentially life-threatening conditions (Bellis et al., 2016; Felitti et al., 1998).
Building on existing research, our study concentrated on adversities that are commonly recognized as childhood adversities and have been thoroughly evaluated during early childhood stages (Bethell et al., 2017; Bevilacqua et al., 2021; O'Connor et al., 2020). These adversities were also examined in the LSAC, starting at wave 3 when the children were aged 4 to 5 years. We identified ten types of adverse conditions that met these criteria, as detailed in the online Appendix Table 1. Within the LSAC dataset, ACEs were measured using a checklist encompassing items related to the following measures. The following ACEs data were collected when the study children were 4–5 years old (i.e., wave 3) and 6–7 years old (i.e., wave 4):
a) Physical Punishment: To gauge the extent of physical punishment, the LSAC employed the following question: “How often were you punished as a child?” Participants responded on a 5-point Likert scale (1 = never or almost never, 5 = always). Subsequently, we categorized the responses into binary variables, with “All the time,” “More than half the time,” “Approximately half the time,” and “Less than half the time” coded as “Yes,” while “Never/almost never” was coded as “No.”
b) Hostile Parenting: Hostile parenting was assessed using four distinct questions directed toward both fathers and mothers:
“Of all the time you talk to this child about his/her behavior, how often is this shout?”
“Of all the time you talk to this child about his/her behavior, how often is this disapproval?”
“How often are you angry when you punish this child?”
“How often do you feel you are having problems managing this child in general?”
Responses to these questions were recorded on a five-point Likert scale (1 = Never, 5 = Many times each day). A binary variable was created by summing the responses. Specifically, we classified “many times each day,” “one or two times a day,” “once a week or less,” and “a few times a week” as “yes,” while categorizing “never” as “no.”
c) Intraparental conflict: Intraparental conflict was assessed using four questions directed toward both fathers and mothers:
“How often do husbands/wives disagree about basic child-rearing issues?”
“How often do husbands/wives have awkward or stressful conversations?”
“How often do husbands/wives argue with each other?”
“How often do husbands/wives express anger or hostility toward each other?”
Responses were recorded on a five-point Likert scale (1 = Never, 5 = Always) and were aggregated to create a binary variable. Responses indicating “Always,” “Often,” “Sometimes,” and “Rarely” were coded as “Yes,” while responses indicating “Never” were coded as “No”.
d) Parental mental illness: The mental well-being of parents was measured using the K-6 depression scale score. Parents were asked about their frequency of experiencing nervousness, hopelessness, restlessness, worthlessness, and difficulty cheering up in the past 4 weeks. Responses to these questions were recorded in binary form, with “0” indicating no probable serious mental illness and “1” indicating the presence of serious parental mental illness.
e) Problematic alcohol use: Data on problematic alcohol use were obtained from parents. It is defined as “regularly consuming more than four alcoholic drinks per day for men or more than two for women, occurring two to three times a month or more frequently”. Responses were coded dichotomously, with “1” indicating problematic alcohol use by parents and “0” indicating no problematic alcohol use.
f) Parental separation: Parental separation was assessed by asking the following question: “Have you experienced separation due to relationships or marital difficulties?” The responses were recorded in binary form, with children living without parents coded as “Yes” and those living with parents coded as “No.”
g) Legal Problems: Legal problems were evaluated using the following question: “In the last year, have you and your partner had problems with the police or a court appearance?” The responses were binary, with “Yes” and “No” options.
h) Drug Problems: Drug problems were measured by asking, “In the last year, have any of the following happened to you (or your partner) or someone in your household had a drug problem?” Responses were recorded as “0” for No and “1” for Yes.
i) Death of Family Members: The occurrence of a family member's death was measured by asking, “Has your partner or child died in the last year?” Responses were recorded as “0” for No and “1” for Yes.
j) Financial Hardship: Financial hardship was assessed using six questions from hardship scales, which were asked to parent 1. The responses were recorded in binary form, with “1” indicating financial hardship (=Yes) and “0” indicating no financial hardship (=No).
In sum, based on the previous literature, we calculate the ACEs scores by summing the binary values for each individual ACEs (Webster, 2022). The ACEs scores were categorized into four groups: no ACEs, 1 ACEs, 2 ACEs, 3 ACEs, 4 ACEs, and >4 ACEs.
2.4. Other variables
This study controlled for several sociodemographic covariates when fitting the GEE model with a Poisson distribution. These covariates included the child's age, which was divided into three groups, namely, early childhood (4–5 years), middle childhood (6–11 years) and adolescence (12–15 years), gender (e.g., male and female), ethnicity (e.g., Aboriginal and Torres Strait Islander and no Aboriginal and Torres Strait Islander), parental education (e.g., postgraduate, certificate/diploma, and year 12 class or below), household income (e.g., lowest income, medium lowest income, medium highest income, and highest income), and parental employment status (e.g., employed, unemployed, and not in the labor force).
2.5. Statistical analysis
Initially, this study employed descriptive statistics to calculate the frequency, percentage, and mean of the variables. Second, latent class analysis was used to determine the ACEs class. The categorization of the ACEs class was determined by employing Akaike's information criterion (AIC), the Bayesian information criterion (BIC), and the log-likelihood ratio (Nylund et al., 2007). The best-fit models are characterized by lower BIC, AIC, and likelihood ratios (McLachlan et al., 2019; Tein et al., 2013). Based on these criteria, we selected five ACEs clusters for the study participants. However, we did not use the LCA due to the low entropy level.
To examine the relationships between ACEs and internalizing and externalizing behaviors in children and adolescents, we utilized generalized estimating equation (GEE) models with a Poisson distribution to analyze the data. The Poisson distribution assumes that the mean and variance of a set of observations are equal. If the variance is larger than the mean, it is referred to as overdispersion. Fortunately, in this study, the Poisson distribution is equal to the mean, which does not exhibit over- or underdispersion in the model. Therefore, the model selected in this study was the GEE with a Poisson distribution (Gardner et al., 1995). In addition, we specifically tested the interactions of gender and age group with the number of ACEs. This approach allowed us to examine the relationships between ACEs and three behavioral outcomes, externalizing, internalizing, and prosocial behaviors, across different developmental stages in childhood and adolescence. By incorporating these interactions, we aimed to understand how the impact of ACEs on these behaviors might vary by gender and age, providing a more nuanced analysis of these dynamics over time.
Additionally, we applied the GEE model, executed different correlation structures (i.e., independence, exchangeable, autoregressive, and unstructured), and applied the quadratic inference function (QIC) to choose the best correlation structure (Ballinger, 2004; Odueyungbo et al., 2008). The lower the QIC is (i.e., the exchangeable correlation structure has a lower QIC), the better the correlation structure for modeling. Finally, the study employed incidence ratios (IRs) along with 95 % confidence intervals (95 % CIs) to examine the relationships between exposure (i.e., ACEs) and outcomes (i.e., internalizing and externalizing behavior problems). A P value <0.05 was also considered to indicate statistical significance. In addition, a simple imputation technique was used to handle the missing data. All analyses were conducted using R software.
3. Results
3.1. Descriptive statistics
Table 1 provides the descriptive statistics for the variables analyzed in this study, which include 18,762 observations from wave 3 to wave 8. The findings of this study reveal that externalizing behaviors slightly increase with age: children aged 4–5 years exhibit a mean score of 4.8, which increases to 5.2 by the ages of 12–15 years. Internalizing behaviors show a more significant increase from an average of 2.4 in early childhood to 4.6 in adolescence with an overall mean of 3.6. Pro-social behaviors peak with a mean of 8.4 during the 8–9 year age range and subsequently decline to 7.4 by ages 12–15 years.
Table 1. Descriptive statistics of the study participants.
Variables under study | Wave 3 (aged 4–5 years) (n = 4386) Mean/percentage | Wave 5 (aged 8–9 years) (n = 4085) Mean/percentage | Wave 8 (aged 12–15 years) (n = 3127) Mean/percentage | Missing values (wave 3 – wave 8) (N = 18,762) Mean/percentage | Pooled (aged 4–15 years) (N = 18,762) Mean/percentage |
|---|---|---|---|---|---|
Outcome Variables | |||||
Externalizing behavior | 4.8 | 4.6 | 5.2 | 4.9 | – |
Internalizing behavior | 2.4 | 3.2 | 4.6 | 3.6 | - |
Pro-social behavior | 7.7 | 8.4 | 7.4 | 7.9 | 4.6 |
Key Independent variables (ACEs) | |||||
Physical punishment Yes | 87.9 | 89.2 | 89.2 | 83.7 | 4.0 |
Hostile parenting Yes | 7.2 | 10.6 | 9.4 | 9.4 | 3.3 |
Intra-parental conflict Yes | 5.8 | 7.2 | 7.0 | 6.7 | 17.7 |
Parental separation Yes | 1.8 | 4.4 | 4.0 | 3.9 | 1.5 |
Financial hardship Yes | 18.5 | 17.5 | 15.6 | 15.5 | 2.1 |
Parental legal issue | 1.5 | 3.3 | 2.0 | 2.5 | 3.9 |
Parental mental illness Yes | 3.1 | 2.6 | 4.1 | 3.3 | 3.5 |
Death of a family member Yes | 3.2 | 5.9 | 7.1 | 5.5 | 3.9 |
Parental drug use problem Yes | 1.2 | 2.8 | 3.7 | 2.6 | 3.9 |
Parental alcohol use Yes | 92.8 | 91.1 | 90.2 | 91.5 | 2.7 |
Demographic variables | |||||
Age in years | 4.3 | 8.5 | 14.3 | 9.4 | - |
Gender | |||||
Male | 51.3 | 51.1 | 51.4 | 51.3 | - |
Female | 48.7 | 48.9 | 48.6 | 48.7 | - |
Household income | |||||
Lowest Income | 19.3 | 10.9 | 6.7 | 12.9 | 5.4 |
Medium lowest income | 45.6 | 29.5 | 23.1 | 33.3 | – |
Medium highest income | 30.2 | 48.1 | 51.3 | 43.1 | – |
Highest Income | 5.0 | 11.5 | 18.9 | 10.6 | – |
Parent's education status | |||||
Postgraduation | 8.0 | 9.7 | 11.5 | 9.6 | – |
Undergraduate | 27.8 | 29.0 | 30.0 | 28.8 | – |
certificate/Diploma | 62.5 | 59.7 | 56.1 | 59.8 | 18.9 |
Year 12 or below | 1.8 | 1.6 | 2.4 | 1.8 | – |
Parent's employment status | |||||
Employed | 65.8 | 74.8 | 85.8 | 76.1 | 0.7 |
Unemployed | 1.9 | 3.0 | 2.0 | 2.5 | – |
Not in labor force | 32.3 | 22.2 | 12.3 | 21.4 | – |
Ethnicity | |||||
No, Aboriginal and Torres Strait Islander | 97.8 | 97.7 | 98.6 | 98.1 | 0.4 |
Yes, Aboriginal Torres Strait Islander | 2.2 | 2.3 | 1.4 | 1.9 | – |
Note: n = total number of child participants in a particular wave, N = person-years observation from wave 3 to wave 8. Lowest income = 500 AUD or less per week, medium lowest income 501 to 999 AUD per week, medium highest income = 1000 to 1999 AUD per week, highest income than 2000 AUD per week.
In terms of adverse childhood experiences (ACEs), physical punishment is highly prevalent across all age groups, as reported by >83 % of participants. It peaks at 89.2 % among 8–9-year-olds and slightly declines to 83.4 % among adolescents (aged 12–15 years). Hostile parenting and intraparental conflict, though less common, show an upward trend, increasing from 7.2 % to 9.4 % and from 5.8 % to 7.0 %, respectively. Reports of parental separation also increase with age, from 1.8 % to 4.4 %. Financial hardships are more prevalent in the youngest group at 18.5 % and decrease marginally in older age groups. The incidence of parental mental health issues and substance use varies, with over 90 % of cases involving alcohol use occurring across waves. Demographically, the sex distribution remained nearly balanced across all age groups. Household income tends to increase as children age, which is accompanied by increases in parental education and employment rates. Ethnicity data revealed that the majority of the study population was not aboriginal or Torres Strait Islander, showing minimal variations over time, as detailed in Table 1.
3.2. Longitudinal relationship between individuals' ACEs (aged 4 to 7 years) and externalizing, internalizing, and prosocial behaviors in childhood and adolescence (aged 4 to 15 years)
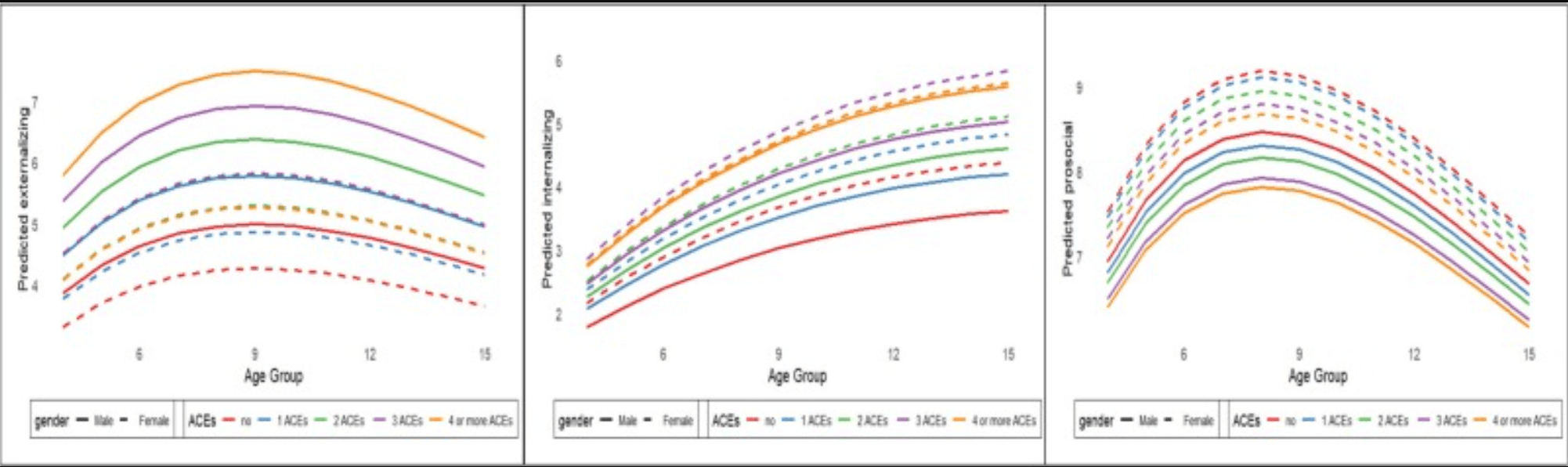
Table 2 presents the results of the longitudinal relationships between individual ACEs and externalizing, internalizing, and prosocial behaviors in adolescence. The findings of the study illustrate a noteworthy relationship wherein an increase of one unit of physical punishment, hostile parenting, intraparental conflict, financial hardship, parental mental health disorders, and parental substance abuse (e.g., alcohol and drug) significantly elevates the risk of externalizing and internalizing; however, it decreases prosocial behaviors among Australian youth (Table 2). Moreover, the study revealed that individuals exposed to ACEs exhibit gender-sensitive patterns in developing externalizing, internalizing, and prosocial behaviors. Specifically, the development of externalizing behavior in response to ACEs exposure seems more pronounced for male respondents than for their female counterparts. Similarly, it was found that externalizing problems increased with age from 4 to 8 years and declined after the age of 10 years. In contrast, female respondents exhibited a more pronounced increase in the intensity of internalizing and prosocial behaviors with each passing year (Fig. 1). Interestingly, the patterns of pro-social behaviors exhibit a distinctive trajectory with respect to ACEs score, age, and gender. As illustrated in Fig. 1, prosocial behavior tends to exhibit an upward trend from early childhood to middle childhood (i.e., aged 4 to 10 years). Unfortunately, after middle childhood, these increasing trends in prosocial behaviors were found to decrease. This indicates that the prosocial behaviors exhibited by young individuals tend to persist at relatively low and consistently lower levels from the ages of 10 to 15 years (Fig. 1). In summary, our findings underscore the profound impact of ACEs on the development of behavioral, emotional, and prosocial behavioral problems in childhood and adolescence.
Table 2. Longitudinal relationship between individuals' adverse childhood experiences (aged 4 to 7 years) and externalizing, internalizing, and prosocial behaviors in childhood and adolescence (aged 4 to 15 years).
Individual ACEs | Externalizing behavior problem Co-eff (SE) | Internalizing behavior problem Co-eff (SE) | Prosocial behavior Co-eff (SE) |
|---|---|---|---|
Physical punishment (Yes =1 | 0.06(0.02) ** | 0.28(0.03) *** | −0.01(0.01) *** |
Female* | −0.08(0.02) ** | 0.14(0.01) *** | 0.09(0.01) *** |
Hostile parenting (Yes =1) | 0.36 (0.02) *** | 0.28(0.03) *** | −0.08 (0.01) *** |
Female*hostile parenting | −0.16 (0.01) *** | 0.14(0.01) *** | 0.08(0.01) *** |
Intra-parental conflict (Yes =1) | 0.14(0.02) *** | 0.17(0.01) *** | −0.01(0.01) * |
Female* intra-parental conflict | −0.17 (0.01) *** | 0.12(0.01) *** | 0.09(0.01) |
Parental separation (Yes = 1) | 0.14 (0.03) *** | 0.23(0.01) *** | −0.03 (0.01) ** |
Female* separation | −0.17(0.01) *** | 0.13(0.01) *** | 0.08(0.01) *** |
Financial hardship (Yes = 1) | 0.09 (0.02) *** | 0.13(0.01) *** | −0.02 (0.01) ** |
Female*: Financial hardship | −0.17 (0.01) *** | 0.13(0.01) | 0.08(0.01) *** |
Parental legal issue (Yes = 1) | 0.13(0.01) *** | 0.19(0.04) *** | 0.03(0.01) |
Female* legal issue | −0.16(0.01) *** | 0.13(0.01) *** | 0.09(0.01) *** |
Parental mental health illness (Yes = 1) | 0.23 (0.03) *** | 0.36(0.04) *** | −0.06 (0.01) *** |
Female* mental health illness | −0.17(0.01) *** | 0.12(0.03) *** | 0.08(0.01) *** |
Death of a family member (Yes = 1) | 0.02 (0.02) | 0.05 (0.01) * | 0.02(0.01) |
Female* death of a family | −0.17(0.01) *** | 0.12(0.01) *** | 0.08(0.01) *** |
Parental drug use problem (Yes = 1) | 0.04 (0.03) * | 0.07 (0.032) | −0.04 (0.01) * |
Female* parental drug use problem | −0.17(0.01) *** | 0.13(0.01) *** | 0.08(0.01) *** |
Parental alcohol use problem (Yes = 1) | 0.09 (0.02) *** | −0.04 (0.02) | 0.02(0.01) * |
Female* parental alcohol | −0.23(0.03) | 0.15(0.04) ** | 0.1(0.01) *** |
Notes: P-values are on parenthesis; (2) ‘*’, ‘**’ and ‘***” indicate statistical significance at 10 %, 5 %, and 1 % levels.
Fig. 1. Externalizing, internalizing, and prosocial behaviors among participants aged 4 to 15, who have experienced 0, 1, 2, 3, and 4 or more ACEs.
3.3. Longitudinal relationship between ACEs (aged 4 to 7 years) and externalized, internalized, and prosocial behaviors in childhood and adolescence (aged 4 to 15 years)
Table 3 shows the longitudinal results of the relationships between adjusted and unadjusted ACEs scores and externalizing, internalizing, and prosocial behavior in childhood and adolescence. Table 3. Longitudinal relationship between adverse childhood experiences (aged 4 to 7 years) and externalizing, internalizing, and prosocial behaviors in childhood and adolescence (aged 4 to 15 years).
Variables | Externalizing behaviors | Externalizing behaviors | Internalizing behaviors | Internalizing behaviors | Prosocial behavior | Prosocial behavior |
|---|---|---|---|---|---|---|
Crude IR With 95 % CI | Adjusted IR With 95 % CI | Crude IR With 95 % CI | Adjusted IR With 95 % CI | Crude IR With 95 % CI | Adjusted IR With 95 % CI | |
Adverse childhood experiences | ||||||
No ACEs (Ref = 1) | 1 | 1 | 1 | 1 | 1 | 1 |
1 ACEs | 1.69(1.49–1.92) | 1.69(1.48–1.92) | 1.50(1.26–1.77) | 1.49(1.26–1.77) | 0.99(0.95–1.02) | 0.98(0.97–0.99) |
2 ACEs | 2.14(1.83–2.50) | 2.12(1.81–2.48) | 2.13(1.72–2.64) | 2.07(1.67–2.56) | 0.93(0.89–0.98) | 0.97(0.96–0.99) |
3 ACEs | 2.52(2.03–3.13) | 2.50(2.02–3.10) | 3.24(2.41–4.34) | 3.17(2.37–4.25) | 0.94(0.86–1.03) | 0.95(0.93–0.98) |
4 or more ACEs | 3.41(2.40–4.84) | 3.34(2.37–4.73) | 4.18(2.61–6.68) | 4.12(2.59–6.54) | 0.96(0.83–1.10) | 0.94(0.91–0.97) |
Gender (ref: Male) | 1 | 1 | 1 | 1 | 1 | 1 |
1 ACEs*Female | 0.98(0.94–1.03) | 0.99(0.94–1.03) | 1.24(1.18–1.27) | 1.25(1.19–1.31) | 1.01(1.00–1.03) | 1.01(1.0–1.03) |
2 ACEs*Female | 0.97(0.91–1.03) | 0.97(0.91–1.03) | 1.29(1.19–1.33) | 1.31(1.15–1.38) | 1.01(0.99–1.03) | 1.01(0.99–1.03) |
3 ACEs*Female | 0.97(0.89–1.05) | 0.96(0.89–1.05) | 1.47(1.43–1.55) | 1.45(1.36–1.55) | 1.01(0.98–1.04) | 1.01(0.98–1.04) |
4 or more ACEs * Female | 0.83(0.72–0.95) | 0.83(0.72–0.95) | 1.81(1.71–1.89) | 1.83(1.78–1.92) | 1.03(0.99–1.08) | 1.03(0.99–1.08) |
1 ACEs *age | 0.84(0.80–0.89) | 0.84(0.80–0.891) | 1.52(1.48–1.59) | 1.49(1.43–1.56) | 1.00(0.98–1.02) | 1.00(0.98–1.02) |
2 ACEs *age | 0.79(0.74–0.85) | 0.79(0.74–0.84) | 1.70(1.63–1.87) | 1.69(1.61–1.88) | 1.02(1.00–1.04) | 1.02(1.0–1.04) |
3 ACEs*age | 0.77(0.70–0.84) | 0.764(0.69–0.84) | 1.79(1.69–1.89) | 1.80(1.73–1.98) | 1.01(0.97–1.05) | 1.01(0.97–1.05) |
4 or more ACEs *age | 0.69(0.59–0.81) | 0.69(0.59–0.81) | 1.86(1.81–2.29) | 1.84(1.79–2.28) | 0.99(0.93–1.06) | 0.99(0.93–1.06) |
Note: Childhood = age 4–5 years; Middle childhood = 6–11 years; and Adolescence = 12–15 years, IR = Incidence ratio. These specifications are adjusted for gender, ethnicity, and parental education.
3.3.1. ACEs scores and externalizing behaviors
In the context of ACEs scores and externalizing behavior problems, this study revealed that children and adolescents who had been exposed to one ACEs exhibited a greater risk of developing externalizing behavior problems (adjIR = 1.69, 95 % CI = 1.48–1.92) than did their counterparts without any ACEs exposure. In a similar vein, those who experienced at least four or more ACEs experienced a substantial threefold increase in the risk of external behavior problems (adjIR = 3.34, 95 % CI = 2.37–4.73) compared with their counterparts who had not encountered ACEs. Notably, the risk of developing externalizing behavior issues was significantly lower in the female cohort than in the male cohort (Table 3).
3.3.2. ACEs scores and internalizing behaviors
This study highlights a significant relationship between exposure to ACEs and an increased risk of developing internalizing behavior in children and adolescents. It is worth mentioning that young individuals who had experienced one ACEs during their developmental periods of life had a significantly increased likelihood of displaying internalizing behavior problems (adjIR = 1.49, 95 % CI = 1.26–1.77), which is in striking contrast to those who had not encountered ACEs. Moreover, following up on this significant relationship, individuals who experienced four or more ACEs exhibited a substantial increase in developing internalizing behaviors (adjIR = 4.12, 95 % CI = 2.59–6.54) compared to their peers who had not been exposed to ACEs. Interestingly, the study revealed that girls exhibited a greater risk of developing internalizing behavior problems than did boys over the observed periods (Table 3).
3.3.3. ACEs scores and prosocial behaviors
Regarding ACEs scores and prosocial behaviors, this study revealed a significant link between exposure to ACEs and the manifestation of prosocial behavior in children and adolescents. The study revealed that individuals who were exposed to one ACEs exhibited a lower likelihood of developing prosocial behaviors (adjIR = 0.98, 95 % CI = 0.97–0.99) than did their counterparts who had not encountered ACEs. Furthermore, a parallel and equally robust pattern emerges among individuals who have endured four or more ACEs, underscoring a continuous decline in engaging in prosocial behavior (adjIR 0.94, 95 % CI = 0.91–0.97) in comparison to those who had no ACEs exposure. Surprisingly, our findings revealed that girls exhibited significantly greater levels of prosocial behavior than did their male counterparts (Table 3).
3.4. Analysis of the latent class and ACEs
The LCA was ineffective on this dataset due to the exceptionally low entropy level. These low entropy values indicated a significant challenge in distinguishing between various ACEs reporting groups. Therefore, our ability to conduct further analysis of associations within the LCA-derived clusters in the context of this study was considerably impeded.
3.5. Robustness tests
The present study has undergone several analyses to assess its robustness. This study specifically examined the cross-sectional relationship between ACEs during childhood (i.e., age 4 to 8 years) and externalizing, internalizing, and prosocial behaviors in adolescents (i.e., age 15 years) (online appendix Table 2). The robustness test shows that early-life exposure to ACEs plays a pivotal role in determining behavioral, emotional, and prosocial challenges among young people, which is consistent with our main findings, confirming that our main findings are both generalizable and robust.
4. Discussion
Adverse childhood experiences profoundly influence the lives of children and adolescents and serve as robust predictors of psychopathological outcomes across their lifespan (Gilbert et al., 2009; Henry et al., 2021; McGrath et al., 2017). Considering the significant consequences of ACEs, it is important to understand the complex mechanism of the association between ACEs and the risk of developing externalizing, internalizing, and prosocial behavior in a cohort of children and adolescents. Therefore, the present study hypothesized that children and adolescents who had poor childhood experiences would exhibit greater externalizing, internalizing, and low prosocial behavior. Three methods were utilized to define ACEs individual ACEs, ACEs scores, and cluster ACEs through the application of latent class analysis.
In line with our first hypothesis, our findings revealed a significant relationship between higher ACEs scores and increased externalizing and internalizing behaviors compared to their peers. This finding aligns with existing research showing that a greater number of ACEs is associated with an elevated risk of externalizing and internalizing behaviors, such as aggression and emotional difficulties (Bevilacqua et al., 2021; Hunt et al., 2017; Qu et al., 2023). Furthermore, our study demonstrated that a greater number of ACEs during childhood and adolescence increased the risk of poor prosocial behaviors. This suggests that ACEs may model negative behaviors and low self-esteem, disrupting decision-making and impulse control and thereby contributing to a propensity for risky and antisocial activities among children and adolescents. Our findings are consistent with previous research that links adverse adoptive home environments, including poor parental practices, parental mental illness, parental separation, and financial hardship, to a decline in prosocial behaviors (Álvarez-García et al., 2019; Otto et al., 2021; Piotrowska et al., 2019). Recent research has also emphasized the role of family characteristics, including prosocial behaviors, in children's and adolescents' mental health (Evans-Whipp and Rowland, 2023).
Additionally, our study investigated gender differences in the relationships between ACEs scores and externalizing, internalizing, and prosocial behaviors. We found distinct gender patterns, with boys more likely to exhibit externalizing problems and girls showing a greater inclination toward internalizing and prosocial behaviors. These differences are influenced by biological, socialization, and coping factors and align with previous studies (Chaplin and Aldao, 2013; Eschenbeck et al., 2007; Godinet et al., 2014; Kring and Gordon, 1998). Therefore, externalizing behavior is often an extreme response associated with ACEs being significantly more prevalent among boys, whereas emotional and prosocial behaviors are more prevalent among girls (Leban, 2021).
Our study revealed that physical punishment significantly increased the risk of externalizing behaviors, while hostile parenting, parental mental health issues, and financial hardship had the most pronounced impact on externalizing, internalizing, and prosocial difficulties. The literature also reports that the use of physical punishment in children is linked to a subsequent increase in externalizing behaviors. These behaviors can be identified by outward manifestations such as aggression, delinquency and criminality issues, which have detrimental impacts on a child's and adolescent's surroundings (Farrington and Hawkins, 1991; Gershoff, 2002; Heilmann et al., 2021). Hence, physical punishment is associated with adjustment problems and aggressive behaviors in children and adolescents (Gershoff, 2002).
On the other hand, hostile parenting, parental mental health problems, and financial hardship significantly exhibited the most pronounced influence on externalizing, internalizing, and prosocial difficulties. Inconsistent caregiving, discipline, and boundaries can lead to confusion in children. Similarly, parents with psychological problems can exhibit negative parenting behaviors, neglect of children's needs, and increased household dysfunction. These consequences may affect children's behavioral, emotional, and social interactions and potentially contribute to behavioral, emotional and social challenges. The literature has shown that an adverse childhood family environment has been linked to a heightened risk of externalizing, internalizing, and prosocial difficulties in children and adolescents (Aunola and Nurmi, 2005; Boden et al., 2010; Fuentes-Balderrama et al., 2020; Meadows et al., 2007; Schepman et al., 2011; Williams and Cheadle, 2016). Hence, the relationships among these factors may contribute to the emergence of externalizing, internalizing, and prosocial difficulties in adolescents who persist throughout adulthood. Therefore, the findings highlight the importance of consistent caregiving, discipline, and boundaries for child development and emphasize the need for interventions to address ACEs and their consequences. In summary, this study contributes to the literature by exploring the longitudinal relationship between ACEs and the risk of externalizing, internalizing, and prosocial behaviors in children and adolescents. The results highlight the correlation between physical punishment, hostile parenting, and household dysfunction with these behaviors, suggesting the need for multisectoral intervention programs (clinical, community, parenting, home visit, economic and social services, psychological, and school-based programs) to address ACEs and their outcomes. These programs should prioritize enhancing social competencies and promoting familial functionality and cohesion, especially for children whose parents are facing financial hardship and mental health disorders. However, due to the unavailability of original ACEs measurement (e.g., physical and emotional neglect, sexual abuse, and the incarceration of family members) in the LSAC dataset, this study adapted ACEs measurement available in LSAC. Therefore, the implications of these omissions and modifications might impact the measurement of outcomes and constrain the broader applicability and generalizability of the study's findings. Despite the constraints posed by the available ACEs measurement in LSAC, we successfully demonstrated robust construct validity.
4.1. Strength and limitations
This study effectively utilized a substantial contemporary national longitudinal dataset from Australia to explore the relationships between ACEs and externalizing, internalizing, and prosocial behaviors among children and adolescents; this study is not exempt from certain limitations. First, the presence of unbalanced longitudinal data stems from variations in the number of observations across different time points, which indeed poses challenges for drawing robust inferences. Second, the presence of missing data points for the study variables across multiple waves could impact the study's findings. Third, there might be a chance of potential bias because respondents may not accurately remember past events or details, which is especially relevant in studies that ask about past ACEs. Fourth, the use of adapted ACEs measurements in the LSAC may have limited the generalizability of the findings. Finally, a limited representation of Aboriginal Australians lacks the generalizability of the findings and may not fully capture the experiences or conditions pertinent to Aboriginal Australian communities. Despite this limitation, this research provides valuable insights into the determinants of externalizing, internalizing, and prosocial behavioral problems among Australian youth.
5. Conclusion
This study offers robust insights into individual ACEs and ACEs scores, shedding light on their relationships with externalizing, internalizing, and prosocial behaviors in Australian children and adolescents. Our findings underscore that ACEs serve as significant predictors for the development of behavioral, emotional, and social issues during childhood and adolescence. These results have profound implications for both clinical practice and policymaking. Recognizing the frequency and nature of stressors experienced by children and adolescents at an early age is crucial for anticipating their mental health trajectories. Subsequently, appropriate intervention initiatives, such as parenting programs, economic and social services, psychological therapies, school-based programs, and community-based support, can be tailored to their specific needs. Our study aligns with the calls from child advocates, emphasizing the importance of banning or eliminating physical punishment, promoting positive parenting styles, and implementing comprehensive health and economic programs within families and communities. By heeding these calls, we can better safeguard the rights and well-being of our youth, paving the way for healthier and happier futures.